



Abnormal uterine bleeding (AUB) in patients of reproductive age is a bleeding pattern that is not consistent with normal menstrual cycle parameters (frequency, regularity, duration, and volume). The PALM-COEIN system classifies causes of AUB as structural (Polyp, Adenomyosis, Leiomyoma [fibroid], or Malignancy or hyperplasia) or nonstructural (Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, Not yet classified). Evaluation is with menstrual history, pelvic examination, hormone blood tests, and usually transvaginal ultrasonography. Treatment depends on cause but may include nonhormonal or hormonal medications or a procedure (eg, hysteroscopy, myomectomy, hysterectomy).
Topic Resources



(See also Vaginal Bleeding.)
Abnormal uterine bleeding (AUB) is a common issue. Ovulatory dysfunction (anovulation or oligo-ovulation) is the most common cause of AUB in women of reproductive age and occurs most often in women > 45 years old (> 50% of cases) and in adolescents (20% of cases).
Pathophysiology of AUB
During an anovulatory cycle, estrogen is produced, but the corpus luteum does not form. Thus, the normal cyclical secretion of progesterone does not occur, and estrogen stimulates the endometrium unopposed. Without opposition by progesterone, the endometrium continues to proliferate, eventually outgrowing its blood supply; it then sloughs incompletely and bleeds irregularly and sometimes profusely or for many days. When this abnormal process occurs repeatedly, the endometrium can become hyperplastic, sometimes with atypical or cancerous cells.
When abnormal uterine bleeding occurs in patients with ovulatory cycles, progesterone secretion is prolonged; irregular shedding of the endometrium results, probably because estrogen levels remain low, near the threshold for bleeding (as occurs during menses). In women with obesity, ovulatory AUB can occur if estrogen levels are high, resulting in amenorrhea alternating with irregular or prolonged bleeding.
Complications
Chronic heavy or prolonged uterine bleeding may cause iron deficiency anemia.
If AUB is due to ovulatory dysfunction, infertility may also be present.
Etiology of AUB
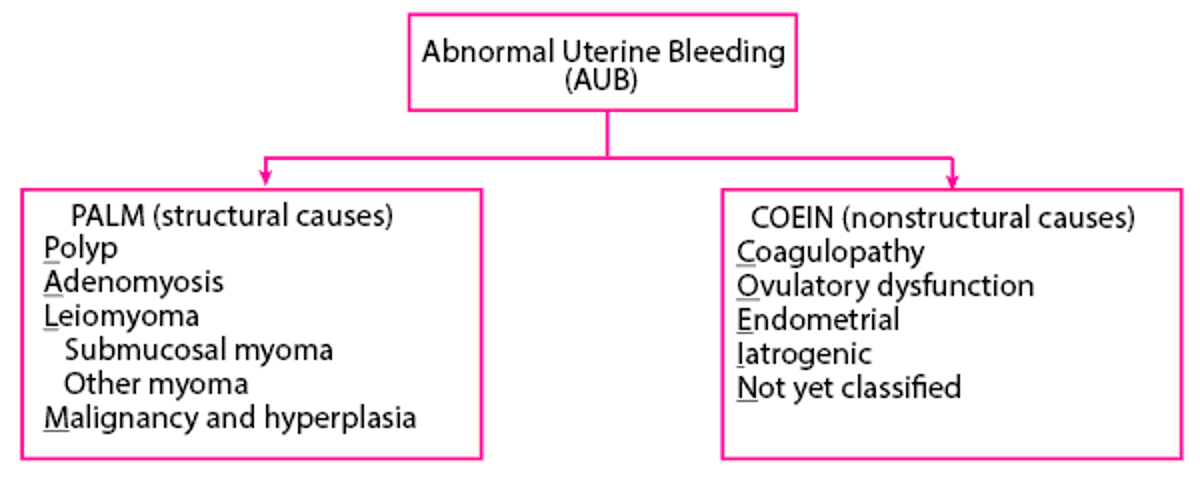
Causes of AUB in nonpregnant women of reproductive age may be classified as structural or nonstructural to aid in identification of the cause and guide treatment. The PALM-COEIN classification system may be used (1). PALM-COEIN is a mnemonic for the structural causes (PALM) and nonstructural (COEIN) causes of abnormal bleeding (see figure PALM-COEIN classification system).
PALM-COEIN classification system

AUB due to ovulatory dysfunction (AUB-O) is the most common type of nonstructural AUB and the most common cause overall. AUB-O can result from any disorder or condition that causes anovulation or oligo-ovulation (irregular or infrequent ovulation—see table Some Causes of Ovulatory Dysfunction). Causes of ovulatory dysfunction include
Hyperprolactinemia
Perimenarche or perimenopause
Idiopathic (sometimes occurring when gonadotropin levels are normal)
During perimenopause, AUB-O may be an early sign of ovarian insufficiency; follicles are still developing but, despite increasing levels of follicle-stimulating hormone (FSH), do not produce enough estrogen to trigger ovulation.
Approximately 20% of women with endometriosis have AUB-O due to unknown mechanisms. Other causes are a short follicular phase and luteal phase dysfunction (due to inadequate progesterone stimulation of the endometrium); a rapid decrease in estrogen before ovulation can cause spotting.
Other causes of ovulatory dysfunction are systemic disease (eg, liver or kidney disease, Cushing syndrome). Significant physical or emotional stress or poor nutrition are typical causes of hypothalamic amenorrhea, but some patients have oligo-ovulation and, thus, oligomenorrhea. In some cases, AUB-O is idiopathic (sometimes occurring when gonadotropin levels are normal).
Other nonstructural causes of AUB include
Coagulopathy
Endometrial factors (eg, endometritis)
Iatrogenic (eg, breakthrough bleeding on hormonal contraceptives)
Structural types of AUB include
Cervical or endometrial polyps
Adenomyosis
Leiomyoma (uterine fibroids)
Uterine or cervical cancer
Etiology reference
1. Munro MG, Critchley HOD, Fraser IS, FIGO (International Federation of Gynecology and Obstetrics) Menstrual Disorders Committee: The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet 143 (3):393–408, 2018. doi: 10.1002/ijgo.12666
Symptoms and Signs of AUB
Compared with typical menses, abnormal uterine bleeding may do the following (see table Normal Menstrual Parameters [1])
Occur more frequently (menses < 24 days apart)
Be irregular (cycle frequency varies ≥ 8 to 10 days)
Involve more days of bleeding (> 8 days)
Involve increased volume of blood loss (> 80 mL [or by patient report of volume]) during menses (heavy menstrual bleeding)
Occur between menses (intermenstrual bleeding)
Normal Menstrual Parameters*
Parameters | Normal Values | Notes |
|---|---|---|
Frequency | ≥ 24 to ≤ 38 days | Cycle length is defined as the number of days from first day of one menstrual period to first day of the next. |
Regularity | ≤ 7 to 9 days | Regularity is defined as variation of cycle frequency between the shortest and longest cycles. |
Duration | ≤ 8 days of bleeding per cycle | — |
Volume of bleeding | < 80 mL Clinically, patient's description of bleeding as normal volume | Clinically, precise measurement bleeding volume is not feasible. Assessment of bleeding volume is based on the patient's description (light, normal, heavy). Clinicians sometimes estimate by asking how many pads or tampons are saturated over time (heavy bleeding is likely if patients saturate a pad or tampon within 3 hours or less and/or if they pass blood clots larger than 1 inch [2.5 cm] in diameter). |
* Based on Munro MG, Critchley HOD, Fraser IS for the FIGO (International Federation of Gynecology and Obstetrics) Menstrual Disorders Committee): The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years. | ||
Patients with ovulatory cycles usually have menstrual cycles that are occur at a normal frequency and are regular, but they may have heavy menstrual bleeding or intermenstrual bleeding. Symptoms that suggest a patient has ovulatory cycles include molimina (eg, cyclic breast tenderness, premenstrual bloating, or mood changes) and midcycle cramping pain (mittelschmerz). Daily body temperature (basal body temperature) increases slightly after ovulation and then decreases after the next menstrual cycle begins.
Patients with AUB-O (ovulatory dysfunction) have uterine bleeding that occurs at unpredictable times, may vary widely in volume, and is not accompanied cyclic changes in basal body temperature.
Symptoms and signs reference
1. Munro MG, Critchley HOD, Fraser IS for the FIGO (International Federation of Gynecology and Obstetrics) Menstrual Disorders Committee): The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet 143 (3):393–408, 2018. doi: 10.1002/ijgo.12666 Epub 2018 Oct 10.
Diagnosis of AUB
Menstrual history
Pregnancy test, complete blood count (CBC,) and hormone measurement (eg, thyroid-stimulating hormone [TSH], prolactin)
Pelvic imaging studies, usually transvaginal ultrasonography
Sometimes procedures (endometrial sampling or hysteroscopy)
Women should be evaluated to identify the cause of abnormal uterine bleeding when the amount or timing of vaginal bleeding is inconsistent with normal menses. Pregnancy should be excluded, even in young adolescents and perimenopausal women.
The pattern of abnormal uterine bleeding often suggests possible causes (eg, regular cycles with prolonged or excessive bleeding suggest structural abnormalities; irregular bleeding or amenorrhea is often due to ovulatory dysfunction) and helps guide the choice of laboratory or imaging tests.
Coagulation disorders should be considered in adolescents who have anemia or require hospitalization for bleeding and in patients with a family history or other risk factors for coagulation disorders.
Laboratory testing
Several tests are typically done:
A urine or blood pregnancy test
Complete blood count (CBC)
Thyroid-stimulating hormone (TSH), prolactin, and sometimes progesterone levels or urine luteinizing hormone (LH)
All women of reproductive age with AUB should have a pregnancy test.
CBC is routinely done. Anemia may be severe in women who regularly have heavy periods. If iron deficiency anemia is suspected in women who have chronic, heavy bleeding, the serum ferritin level, which reflects body iron stores, is measured.
TSH levels are usually measured, and prolactin levels are measured, even when galactorrhea is absent, because thyroid disorders and hyperprolactinemia are common causes of AUB.
To determine whether a patient is anovulatory or ovulatory, some clinicians measure serum progesterone levels during the luteal phase (after day 14 of a normal menstrual cycle or after basal body temperature increases, as occurs during this phase). A level of ≥ 3 ng/mL (≥ 9.75 nmol/L) suggests that ovulation has occurred. Another option is for patients to use a home test kit for urine LH levels, which are measured daily for several days beginning at or after cycle day 9.
Other tests are done depending on results of the history and physical examination and include the following:
Testosterone and dehydroepiandrosterone sulfate (DHEAS) levels if polycystic ovary syndrome is suspected
Serum glucose and lipid levels, blood pressure, and body mass index if polycystic ovary syndrome is suspected
Follicle-stimulating hormone (FSH) and estradiol levels if primary ovarian insufficiency is possible
Coagulation tests if women have risk factors for coagulation disorders, bruising, or hemorrhage
Tests done to exclude other causes of vaginal bleeding include
A cervical cancer screening test (eg, Papanicolaou [Pap] test, human papillomavirus [HPV] test) if the patient is due for routine screening or a biopsy when a suspicious cervical lesion is seen during a pelvic examination
Testing for Neisseria gonorrhea and Chlamydia species if pelvic inflammatory disease or cervicitis is suspected
Imaging or procedures
Transvaginal ultrasonography is done as part of the evaluation for AUB in most patients. Specifically, it is done if women have any of the following:
Bleeding pattern, other symptoms, or a pelvic examination suggesting a structural lesion or pelvic organs cannot be examined adequately
Risk factors for endometrial cancer (eg, obesity, diabetes, hypertension, polycystic ovary syndrome, chronic eugonadal anovulation, other conditions associated with prolonged unopposed estrogen exposure)
Age ≥ 45 (earlier if women have risk factors)
Bleeding that continues despite use of empiric hormone therapy
Transvaginal ultrasonography can detect structural abnormalities, including most polyps, fibroids, other masses, ovarian abnormalities, adenomyosis, and endometrial thickening.
If focal thickening is detected, further testing may be needed to identify smaller intrauterine masses (eg, small endometrial polyps, submucous myomas). Sonohysterography (ultrasonography after saline is infused into the uterus) is useful in evaluating such abnormalities; it can be used to determine whether hysteroscopy, a more invasive test, is indicated and to plan resection of intrauterine masses. Or hysteroscopy may be done without sonohysterography. Both can be done in the office.
For some patients with postmenopausal bleeding, measurement of endometrial thickness (endometrial stripe) during transvaginal ultrasonography may be used as a first-line test to evaluate for endometrial neoplasia (hyperplasia or cancer). Endometrial sampling is required if patients have
Risk factors for endometrial cancer (eg, current or recent tamoxifen therapy)Risk factors for endometrial cancer (eg, current or recent tamoxifen therapy)
Persistent or recurrent bleeding
Endometrial thickness > 4 to 5 mm determined during ultrasonography (as a follow-up test)
In premenopausal women, endometrial thickness measurement is not used for evaluation for endometrial neoplasia because it varies across the menstrual cycle (1):
During menstruation: 2 to 4 mm
Early proliferative phase (cycle days 6 to 14): 5 to 7 mm
Late proliferative phase: ≤ 11 mm
Secretory phase: 7 to 16 mm
MRI provides detailed images that are useful in planning surgery but is expensive and is not the first-line imaging test for patients with AUB.
Endometrial sampling is usually recommended to rule out hyperplasia or cancer in women with any of the following:
Age ≥ 45 years
Age < 45 years with one or more risk factors for endometrial cancer (see above)
Abnormal bleeding that is persistent or recurs after a normal initial evaluation and despite treatment
Postmenopausal patients with abnormal endometrial findings detected during transvaginal ultrasonography (endometrial thickness > 4 to 5 mm or with focal or irregular endometrial thickening)
Inconclusive ultrasonography findings in a patient with suspected endometrial neoplasia
In endometrial sampling (which may be done as an office endometrial biopsy or a dilation and curettage procedure), only about 25% of the endometrium is analyzed, but sensitivity for detecting abnormal cells is approximately 97%. Most endometrial biopsy specimens contain proliferative or dyssynchronous endometrium, which confirms anovulation because no secretory endometrium is found.
Directed biopsy (with hysteroscopy) may be done to visualize the endometrial cavity directly and do targeted biopsies of focal endometrial abnormalities.
Evaluation reference
1. Weerakkody Y, Fahrenhorst-Jones T, Sharma R, et al: Endometrial thickness. Radiopaedia.org. https://doi.org/10.53347/rID-8106 Accessed 1/3/23.
Treatment of AUB
Control of bleeding, usually with a nonsteroidal anti-inflammatory drug (NSAID), tranexamic acid, or hormone therapyControl of bleeding, usually with a nonsteroidal anti-inflammatory drug (NSAID), tranexamic acid, or hormone therapy
Iron for iron deficiency anemia, if present
Sometimes a procedure to treat structural lesions (eg, hysteroscopic myomectomy, uterine fibroid embolization)
Hysterectomy for endometrial cancer; progestin therapy or hysterectomy for endometrial hyperplasia
Medications
Nonhormonal medications for abnormal uterine bleeding have fewer risks and adverse effects than hormone therapy and can be given intermittently, when bleeding occurs. They are used mainly to treat women who desire pregnancy, who wish to avoid hormone therapy, or who have heavy regular bleeding (menorrhagia). Choices include
Nonsteroidal anti-inflammatory drugs (NSAIDs), which reduce bleeding by 25 to 35% and relieve dysmenorrhea by reducing prostaglandin levels
Tranexamic acid, which inhibits plasminogen activator, reducing menstrual blood loss by 40 to 60% Tranexamic acid, which inhibits plasminogen activator, reducing menstrual blood loss by 40 to 60%
Hormone therapy (eg, estrogen/progestin contraceptives, progestins, a long-acting progestin-releasing intrauterine device [IUD]) is often tried first in women who want contraception or who are perimenopausal. This therapy does the following:
Suppresses endometrial development
Reestablishes predictable bleeding patterns
Decreases menstrual flow
Contraceptive hormone therapy is continued for as long as the patient wishes to use contraception. Once bleeding has been controlled for a few months, patients may choose to continue hormone therapy or to stop therapy to see if AUB is still present.
Combined estrogen/progestin oral contraceptives (COCs) are commonly given. COCs, used cyclically or continuously, can control abnormal uterine bleeding due to ovulatory dysfunction. Also, for women with heavy menstrual bleeding (eg, due to fibroids or adenomyosis), COCs decrease menstrual volume. Progestin-only oral contraceptives do not control heavy bleeding. Benefits of COCs include
Decreasing menstrual blood loss by 40 to 50%
Decreasing dysmenorrhea
Decreasing risk of uterine and ovarian cancer
Risks of an OC depend on the type of OC, dose, duration of use, and patient factors.
A progestogen may be used in the following cases:
Estrogen is contraindicated (eg, for patients with cardiovascular risk factors or prior deep vein thrombosis).
Estrogen is declined by the patient.
Withdrawal bleeding may be more predictable with cyclic progestin therapy (medroxyprogesterone acetate 10 mg/day orally or norethindrone acetate 2.5 to 5 mg/day orally) given for 21 days a month than with a COC. Cyclic natural (micronized) progesterone 200 mg/day for 21 days a month may be used, particularly if pregnancy is possible; however, it may cause drowsiness and does not decrease blood loss as much as a progestin.Withdrawal bleeding may be more predictable with cyclic progestin therapy (medroxyprogesterone acetate 10 mg/day orally or norethindrone acetate 2.5 to 5 mg/day orally) given for 21 days a month than with a COC. Cyclic natural (micronized) progesterone 200 mg/day for 21 days a month may be used, particularly if pregnancy is possible; however, it may cause drowsiness and does not decrease blood loss as much as a progestin.
If patients using noncontraceptive cyclic progestins or progesterone wish to prevent pregnancy, contraception should be used. Contraceptive progestin options include If patients using noncontraceptive cyclic progestins or progesterone wish to prevent pregnancy, contraception should be used. Contraceptive progestin options include
Levonorgestrel-releasing IUD:Levonorgestrel-releasing IUD: It is effective in up to 97% by 6 months, provides contraception, and relieves dysmenorrhea.
Depot medroxyprogesterone acetate:Depot medroxyprogesterone acetate: They cause amenorrhea and provide contraception but may cause irregular spotting and reversible bone loss.
Other treatments that are occasionally used to treat abnormal uterine bleeding due to ovulatory dysfunction include
Gonadotropin-releasing hormone (GnRH) agonists or antagonists: These medications suppress ovarian hormone production and cause amenorrhea; they are used to shrink fibroids or the endometrium preoperatively. However, their hypoestrogenic adverse effects (eg, osteoporosis) limit their use to 6 months; they are often used concurrently with low-dose hormone therapy. GnRH agonists are effective after 7 to 14 days because they initially cause a surge in luteinizing hormone and follicle stimulating hormone (1, 2). GnRH antagonists rapidly and reversibly suppress gonadotropins and ovarian sex hormones in women and reduce heavy bleeding. For either class of medication, add-back low-dose estrogen and progestin therapy may also be needed.
Danazol:Danazol: It reduces menstrual blood loss (by causing endometrial atrophy) but is not frequently used because it has many androgenic adverse effects, which may be lessened by using lower doses or a vaginal formulation. To be effective, danazol must be taken continuously, usually for about 3 months. It is usually used only when other forms of therapy are contraindicated. It reduces menstrual blood loss (by causing endometrial atrophy) but is not frequently used because it has many androgenic adverse effects, which may be lessened by using lower doses or a vaginal formulation. To be effective, danazol must be taken continuously, usually for about 3 months. It is usually used only when other forms of therapy are contraindicated.
If pregnancy is desired and bleeding is not heavy, ovulation induction with clomiphene (50 mg orally on days 5 through 9 of the menstrual cycle) may be tried.with clomiphene (50 mg orally on days 5 through 9 of the menstrual cycle) may be tried.
Procedures
Hysteroscopy with dilation and curettage (D & C) may be therapeutic as well as diagnostic; it may be the treatment of choice when anovulatory bleeding is severe or when hormone therapy is ineffective. Structural causes such as polyps or fibroids may be identified or removed during hysteroscopy. This procedure may decrease bleeding but, in some women, causes amenorrhea due to endometrial scarring (Asherman syndrome).
Endometrial ablation (eg, laser, rollerball, resectoscopic, thermal, or freezing) may help control bleeding in 60 to 80% of patients. Ablation is less invasive than hysterectomy, and the recovery time is shorter. Ablation may be repeated if heavy bleeding recurs after ablation is initially effective. If this treatment does not control bleeding or if bleeding continues to recur, the cause may be adenomyosis and thus is not abnormal uterine bleeding due to ovulatory dysfunction. Endometrial ablation does not prevent pregnancy. Pregnancy rates may be as high as 5% after ablation. Ablation causes scarring, which may make sampling the endometrium difficult later.
Treatment of fibroids includes
Uterine artery embolization is a minimally invasive procedure in which fluoroscopy is used to visualize fibroids. Femoral artery catheters are inserted, and embolic particles are injected through them to occlude the blood supply to the fibroids.
Myomectomy (removal of uterine fibroids) may be done hysteroscopically for submucosal fibroids or laparoscopically or via laparotomy for intramural or subserosal fibroids.
Hysterectomy, laparoscopic, abdominal, or vaginal, may be recommended for patients who decline hormone therapy or who, despite other treatments, have symptomatic anemia or poor quality of life caused by persistent, irregular bleeding.
Emergency treatment
Emergency measures are needed only rarely, when bleeding is very heavy. Patients are stabilized hemodynamically with IV crystalloid fluid, blood products, and other measures as needed. If bleeding persists, a bladder catheter is inserted into the uterus and inflated with 30 to 60 mL of water to tamponade the bleeding. Once patients are stable, hormone therapy is used to control bleeding.
Very rarely, in patients with very heavy bleeding due to anovulatory AUB, conjugated estrogens 25 mg IV every 4 to 6 hours for a total of 4 doses may be used. This therapy stops bleeding in about 70% of patients but increases risk of thrombosis. Immediately afterward, patients are given a combination OC, which may be continued until bleeding has been controlled for a few months.Very rarely, in patients with very heavy bleeding due to anovulatory AUB, conjugated estrogens 25 mg IV every 4 to 6 hours for a total of 4 doses may be used. This therapy stops bleeding in about 70% of patients but increases risk of thrombosis. Immediately afterward, patients are given a combination OC, which may be continued until bleeding has been controlled for a few months.
Treatment of endometrial hyperplasia
In postmenopausal women, atypical adenomatous endometrial hyperplasia is usually treated with hysterectomy.
In premenopausal women, atypical adenomatous endometrial hyperplasia may be treated with medroxyprogesterone acetate 40 mg orally once a day for 3 to 6 months or a levonorgestrel-releasing IUD (atypical adenomatous endometrial hyperplasia may be treated with medroxyprogesterone acetate 40 mg orally once a day for 3 to 6 months or a levonorgestrel-releasing IUD (3). After 3 to 6 months of treatment, endometrial sampling is repeated. If repeat endometrial sampling indicates resolution of hyperplasia, women may be given cyclic medroxyprogesterone acetate (5 to 10 mg orally once a day for 10 to 14 days each month) or, if pregnancy is desired, clomiphene. This treatment is given for 3 months, then response is assessed, usually by endometrial biopsy. If repeat endometrial sampling shows persistent or progressive atypical hyperplasia, hysterectomy may be necessary.). After 3 to 6 months of treatment, endometrial sampling is repeated. If repeat endometrial sampling indicates resolution of hyperplasia, women may be given cyclic medroxyprogesterone acetate (5 to 10 mg orally once a day for 10 to 14 days each month) or, if pregnancy is desired, clomiphene. This treatment is given for 3 months, then response is assessed, usually by endometrial biopsy. If repeat endometrial sampling shows persistent or progressive atypical hyperplasia, hysterectomy may be necessary.
More benign cystic or adenomatous hyperplasia can usually be treated with high-dose cyclic progestin therapy (eg, cyclic medroxyprogesterone acetate) or a progestin- or levonorgestrel-releasing IUD; sampling is repeated after about 3 months.More benign cystic or adenomatous hyperplasia can usually be treated with high-dose cyclic progestin therapy (eg, cyclic medroxyprogesterone acetate) or a progestin- or levonorgestrel-releasing IUD; sampling is repeated after about 3 months.
Treatment references
1. Schlaff WD, Ackerman RT, Al-Hendy A, et al: Elagolix for heavy menstrual bleeding in women with uterine fibroids. : Elagolix for heavy menstrual bleeding in women with uterine fibroids.N Engl J Med 382 (4):328–340, 2020. doi: 10.1056/NEJMoa1904351
2. de Lange ME, Huirne JAF: Linzagolix: An oral gonadotropin-releasing hormone receptor antagonist treatment for uterine fibroid-associated heavy menstrual bleeding. Lancet 400 (10356):866–867, 2002. doi: 10.1016/S0140-6736(22)01781-0
3. Mentrikoski MJ, Shah AA, Hanley KZ, et al: Assessing endometrial hyperplasia and carcinoma treated with progestin therapy. Am J Clin Pathol 38 (4):524–534, 2012. doi: 10.1309/AJCPM2TSDDF1MHBZ
Key Points
Abnormal uterine bleeding is a common medical issue; ovulatory dysfunction is the most common cause of abnormal uterine bleeding.
Test for treatable causes of bleeding; tests may include a pregnancy test, CBC and ferritin, measurement of hormone levels (TSH, prolactin, progesterone), and often ultrasonography, office hysteroscopy, and endometrial sampling.Test for treatable causes of bleeding; tests may include a pregnancy test, CBC and ferritin, measurement of hormone levels (TSH, prolactin, progesterone), and often ultrasonography, office hysteroscopy, and endometrial sampling.
In women at risk, do endometrial sampling to check for endometrial hyperplasia or cancer.
If medications are needed to control bleeding, treat with NSAIDs, tranexamic acid, estrogen/progestin OCs, levonorgestrel-releasing IUDs, gonadotrophin agonists or antagonists, or other hormones.If medications are needed to control bleeding, treat with NSAIDs, tranexamic acid, estrogen/progestin OCs, levonorgestrel-releasing IUDs, gonadotrophin agonists or antagonists, or other hormones.
Treat structural lesions or bleeding that does not respond to medications with a procedure (eg, hysteroscopy, endometrial ablation, hysterectomy).







