



Topic Resources

Most women with genito-pelvic pain/penetration disorder are anxious about and cannot tolerate insertion of any object into the vagina (such as from sexual intercourse, a tampon, or a pelvic examination).
Women may develop this disorder after experiencing painful intercourse (due to vaginal dryness or sexual trauma), or there may be no known cause.
Doctors diagnose genito-pelvic pain/penetration disorder based on symptoms, a pelvic examination, and specific criteria.
Lubricants, topical anesthetic (numbing) gels, exercises to relax pelvic muscles, exercises to make women feel comfortable with vaginal contact by themselves or their partner, or pelvic physical therapy may help.
(See also Overview of Sexual Dysfunction in Women.)
Pain during intercourse may occur in the
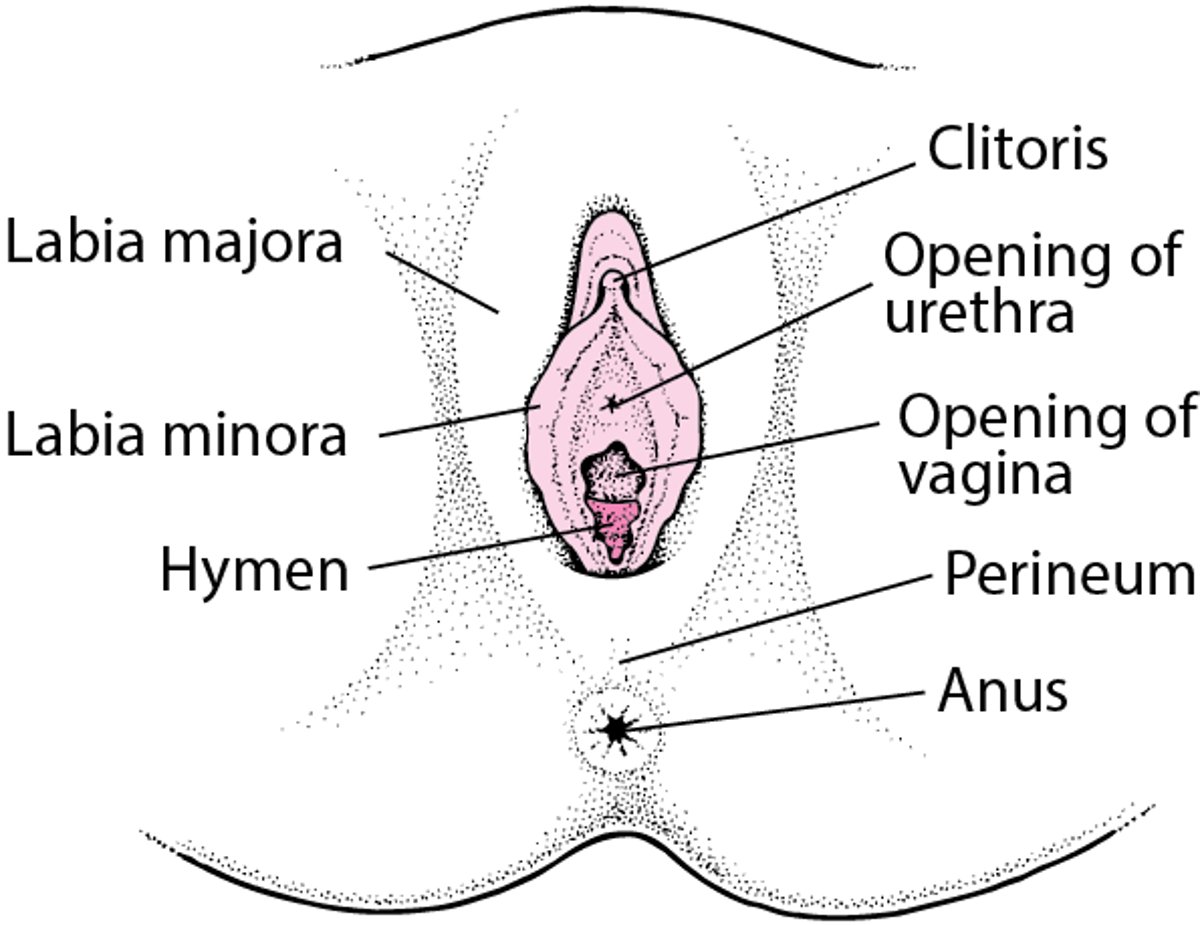
Vulva (the external female genitals, including the labia, clitoris, and opening of the vagina), called provoked vestibulodynia: Occurring when the vulva is touched, even with light pressure
Vagina, called dyspareunia: Occurring when something is inserted into the vagina
Abdomen (belly), called deep dyspareunia: Occurring in the abdomen when something is inserted into the vagina
The pain may be burning, sharp, or cramping. Pelvic muscles tend to become tight, which increases the pain, whether it is superficial or deep.
In genito-pelvic pain/penetration disorder, muscles around the opening of vagina tighten involuntarily when a woman thinks about or tries to have sexual intercourse (or any vaginal insertion, such as during a pelvic examination).
Many women with genito-pelvic pain/penetration disorder also have difficulty becoming aroused and/or difficulty reaching orgasm.
External Female Reproductive Anatomy

Causes of Genito-Pelvic Pain/Penetration Disorder
Causes of genito-pelvic pain/penetration disorder vary depending on whether the pain is superficial or deep.
Vulvar pain
Vulvar pain may result from the following:
Increased sensitivity of the genital area to pain (as may occur in provoked vestibulodynia)
Breastfeeding, which can cause dryness of the vagina because estrogen levels are low
Genitourinary syndrome of menopause (changes in the vagina and urinary tract that can occur at menopause)
Inadequate lubrication from insufficient foreplay
Inflammation or infection in the genital area (including genital herpes and yeast infections) or Bartholin glands (the small glands on either side of the vaginal opening)
An allergic reaction to contraceptive foams or jellies or to latex condoms
Inflammation or infection of the urinary tract
Injuries in the genital area
A history of sexual trauma
Use of antihistamines, which can cause slight, temporary dryness of the vagina
Radiation therapy affecting the vagina, which can make the vagina less elastic and can cause scarring, making the area around the vagina narrower and shorter
Genitourinary syndrome of menopause refers to changes in the vagina and urinary tract that occur after menopause. Tissues of the vagina can become thin, dry, and have difficultly stretching, and lubrication for intercourse is inadequate. These changes occur because estrogen levels decrease after menopause. These changes can make intercourse painful. Urinary symptoms that can occur at menopause include a compelling need to urinate (urinary urgency) and frequent urinary tract infections.
Provoked vestibulodynia (pain of an area at the opening of the vagina, called the vulvar vestibule) may be present the first time something (such as a tampon, speculum, or penis) is inserted into the vagina (penetration). Or it may develop in a woman who has experienced comfortable, pain-free penetration. Vestibulodynia may result from a combination of factors, including the following:
Inflammation or an immune reaction (which may result from contact with an irritating substance, a contact irritant, an infection or a medication)
An increased number of nerve fibers (which is sometimes present at birth), making the area more sensitive to pain
Menopause or other causes of decreased production of estrogen
Problems with the pelvic floor muscles (muscles that are located in the low in the pelvis and that support organs in the pelvis, including the vagina)
Provoked vestibulodynia can occur in chronic pain syndromes, including fibromyalgia, interstitial cystitis, and irritable bowel syndrome. Also, certain connective tissue disorders (such as Ehlers-Danlos syndrome) increase the risk of having provoked vestibulodynia.
Vaginal pain
Vaginal pain during or after sexual intercourse may result from the following:
Vaginitis (bacterial vaginosis, yeast infections, or trichomonal infection)
Rarely, an abnormality present at birth (such as an abnormal partition within the vagina) or a hymen that interferes with entry of the penis
Surgery that narrows the vagina (for example, to repair tissues torn during childbirth or to correct pelvic organ prolapse)
Levator ani syndrome (previously called vaginismus)
Myofascial pain (pain that is caused by tension and tenderness in areas of muscle called trigger points)
Growths in the pelvis (such as tumors and ovarian cysts)
Bands of scar tissue (adhesions) between organs in the pelvis, which may form after an infection, surgery, or radiation therapy for cancer in a pelvic organ (such as the bladder, uterus, cervix, fallopian tubes, or ovaries)
The term levator ani syndrome has largely replaced the term vaginismus because symptoms of vaginismus typically result from levator ani muscle dysfunction. Levator ani syndrome is involuntary contraction of the levator ani, which is the main pelvic floor muscle. This disorder may result from fear that intercourse will be painful. It often begins when sexual intercourse is first attempted but may develop later after periods of stress or experiences of painful sex or trauma. If women fear sex will be painful, their pelvic muscles may automatically tighten whenever intercourse is anticipated or attempted.
The hymen is a membrane that encircles or, in a very few women, covers the opening of the vagina. When women have sexual intercourse the first time, the hymen, if not previously stretched (for example, from tampon use or sexual stimulation with a finger inside the vagina), may tear, causing some pain and bleeding. A few women are born with an abnormally tight hymen.
Deep abdominal pain
Pain deep in the abdomen during or after sexual intercourse may result from the following:
Infection of the cervix, uterus, or fallopian tubes (pelvic inflammatory disease), which may cause collections of pus (abscesses) to form in the pelvis
Myofascial pain
Growths in the pelvis (such as tumors and ovarian cysts)
Bands of scar tissue (adhesions) between organs in the pelvis, which may form after an infection, surgery, or radiation therapy for cancer in a pelvic organ (such as the bladder, uterus, cervix, fallopian tubes, or ovaries)
The cause of deep abdominal pain during sex is treated, if possible. This may be with antibiotics for pelvic infection or surgery for endometriosis or uterine fibroids.
Symptoms of Genito-Pelvic Pain/Penetration Disorder
The pain of genito-pelvic pain/penetration disorder may first occur when something (tampon, speculum, or penis) is inserted into the vagina. Or a woman may never have had pain-free sexual intercourse. For example, the pain may occur even if she has not had sexual pain in the past. The pain is often described as burning or stabbing.
Women with genito-pelvic pain/penetration disorder may have an intense fear of and anxiety about pain before or during penetration of the vagina. When women anticipate that pain will recur during penetration, their vaginal muscles tighten, making attempts at sexual intercourse even more painful.
The inability to have sexual intercourse is stressful for a woman and can cause relationship stress with a partner. It causes significant stress for a woman who wants to become pregnant.
Diagnosis of Genito-Pelvic Pain/Penetration Disorder
Doctor's evaluation, based on specific criteria
Doctors diagnose genito-pelvic pain/penetration disorder based on the woman’s description of the problem, including when and where the pain is felt, and on the results of a pelvic examination. The pelvic examination can detect or rule out physical abnormalities.
If a woman has a history vaginal pain, the anticipation of pain and involuntary contraction of muscles around the vagina's opening can make it difficult to have a pelvic examination. This can be discussed with the doctor before the examination. Some strategies for making a pelvic examination more tolerable are as follows:
A woman and her doctor can discuss the examination before it begins and agree on how to communicate during the examination.
A woman can hold a mirror to be able to see what the doctor sees during the examination and allow the doctor to show her any issues that are detected.
A woman can place her hand on the doctor’s hand to have a greater sense of control during the examination.
The area in and around the opening of vagina is examined for possible causes, such as signs of inflammation or abnormalities.
To determine where the pain occurs, a doctor may use a cotton swab to touch different areas around and/or in the vagina.
Doctors may also press on the urethra and bladder to check for tenderness.
The doctor assesses the tightness of the pelvic muscles around the vagina by inserting one or two gloved fingers into the vagina. To check the uterus and ovaries for abnormalities, the doctor then places the other hand on the lower abdomen (called a bimanual examination) and presses on these organs.
A rectal examination may also be done.
Doctors diagnose genito-pelvic pain/penetration disorder based on criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), published by the American Psychiatric Association. These criteria require the presence of at least one of the following:
Significant pain during intercourse or penetration attempts
Significant fear or anxiety about pain in anticipation of, during, or because of vaginal penetration
Significant tensing or tightening of the pelvic muscles during attempts to penetrate the vagina
These symptoms must have been present for at least 6 months and must cause significant distress in the woman. Also, doctors must rule out any other cause of the symptoms, such as another disorder, sexual trauma, or medication or other substance.
Treatment of Genito-Pelvic Pain/Penetration Disorder
Treatment of the cause of the pain, if possible
Lubricants, sometimes anesthetic (numbing) gels
Pelvic floor physical therapy
Sometimes psychotherapy
Treatment may involve a team of clinicians, such as doctors, physical therapists, psychotherapists, and sex therapists.
Which treatments for genito-pelvic pain/penetration disorder are best has not been determined, and treatments vary depending on symptoms. However, some general measures are recommended.
General measures
Vaginal lubricants and moisturizers include food-based oils (such as coconut oil), silicone-based lubricants, and water-based products. Water-based lubricants dry out quickly and may have to be reapplied, but they are preferred over petroleum jelly or other oil-based lubricants. Oil-based lubricants tend to dry the vagina and can damage latex contraceptive devices such as condoms and diaphragms. They should not be used with condoms. Silicone-based lubricants can be used with condoms and diaphragms, as can water-based lubricants. Women can ask their doctor which type of lubricant would be best for them.
General measures for vaginal health include wearing cotton underwear, possibly wearing no underwear while sleeping, washing only with water or a mild soap, and not douching or using over-the-counter vaginal deodorants.
When treating genito-pelvic pain/penetration disorder, doctors or other team members often do the following:
Encourage a woman or couple to develop satisfying forms of sexual activities that do not involve penetration and teach how to do it
Discuss emotional issues contributing to and caused by the chronic pain
When possible, treat any physical abnormality that contributes to pain (such as endometriosis or vaginal infections)
Treat involuntary contraction of the muscles in the pelvis (pelvic muscle hypertonicity)
Treat sexual interest/arousal disorders if also present
Sexual activities that do not involve penetration can help couples attain mutual pleasure (including having orgasms and ejaculation). An example is stimulation involving the mouth, hands, or a vibrator.
Spending more time in foreplay may increase vaginal lubrication and thus make intercourse less painful.
For deep pain, using a different position for intercourse may help. For example, being on top can give women more control of penetration, or another position may limit the depth of penetration.
Pelvic floor physical therapy
Pelvic floor physical therapy can often benefit women with genito-pelvic pain/penetration disorder. It includes pelvic floor muscle training, sometimes with biofeedback, to teach women how to consciously relax their pelvic muscles.
Physical therapists may use other techniques to improve the function of the pelvic muscles. Techniques include
Soft-tissue mobilization and myofascial release: Using various movements (such as rhythmic pushing or massage) to apply pressure on and stretch the affected muscles or the tissues that cover muscles (myofasciae)
Trigger-point pressure: Applying pressure to very sensitive areas of the affected muscles, which may be where the pain starts (trigger points)
Electrical stimulation: Applying gentle electric current through a device positioned at the opening of the vagina
Bladder training and bowel retraining: Having women follow a strict schedule for urination and recommending exercises to strengthen the muscles around the urethra and anus, sometimes with biofeedback
Therapeutic ultrasonography: Applying high-frequency sound waves to the affected muscles (increasing blood flow, enhancing healing, and making tight muscles less tight)
Levator ani syndrome (vaginismus) can be treated with progressive desensitization (done by hand or with dilators). This technique enables women to gradually get used to the genital area being touched. The next step is taken only when the woman is comfortable with the previous step.
The woman touches herself daily as close to the vagina's opening as possible. Once her fear and anxiety due to touching her genitals has decreased, the woman will be more able to tolerate the physical examination.
The woman inserts her finger past her hymen. She is instructed to push or bear down as she inserts her finger to enlarge the opening and ease entry into the vagina.
She inserts specially designed dilators gradually increasing sizes. Leaving a dilator inside for 10 to 15 minutes helps the muscles get used to gently increasing pressure without automatically contracting. After she can tolerate the smallest size, she inserts the next larger and so on.
The woman allows her partner to help her insert a dilator during a sexual encounter to confirm that it can go in comfortably when she is sexually excited.
The woman should allow her partner to touch the area around the vagina's opening with his penis or a dildo but without its entering the vagina. Then the woman can get used to feeling the penis or dildo on this area.
Eventually, the woman inserts her partner’s penis or a dildo partially or fully in the vagina in the same way that she placed the dilator. She may feel more confident if she is on top during intercourse.
For superficial pain, pelvic floor physical therapy is key because involuntary contraction of the muscles around the vagina's opening is often part of the problem. Liberally applying a lubricant before intercourse may help. Sometimes doctors suggest applying an anesthetic gel.
Psychological therapies
Psychological therapies, such as cognitive-behavioral therapy and mindfulness-based cognitive therapy, may benefit some women. Mindfulness involves focusing on what is happening in the moment, without making judgments about or monitoring what is happening. Such therapies may help a woman manage fear and anxiety about pain during sexual intercourse.
Doctors may refer women to a psychotherapist, couples therapist, or a qualified sex therapist for psychological therapies.
Specific therapies
More specific treatment depends on the cause, as in the following:
Thinning and drying of the vagina after menopause: Estrogen or DHEA (dehydroepiandrosterone) inserted into the vagina
Vaginal infections: Antibiotics or antifungal medications, as appropriate
Cysts or abscesses: Surgical removal
An abnormality of the hymen or other congenital abnormality: Surgery to correct it
Vaginal hormone therapy includes low-dose estrogen (as a cream, tablet, or ring or DHEA (as a suppository). Estrogen may be taken by mouth or applied to the skin in a patch or gel, but these forms of estrogen affect the whole body and are usually only used if a woman also has other symptoms of menopause (such as hot flashes).
Ospemifene (a selective Ospemifene (a selectiveestrogen receptor modulator, or SERM) and estrogen affect vaginal tissues in a similar way. Like estrogen, ospemifene can be used to relieve vaginal dryness and other symptoms that involve the vagina and/or urinary tract.receptor modulator, or SERM) and estrogen affect vaginal tissues in a similar way. Like estrogen, ospemifene can be used to relieve vaginal dryness and other symptoms that involve the vagina and/or urinary tract.
Medications used to treat neuropathic pain (pain due to damage of the nervous system) can help lessen the pain in provoked vestibulodynia. They include the antiseizure medications gabapentin and pregabalin and the antidepressants amitriptyline and nortriptyline.(pain due to damage of the nervous system) can help lessen the pain in provoked vestibulodynia. They include the antiseizure medications gabapentin and pregabalin and the antidepressants amitriptyline and nortriptyline.
Various creams that contains gabapentin and amitriptyline can be applied directly to the vagina's opening. These treatments may help relieve the pain and have fewer side effects.Various creams that contains gabapentin and amitriptyline can be applied directly to the vagina's opening. These treatments may help relieve the pain and have fewer side effects.
Botulinum toxin type A, injected into the pelvic floor muscles, is usually used only to treat provoked vestibulodynia when no other treatments have been effective. It is used only for a short period of time.
Vestibulectomy (removal of the area around the vagina's opening) is rarely done. It is usually done in women who have never had pain-free sexual intercourse.
Drugs Mentioned In This Article






