


Cardiopulmonary resuscitation (CPR) is an organized, sequential response to cardiac arrest, including
Recognition of absent breathing and circulation
Basic life support with chest compressions and rescue breathing
Advanced cardiac life support (ACLS) with definitive airway and rhythm control
Postresuscitative care
(See also Neonatal Resuscitation and Cardiopulmonary Resuscitation in Infants and Children.)
Prompt initiation of chest compressions and early defibrillation (when indicated) are the keys to success.
Speed, efficiency, and proper application of CPR with the fewest possible interruptions determine successful outcome; the rare exception is profound hypothermia caused by cold water immersion without drowning, when successful resuscitation may be accomplished with intermittent CPR even after prolonged arrest (1).
Overview of CPR
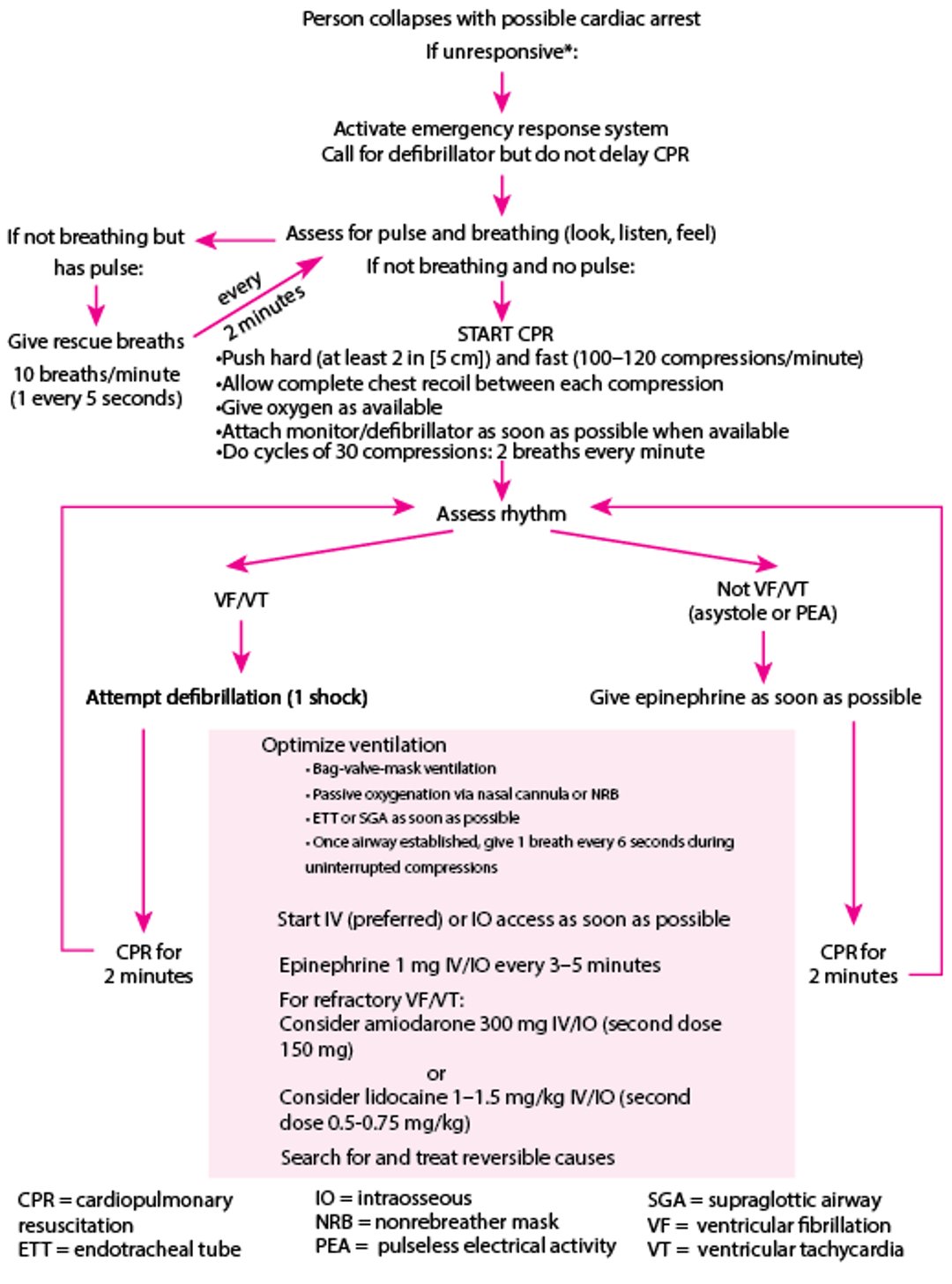
Guidelines for health care professionals from the American Heart Association (AHA) are followed (see figure Adult Comprehensive Emergency Cardiac Care) (2, 3). If a person has collapsed with possible cardiac arrest, a rescuer first establishes unresponsiveness and confirms absence of breathing or the presence of only gasping respirations. Then, the rescuer calls for help. Anyone answering is directed to activate the emergency response system (or appropriate in-hospital resuscitation personnel) and, if possible, obtain a defibrillator. Basic life support should be started immediately (2).
If no one responds to the call for help, the rescuer first activates the emergency response system and then begins basic life support by giving 30 chest compressions at a rate of 100 to 120/minute and a depth of 5 to 6 cm, allowing the chest wall to return to full height between compressions, and then opening the airway (lifting the chin and tilting back the forehead) and giving 2 rescue breaths. The cycle of compressions and breaths is continued (see table CPR Techniques for Health Care Professionals) without interruption; preferably each rescuer is relieved every 2 minutes. It is crucial that even untrained bystanders begin and maintain continuous chest compressions until skilled help arrives. Therefore, many emergency response providers now give pre-arrival instructions to callers, including phone instruction in compressions-only CPR.
When a defibrillator (manual or automated) becomes available, a person in ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) is given an unsynchronized shock (see also Defibrillation). If the cardiac arrest is witnessed and a defibrillator is on the scene, a person in VF or VT should be immediately defibrillated, with compressions immediately resumed after shock is delivered; early defibrillation may promptly convert VF or pulseless VT to a perfusing rhythm. If the initial rhythm is pulseless electrical activity or asystole, an initial dose of epinephrine 1 mg IV/IO (intravenous/intraosseous) should be administered as soon as possible after recognition of cardiac arrest. ). If the cardiac arrest is witnessed and a defibrillator is on the scene, a person in VF or VT should be immediately defibrillated, with compressions immediately resumed after shock is delivered; early defibrillation may promptly convert VF or pulseless VT to a perfusing rhythm. If the initial rhythm is pulseless electrical activity or asystole, an initial dose of epinephrine 1 mg IV/IO (intravenous/intraosseous) should be administered as soon as possible after recognition of cardiac arrest.
Adult Comprehensive Emergency Cardiac Care
* If an adequate number of trained personnel are available, patient assessment, CPR, and activation of the emergency response system should occur simultaneously. |
Based on the 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. |
The techniques used in basic 1- and 2-rescuer CPR are listed in Table CPR Techniques for Health Care Professionals. Mastery is best acquired by hands-on training. |

CPR Techniques for Health Care Professionals
Age Group | One-Rescuer CPR* | Two-Rescuer CPR | Breath Size |
|---|---|---|---|
Adults and adolescents | Cycles of 30 chest compressions at a rate of 100–120 compressions per minute, followed by 2 breaths (1 second each) Depth of compressions 5–6 cm; allow complete chest recoil between compressions | Cycles of 30 chest compressions at a rate of 100–120 per minute, followed by 2 breaths (1 second each over a pause of 3–4 seconds) OR continuous compressions with 1 breath every 6 seconds If an advanced airway (SGA or ETT) is used, asynchronous ventilation of 1 breath every 6 seconds, with continuous compressions | Each breath 500–600 mL (caution against hyperventilation) |
Children (1 year–puberty)† | Cycles of 30 compressions at a rate of 100–120 compressions per minute, followed by 2 breaths (1 second each) Depth of compression is 5 cm or ⅓ the anterior-posterior diameter of the chest;allow for complete chest recoil between compressions | Cycles of 15 chest compressions at a rate of 100–120 compressions per minute, followed by 2 breaths (1 second each) If an advanced airway (SGA or ETT) is used, ventilations should be done at a rate of 20–30 per minute, without pausing compressions | Smaller breaths than for adults (enough to make chest rise) |
Infants (< 1 year, excluding neonates) | Cycles of 30 compressions at a rate of 100–120 compressions per minute, followed by 2 breaths (1 second each) Depth of compressions should be 4 cm or 1/3 the anterior-posterior diameter of the chest; allow for complete recoil between compressions. | Cycles of 15 chest compressions at a rate of 100–120 compressions per minute, followed by 2 breaths (1 second each) If an advanced airway (SGA or ETT) is used, ventilations should be done at a rate of 30 per minute, without pausing compressions | Small breath, just enough to see chest rise |
* For lay rescuer, compression-only CPR is recommended in adults if the rescuer is unwilling or unable to provide mouth-to-mouth rescue breaths. | |||
† Puberty is defined as the appearance of breasts in females and axillary hair in males. | |||
Data from Panchal AR, Bartos JA, Cabañas JG, et al: Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 142(16_suppl_2):S366–S468, 2020. doi:10.1161/CIR.0000000000000916 and from Topjian AA, Raymond TT, Atkins D, et al: Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 142(16_suppl_2):S469–S523, 2020. doi:10.1161/CIR.0000000000000901 | |||
ETT = endotracheal tube; SGA = supraglottic airway. | |||
General references
1. Gordon L, Paal P, Ellerton JA, Brugger H, Peek GJ, Zafren K: Delayed and intermittent CPR for severe accidental hypothermia. Resuscitation 90:46–49, 2015. doi:10.1016/j.resuscitation.2015.02.017
2. Panchal AR, Bartos JA, Cabañas JG, et al: Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 142(16_suppl_2):S366–S468, 2020. doi:10.1161/CIR.0000000000000916
3. Atkins DL, Sasson C, Hsu A, et al: 2022 Interim Guidance to Health Care Providers for Basic and Advanced Cardiac Life Support in Adults, Children, and Neonates With Suspected or Confirmed COVID-19: From the Emergency Cardiovascular Care Committee and Get With The Guidelines-Resuscitation Adult and Pediatric Task Forces of the American Heart Association in Collaboration With the American Academy of Pediatrics, American Association for Respiratory Care, the Society of Critical Care Anesthesiologists, and American Society of Anesthesiologists. Circ Cardiovasc Qual Outcomes 15(4):e008900, 2022. doi:10.1161/CIRCOUTCOMES.122.008900
CPR: Airway and Breathing
Opening the airway is the second priority (see Clearing and Opening the Upper Airway) after beginning chest compressions. For witnessed out-of-hospital cardiac arrest with an initial shockable rhythm, it is acceptable to provide passive oxygenation for the first 6 minutes, as part of an emergency medical services bundle of care aimed at minimizing pauses in the initial provision of CPR and defibrillation. For mechanical measures regarding resuscitation in children, see table Guide to Pediatric Resuscitation—Mechanical Measures.
When health care professionals provide CPR, bag-valve-mask ventilation should be started as early as possible, but bag-valve-mask ventilation should not delay initiation of compressions or defibrillation. Lay rescuers may provide compressions-only CPR or, if trained to do so, may give rescue breaths delivered mouth-to-mouth (for adults, adolescents, and children) or combined mouth-to-mouth-and-nose (for infants). If available, an oropharyngeal airway may be inserted to maintain airway patency during bag-valve-mask ventilation. Cricoid pressure is not recommended.

If abdominal distention develops, the airway is rechecked for patency, and the amount of air delivered during rescue breathing is reduced. Nasogastric or orogastric intubation to relieve gastric distention should not interrupt CPR.
When qualified rescuers are present, an advanced airway (endotracheal tube or supraglottic airway) is placed without interruption of chest compressions after initial CPR and defibrillation attempts, as described under Airway Establishment and Control. A breath is given every 6 seconds (10 breaths/minute) without interrupting chest compression in adults; infants and children are given breaths every 2 to 3 seconds (20 to 30 breaths/minute). However, chest compression and defibrillation take precedence over endotracheal intubation. Unless highly experienced rescuers are available, endotracheal intubation may be delayed in favor of ventilation with a bag-valve-mask, laryngeal mask airway, or similar device.
For patients suspected of having COVID-19, the American Heart Association released interim guidance for basic and advanced life support (1, 2).
Airway and breathing references
1. Edelson DP, Sasson C, Chan PS, et al; American Heart Association ECC Interim COVID Guidance Authors: Interim Guidance for Basic and Advanced Life Support in Adults, Children, and Neonates With Suspected or Confirmed COVID-19: From the Emergency Cardiovascular Care Committee and Get With The Guidelines-Resuscitation Adult and Pediatric Task Forces of the American Heart Association. Circulation 141(25):e933–e943, 2020. doi: 10.1161/CIRCULATIONAHA.120.047463
2. Goodloe JM, Topjian A, Hsu A, et al: Interim Guidance for Emergency Medical Services Management of Out-of-Hospital Cardiac Arrest During the COVID-19 Pandemic. Circ Cardiovasc Qual Outcomes 14(7):e007666, 2021. doi:10.1161/CIRCOUTCOMES.120.007666
CPR: Circulation
Chest compressions
Chest compression should be started immediately on recognition of cardiac arrest and done with minimal interruption until defibrillation is available. In a patient who is unresponsive and whose collapse was unwitnessed, the trained rescuer should immediately begin external (closed chest) cardiac compressions, followed by rescue breathing. Chest compressions must not be interrupted for > 10 seconds at any time (eg, for intubation, defibrillation, rhythm analysis, central IV catheter placement, or transport). A compression cycle should consist of 50% compression and 50% release; during the release phase, it is important to allow the chest to recoil fully. Rhythm interpretation and defibrillation (if appropriate) are done as soon as a defibrillator is available.
The recommended chest compression depth for adults is approximately 5 to 6 cm. Ideally, external cardiac compression produces a palpable pulse with each compression, although cardiac output is only 20 to 30% of normal. However, palpation of pulses during chest compression is difficult, even for experienced clinicians and is often unreliable. Quantitative end-tidal carbon dioxide monitoring may provide a better estimate of cardiac output during chest compressions; patients with inadequate perfusion have little venous return to the lungs and hence a low end-tidal carbon dioxide level. Hyperventilation during CPR can also result in a low end-tidal carbon dioxide level. While there is limited evidence supporting specific numbers in physiologic monitoring, it is generally accepted that an end-tidal carbon dioxide level of > 10 and ideally > 20 mm Hg is associated with adequate CPR. A sudden significant rise in end-tidal carbon dioxide level, or a palpable pulse during pause in compressions, indicates restoration of spontaneous circulation.
Mechanical chest compression devices are available; these devices are as effective as properly executed manual compressions and can minimize effects of performance error and fatigue. They may be particularly helpful in some circumstances, such as during patient transport or in the cardiac catheterization laboratory. These devices have also been recommended for use in patients with suspected or confirmed COVID-19 (1).
Open-chest cardiac compression via thoracotomy may be effective but is used only in patients with penetrating chest injuries, shortly after cardiac surgery (ie, within 48 hours), in cases of cardiac tamponade, and most especially after cardiac arrest in the operating room when the patient’s chest is already open. However, thoracotomy requires training and experience and is best done only within these limited indications.
Complications of chest compression
A frequent complication is regurgitation followed by aspiration of gastric contents, causing life-threatening aspiration pneumonia in patients who have been resuscitated.
Costochondral separation and fractured ribs often cannot be avoided because it is important to compress the chest enough to produce sufficient blood flow. Fractures are quite rare in children because of the flexibility of the chest wall.
Bone marrow emboli to the lungs have rarely been reported after external cardiac compression, but there is no clear evidence that they contribute to mortality. Lung injury is rare, but pneumothorax after a penetrating rib fracture may occur. Tension pneumothorax should be considered in a patient who has achieved return of spontaneous circulation after prolonged CPR and subsequently becomes difficult to ventilate or hypoxic and suddenly rearrests.
Serious myocardial injury caused by compression is highly unlikely, with the possible exception of injury to a preexisting ventricular aneurysm.
Concern for these injuries should not deter the rescuer from doing CPR.
Laceration of the liver is a rare but potentially serious (sometimes fatal) complication and is usually caused by compressing the abdomen below the sternum. Rupture of the stomach (particularly if the stomach is distended with air) is also a rare complication. Delayed rupture of the spleen is very rare.
Circulation reference
1. Atkins DL, Sasson C, Hsu A, et al: 2022 Interim Guidance to Health Care Providers for Basic and Advanced Cardiac Life Support in Adults, Children, and Neonates With Suspected or Confirmed COVID-19: From the Emergency Cardiovascular Care Committee and Get With The Guidelines-Resuscitation Adult and Pediatric Task Forces of the American Heart Association in Collaboration With the American Academy of Pediatrics, American Association for Respiratory Care, the Society of Critical Care Anesthesiologists, and American Society of Anesthesiologists. Circ Cardiovasc Qual Outcomes 2022;15(4):e008900. doi:10.1161/CIRCOUTCOMES.122.008900
CPR: Defibrillation
In adults, the most common rhythm in witnessed cardiac arrest is ventricular fibrillation (VF); rapid conversion to a perfusing rhythm is essential. Pulseless ventricular tachycardia (VT) is treated the same as VF.
Prompt defibrillation is the only intervention for cardiac arrest, other than high-quality CPR, that has been shown to improve survival; however, the success of defibrillation is time dependent, with approximately a 10% decline in success after each minute of VF (or pulseless VT). Automated external defibrillators (AEDs) allow minimally trained rescuers to treat pulseless VT or VF. Their use by first responders (police and fire services) and their prominent availability in public locations have increased the likelihood of resuscitation.
Defibrillating paddles or pads are placed with one on the anterior right chest wall below the clavicle at the mid-clavicular line and the other over the left 5th or 6th intercostal space at the apex of the heart in the anterior-axillary line. Alternatively, the 2 pads may be placed with one pad over the anterior left hemithorax and the other pad on the posterior left hemithorax. Defibrillator paddles are used with conducting paste; pads have conductive gel incorporated into them. Most defibrillators use pads rather than paddles.
One initial shock is advised as soon as a shockable rhythm is detected, after which chest compressions are immediately resumed. Energy level for biphasic defibrillators is between 150 and 200 joules (2 joules/kg in children) for the initial shock; monophasic defibrillators are set at 360 joules for the initial shock. Postshock rhythm is not checked until after 2 minutes of chest compressions. Subsequent shocks are delivered at the same or higher energy level (maximum 360 joules in adults, or 10 joules/kg in children). Patients remaining in VF or pulseless VT receive additional shocks every 2 minutes, along with continued chest compression and ventilation and optional pharmacotherapy.
CPR: Monitoring and IV Access
Electrocardiographic (ECG) monitoring is established to identify the underlying cardiac rhythm.
An IV line may be started; 2 lines minimize the risk of losing IV access during CPR. Large-bore peripheral lines in the antecubital veins are preferred. In adults and children, if a peripheral line cannot be established quickly, a subclavian or femoral central line (see Procedure) can be placed provided it can be done without stopping chest compression (often difficult). Intraosseous lines (see Intraosseous Infusion) are alternatives, especially in children, as they can be placed quickly to avoid delay in administration of the first dose of epinephrine. Femoral vein catheters (see ) are alternatives, especially in children, as they can be placed quickly to avoid delay in administration of the first dose of epinephrine. Femoral vein catheters (seeProcedure) are an option because CPR does not need to be stopped and they have less potential for lethal complications; however, they may have a lower rate of successful placement because no discrete femoral arterial pulsations are available to guide insertion.
The type and volume of fluids or medications given depend on the clinical circumstances. Usually, IV 0.9% saline is given slowly (sufficient only to keep an IV line open); vigorous volume replacement (crystalloid and colloid solutions, blood) is required only when arrest results from hypovolemia (see Intravenous Fluid Resuscitation), or as part of the management of cardiogenic shock after return of spontaneous circulation.
CPR: Special Circumstances
In accidental electrical shock, rescuers must be certain that the patient is no longer in contact with the electrical source to avoid shocking themselves. Use of nonmetallic grapples or rods and grounding of the rescuer allows for safe removal of the patient before starting CPR.
In drowning, rescue breathing may be started in shallow water, although chest compression is not likely to be effectively done until the patient is placed horizontally on a firm surface.
If cardiac arrest follows traumatic injury, airway-opening maneuvers and a brief period of external ventilation after clearing the airway have the highest priority because airway obstruction is the most likely treatable cause of arrest. If cervical spine injury is suspected, jaw thrust (see figure Jaw Thrust), but not head tilt and chin lift, is advised. Other survivable causes of traumatic cardiac arrest include cardiac tamponade and tension pneumothorax, for which immediate needle decompression is lifesaving. However, most patients with traumatic cardiac arrest have severe hypovolemia due to blood loss (for which chest compression may be ineffective) or nonsurvivable brain injuries.
CPR: Medications for ACLS
Despite widespread and long-standing use, no medication or combination of medications has been definitively shown to increase neurologically intact survival to hospital discharge in patients with cardiac arrest. Some medications do seem to improve the likelihood of return of spontaneous circulation and thus may reasonably be given (for dosing, including pediatric, see table Medications Commonly Used for Resuscitation). Pharmacotherapy for shock and cardiac arrest continues to be researched.
Medications Commonly Used for Resuscitation*
Medication† | Adult Dose | Pediatric Dose |
|---|---|---|
AdenosineAdenosine | 6 mg initially, then 12 mg × 2 if needed | 0.1 mg/kg initially, then 0.2 mg/kg × 2 |
AmiodaroneAmiodarone | For VF/pulseless VT: 300 mg IV push over 2 minutes If persistent VF/pulseless VT, may give additional 150 mg | For VF/pulseless VT: 5 mg/kg IV push If persistent VF/pulseless VT, may repeat up to 3 total doses |
For perfusing VT:
| For perfusing VT: 5 mg/kg over 20–60 minutes, may repeat twice to a maximum of 15 mg/kg/day | |
Atropine‡ Atropine‡ | 1 mg, repeat every 3–5 minutes to effect or total dose of 3 mg, minimum dose 0.5 mg | 0.02 mg/kg, repeat once in 3–5 minutes if needed, minimum dose 0.1 mg |
Calcium chlorideCalcium chloride | 1 g | 20 mg/kg |
Calcium gluceptate§ | 0.66 g | N/A |
Calcium gluconateCalcium gluconate | 3 g | 30 mg/kg |
DobutamineDobutamine | 2–5 mcg/kg/minute—increasing as needed to maximum 20 mcg/kg/minute | Same as adult dose |
DopamineDopamine | 2–5 mcg/kg/minute—increasing as needed to maximum 20 mcg/kg/minute | Same as adult dose |
EpinephrineEpinephrine | Bolus: 1 mg Infusion: 2–10 mcg/minute | Bolus: 0.01 mg/kg Infusion: 0.1–1.0 mcg/kg/minute |
Glucose (only for documented hypoglycemia) | 25 g 50% D/W | 0.5–1 g/kg of 10% D/W Avoid high concentrations in infants and young children. Recommend using 10% D/W for infants and 10% or 25% for children |
LidocaineLidocaine | 1–1.5 mg/kg; repeat every 5–10 minutes to a maximum of 3 mg/kg | Loading dose: 1 mg/kg Infusion: 20–50 mcg/kg/minute |
Magnesium sulfate | 1–2 g | 25–50 mg/kg to a maximum of 2 g |
NaloxoneNaloxone | 2–4 mg intranasal or 0.4 mg IM | 0.1 mg/kg if patients are < 20 kg or < 5 years 2 mg if patients are ≥ 20 kg or ≥ 5 years |
NorepinephrineNorepinephrine | Infusion: 5–30 mcg/minute | Infusion: Starting with 0.05–0.1 mcg/kg/minute (maximum dose 2 mcg/kg/minute) |
PhenylephrinePhenylephrine | Infusion: 0.1–0.5 mcg/kg/minute | Infusion: 0.1–0.5 mcg/kg/minute |
ProcainamideProcainamide | 20–50 mg/minute (total maximum dose of 17 mg/kg | 15 mg/kg over 30–60 minutes |
Sodium bicarbonateSodium bicarbonate | 50 mEq | 1 mEq/kg The PALS 2020 guideline does not recommend sodium bicarbonate in pediatric patients except in those with hyperkalemia, hypocalcemia, hypermagnesemia, tricyclic antidepressant toxicity, or calcium channel blocker overdose¶The PALS 2020 guideline does not recommend sodium bicarbonate in pediatric patients except in those with hyperkalemia, hypocalcemia, hypermagnesemia, tricyclic antidepressant toxicity, or calcium channel blocker overdose¶ |
* For indications and use, see text. | ||
† IV or intraosseous. | ||
‡ Atropine is no longer recommended in patients with pulseless VT. It's use is limited to patients with symptomatic bradycardia.‡ Atropine is no longer recommended in patients with pulseless VT. It's use is limited to patients with symptomatic bradycardia. | ||
§ Rarely used. | ||
¶ Maconochie IK, Aickin R, Hazinski MF, et al. Pediatric Life Support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Pediatrics 2021;147(Suppl 1):e2020038505B. doi:10.1542/peds.2020-038505B | ||
D/W = dextrose in water; SVT dextrose in water; SVT= supraventricular tachycardia;VF = ventricular fibrillation; VT = ventricular tachycardia. | ||
In a patient with a peripheral IV line, administration of medication is followed by a fluid bolus (“wide open” IV in adults; 3 to 5 mL in young children) to flush the medication into the central circulation. In a patient without IV or intraosseous (IO) access, naloxone, atropine, and epinephrine, when indicated, may be given via the endotracheal tube at 2 to 2.5 times the IV dose. During administration of a medication via endotracheal tube, compression should be briefly stopped.In a patient with a peripheral IV line, administration of medication is followed by a fluid bolus (“wide open” IV in adults; 3 to 5 mL in young children) to flush the medication into the central circulation. In a patient without IV or intraosseous (IO) access, naloxone, atropine, and epinephrine, when indicated, may be given via the endotracheal tube at 2 to 2.5 times the IV dose. During administration of a medication via endotracheal tube, compression should be briefly stopped.
First-line medications
The main first-line medication used in cardiac arrest is
EpinephrineEpinephrine
Epinephrine 1 mg IV/IO should be given as soon as possible to patients with a nonshockable initial rhythm and may be repeated every 3 to 5 minutes. It should be given early in nonshockable rhythms, because evidence suggests survival is increased when it is given earlier in resuscitation (Epinephrine 1 mg IV/IO should be given as soon as possible to patients with a nonshockable initial rhythm and may be repeated every 3 to 5 minutes. It should be given early in nonshockable rhythms, because evidence suggests survival is increased when it is given earlier in resuscitation (1), or for ventricular tachycardia (VT) or ventricular fibrillation (VF) refractory to 2 shocks. Epinephrine has combined alpha-adrenergic and beta-adrenergic effects. The alpha-adrenergic effects may augment coronary diastolic pressure, thereby increasing subendocardial perfusion during chest compressions. Epinephrine also increases the likelihood of successful defibrillation. However, beta-adrenergic effects may be detrimental because they increase oxygen requirements (especially of the heart) and cause vasodilation. Intracardiac injection of epinephrine is not recommended because, in addition to interrupting precordial compression, pneumothorax, coronary artery laceration, and cardiac tamponade may occur.
Vasopressin is no more effective than epinephrine and is therefore not recommended as a first-line medication in the American Heart Association's guidelines (Vasopressin is no more effective than epinephrine and is therefore not recommended as a first-line medication in the American Heart Association's guidelines (2). However, if epinephrine is unavailable, vasopressin may be substituted.
AmiodaroneAmiodarone 300 mg can be given if a third attempt at defibrillation is unsuccessful after epinephrine. An additional dose of 300 mg can be given if a third attempt at defibrillation is unsuccessful after epinephrine. An additional dose ofamiodarone (150 mg) may be given if refractory shockable rhythms persist despite 5 or more shocks and 2 or more doses of epinephrine. (150 mg) may be given if refractory shockable rhythms persist despite 5 or more shocks and 2 or more doses of epinephrine.Amiodarone is also of potential value if pulseless VT or VF recurs after successful defibrillation; a lower initial dose (150 mg) is given over 10 minutes followed by a continuous infusion. There is no persuasive proof that it increases survival to hospital discharge. Lidocaine is an alternative antiarrhythmic to is also of potential value if pulseless VT or VF recurs after successful defibrillation; a lower initial dose (150 mg) is given over 10 minutes followed by a continuous infusion. There is no persuasive proof that it increases survival to hospital discharge. Lidocaine is an alternative antiarrhythmic toamiodarone.
Other medications
A range of additional medications may be useful in specific settings.
Atropine sulfateAtropine sulfate is a vagolytic medication that increases heart rate and conduction through the atrioventricular node. It is given for symptomatic bradyarrhythmias and high-degree atrioventricular nodal block. It is not recommended for asystole or pulseless electrical activity.
Calcium chlorideCalcium chloride is recommended for patients with hyperkalemia, hypermagnesemia, hypocalcemia, or calcium channel blocker toxicity. In other patients, because intracellular calcium is already higher than normal, additional calcium is likely to be detrimental. Because cardiac arrest in patients on renal dialysis is often a result of or accompanied by hyperkalemia, these patients may benefit from a trial of calcium if bedside potassium determination is unavailable. Caution is necessary because calcium exacerbates digitalis toxicity and can cause cardiac arrest.
LidocaineLidocaine is recommended as an alternative to amiodarone for VF or VT that is unresponsive to defibrillation and initial vasopressor therapy with epinephrine. It may also be considered after return of spontaneous circulation after arrest due to VF or VT (in adults) to prevent recurrent VF or VT.is recommended as an alternative to amiodarone for VF or VT that is unresponsive to defibrillation and initial vasopressor therapy with epinephrine. It may also be considered after return of spontaneous circulation after arrest due to VF or VT (in adults) to prevent recurrent VF or VT.
Magnesium sulfate has not been shown to improve outcome in randomized clinical studies (3). However, it may be helpful in patients with torsades de pointes or known or suspected magnesium deficiency (ie, patients with alcohol use disorder or protracted diarrhea).
ProcainamideProcainamide is a second-line medication for treatment of refractory VF or VT. However, procainamide is not recommended for pulseless arrest in children and is no longer recommended by American Heart Association guidelines for treatment of post-arrest ventricular arrhythmias. However, per the 2021 European Resuscitation Council guidelines, it is an option to treat hemodynamically stable patients with wide complex QRS tachycardia, as some studies have shown an association with fewer major adverse events as compared with amiodarone (is a second-line medication for treatment of refractory VF or VT. However, procainamide is not recommended for pulseless arrest in children and is no longer recommended by American Heart Association guidelines for treatment of post-arrest ventricular arrhythmias. However, per the 2021 European Resuscitation Council guidelines, it is an option to treat hemodynamically stable patients with wide complex QRS tachycardia, as some studies have shown an association with fewer major adverse events as compared with amiodarone (4).
PhenytoinPhenytoin may rarely be used to treat VT, but only when VT is due to digitalis toxicity and is refractory to other medications. A dose of 50 to 100 mg/minute every 5 minutes is given until rhythm improves or the total dose reaches 20 mg/kg.
Sodium bicarbonateSodium bicarbonate is not recommended unless cardiac arrest is caused by hyperkalemia, severe metabolic acidosis, or tricyclic antidepressant overdose. Sodium bicarbonate may be considered when cardiac arrest is prolonged (> 10 minutes); it is given only if there is good ventilation. When sodium bicarbonate is used, serum bicarbonate concentration or base deficit should be monitored before infusion and after each 50-mEq dose (1mEq/kg in children).
Medications for ACLS references
1. Okubo M, Komukai S, Callaway CW, Izawa J. Association of Timing of Epinephrine Administration With Outcomes in Adults With Out-of-Hospital Cardiac Arrest. JAMA Netw Open 4(8):e2120176, 2021. doi:10.1001/jamanetworkopen.2021.20176
2. Merchant RM, Topjian AA, Panchal AR, et al: Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 142(16_suppl_2):S337-S357, 2020. doi:10.1161/CIR.0000000000000918
3. Thel MC, Armstrong AL, McNulty SE, Califf RM, O'Connor CM: Randomised trial of magnesium in in-hospital cardiac arrest. Duke Internal Medicine Housestaff. Lancet 350(9087):1272–1276, 1997. doi:10.1016/s0140-6736(97)05048-4
4. Soar J, Böttiger BW, Carli P, et al: European Resuscitation Council Guidelines 2021: Adult advanced life support [published correction appears in Resuscitation 2021 Oct;167:105-106]. Resuscitation 161:115-151, 2021. doi:10.1016/j.resuscitation.2021.02.010
Arrhythmia Treatment in CPR
VF or pulseless VT is treated with one direct-current shock, preferably with biphasic waveform, as soon as possible after those rhythms are identified. Despite some laboratory evidence to the contrary, it is not recommended to delay defibrillation to administer a period of chest compressions. Chest compression should be interrupted as little as possible and for no more than 10 seconds at a time for defibrillation. Recommended energy levels for defibrillation vary:
120 to 200 joules for biphasic defibrillators
360 joules for monophasic defibrillators
If this treatment is unsuccessful after 2 attempts, epinephrine 1 mg IV is administered and repeated every 3 to 5 minutes. Defibrillation at the same energy level or higher is attempted 1 to 2 minutes after each epinephrine administration. If this treatment is unsuccessful after 2 attempts, epinephrine 1 mg IV is administered and repeated every 3 to 5 minutes. Defibrillation at the same energy level or higher is attempted 1 to 2 minutes after each epinephrine administration.
If VF persists, amiodarone 300 mg IV is given. Then, if VF/VT recurs, amiodarone150 mg is given followed by infusion of 1 mg/minute for 6 hours, then 0.5 mg/minute.If VF persists, amiodarone 300 mg IV is given. Then, if VF/VT recurs, amiodarone150 mg is given followed by infusion of 1 mg/minute for 6 hours, then 0.5 mg/minute.
Automatic external defibrillators (AEDs) provide a pediatric cable that effectively reduces the energy delivered to children. (For pediatric energy levels, see Defibrillation; for medication doses, see table Medications Commonly Used for Resuscitation.)
Asystole can be mimicked by a loose or disconnected monitor lead; thus, monitor connections should be checked and the rhythm viewed in an alternative lead. If asystole is confirmed, the patient is given epinephrine 1 mg IV repeated every 3 to 5 minutes. Defibrillation of apparent asystole (because it “might be fine VF”) is discouraged because electrical shocks may injure the nonperfused heart.Asystole can be mimicked by a loose or disconnected monitor lead; thus, monitor connections should be checked and the rhythm viewed in an alternative lead. If asystole is confirmed, the patient is given epinephrine 1 mg IV repeated every 3 to 5 minutes. Defibrillation of apparent asystole (because it “might be fine VF”) is discouraged because electrical shocks may injure the nonperfused heart.
Pulseless electrical activity is circulatory collapse that occurs despite satisfactory electrical complexes on the electrocardiogram (ECG). Patients with pulseless electrical activity receive epinephrine 1.0 mg IV repeated every 3 to 5 minutes, followed by 500- to 1000-mL (20 mL/kg for children) infusion of 0.9% saline if hypovolemia is suspected. Cardiac tamponade can cause pulseless electrical activity, but this disorder usually occurs in patients after thoracotomy and in patients with known pericardial effusion or major chest trauma. In such settings, immediate pericardiocentesis or thoracotomy is done (see figure Pulseless electrical activity is circulatory collapse that occurs despite satisfactory electrical complexes on the electrocardiogram (ECG). Patients with pulseless electrical activity receive epinephrine 1.0 mg IV repeated every 3 to 5 minutes, followed by 500- to 1000-mL (20 mL/kg for children) infusion of 0.9% saline if hypovolemia is suspected. Cardiac tamponade can cause pulseless electrical activity, but this disorder usually occurs in patients after thoracotomy and in patients with known pericardial effusion or major chest trauma. In such settings, immediate pericardiocentesis or thoracotomy is done (see figurePericardiocentesis). Tamponade is rarely an occult cause of cardiac arrest but, if suspected, can be confirmed by ultrasonography or, if ultrasonography is unavailable, pericardiocentesis.
CPR: Termination of Resuscitation
CPR should be continued until the cardiopulmonary system is stabilized, the patient is pronounced dead, or a lone rescuer is physically unable to continue. If cardiac arrest is thought to be due to hypothermia, CPR should be continued until the body is rewarmed to 34° C.
The decision to terminate resuscitation is a clinical one, and clinicians take into account duration of arrest, age of the patient, and prognosis of underlying medical conditions. The decision is typically made when spontaneous circulation has not been established after CPR and advanced cardiovascular life support measures have been done. In patients who are intubated, an end-tidal carbon dioxide (ETCO2) level of < 10 mm Hg after 20 minutes of CPR is a poor prognostic sign. Studies of outcomes from cardiac arrest have found that neurologically favorable survival is < 1% in older patients—1, 2 with unwitnessed cardiac arrest and initial non-shockable rhythm.
Termination of resuscitation references
1. Goto Y, Funada A, Maeda T, Okada H, Goto Y: Field termination-of-resuscitation rule for refractory out-of-hospital cardiac arrests in Japan. J Cardiol 73(3):240–246, 2019. doi:10.1016/j.jjcc.2018.12.002
2. Grunau B, Scheuermeyer F, Kawano T, et al: North American validation of the Bokutoh criteria for withholding professional resuscitation in non-traumatic out-of-hospital cardiac arrest. Resuscitation 135:51–56, 2019. doi:10.1016/j.resuscitation.2019.01.008
CPR: Postresuscitative Care
Restoration of spontaneous circulation is only an intermediate goal in resuscitation. The ultimate goal is survival to hospital discharge with good neurologic function, which is achieved by only a minority of patients with restoration of spontaneous circulation. To maximize the likelihood of a good outcome, clinicians must provide good supportive care (eg, manage blood pressure, temperature, and cardiac rhythm) and treat underlying conditions, particularly acute coronary syndromes.
Postresuscitative care includes mitigation of reperfusion injury occurring after the period of ischemia. Postresuscitative care should begin immediately after restoration of spontaneous circulation is determined. To minimize hyperoxic damage to lungs, oxygen administration should be titrated down until a peripheral oxygen saturation (SpO2) of 94% is attained. Ventilation rate and volume should be titrated to an end-tidal carbon dioxide reading of 35 to 40 mm Hg. A fluid bolus should be administered if tolerated, and a vasopressor infusion should be given as necessary to maintain a systolic blood pressure > 90 mm Hg.
Postresuscitation laboratory studies include arterial blood gases (ABG), complete blood count (CBC), and blood chemistries, including electrolytes, glucose, BUN (blood urea nitrogen), creatinine, and cardiac biomarkers. (Creatine kinase is usually elevated because of skeletal muscle damage caused by CPR; troponins, which are unlikely to be affected by CPR or defibrillation, are preferred.) Arterial partial pressure of oxygen (PaO2) should be kept near normal values (80 to 100 mm Hg). Hematocrit should be maintained at ≥ 30%, and glucose at 140 to 180 mg/dL (7.7 to 9.9 mmol/L); electrolytes, especially potassium, should be within the normal range.
Coronary angiography
The decision to do cardiac catheterization after resuscitation from cardiac arrest should be individualized based on the electrocardiogram (ECG), the interventional cardiologist's clinical impression, and the patient's prognosis. Guidelines suggest doing emergency angiography for adult patients in whom a cardiac cause is suspected and who have ST-segment elevation myocardial infarction (STEMI) on ECG (1).
It is unclear whether emergency (within 2 hours) or more delayed (median approximately 120 hours after arrest) cardiac catheterization in patients without STEMI on ECG results is any clinical benefit (2). Some researchers advocate liberal use of cardiac catheterization after restoration of spontaneous circulation, doing the procedure on most patients unless the etiology is clearly unlikely to be cardiac (eg, drowning) or there are contraindications (eg, intracranial bleeding).
Neurologic support
Fewer than 10% of patients who survive out-of-hospital cardiac arrest have good central nervous system function (cerebral performance category [CPC] score 1 or 2—see table Cerebral Performance Category Scale) at hospital discharge (3, 4, 5). A CPC score of 1 is indicative of good cerebral performance (patient is conscious, alert, and able to work but may have mild neurologic or psychologic deficit). A CPC score of 2 is indicative of moderate cerebral performance (patient is conscious, able to do activities of daily living [ADLs], and work in a simple environment). Hypoxic brain injury is a result of ischemic damage and cerebral edema (see pathophysiology of cardiac arrest). Both damage and recovery may evolve over 48 to 72 hours after resuscitation.
Cerebral Performance Category Scale (Adult)*
Score | Category | Description |
|---|---|---|
1 | Normal (good cerebral performance) | Conscious, alert, able to work and lead a normal life May have minor psychologic or neurologic deficits (eg, mild dysphasia, non-incapacitating hemiparesis, minor cranial nerve abnormalities) |
2 | Moderate disability (disabled but independent) | Conscious, with sufficient cerebral function for part-time work in sheltered environment and independent activities of daily life (eg, dress, travel by public transportation, prepare food) May have hemiplegia, seizures, ataxia, dysarthria, dysphasia, or permanent memory or mental changes |
3 | Severe disability (conscious but disabled and dependent) | Conscious, but dependent on others for daily support; has at least limited cognition This category includes a wide range of neurologic dysfunction, from patients who are ambulatory but have severe memory disturbances or dementia that precludes independent existence to those who are paralyzed and can communicate only with their eyes (as in the locked-in syndrome). |
4 | Unconscious (coma or vegetative state) | Unconscious, unaware of surroundings, no cognition; no verbal or psychologic interaction with environment |
5 | Brain death | Meeting criteria for brain death or dead by traditional criteria |
* Worst level of performance for any single criterion is used for categorizing. Deficits are scored only if they result from a neurologic disorder. Assessments are based on medical records or an interview with the caretaker. | ||
Data from Safar P. Resuscitation after Brain Ischemia. In: Grenvik A, Safar P, editors. Brain Failure and Resuscitation. 1981. pp. 155–184 | ||
Maintenance of oxygenation and cerebral perfusion pressure (avoiding hyperventilation, hyperoxia, hypoxia, and hypotension) may reduce cerebral complications. Both hypoglycemia and hyperglycemia may damage the post-ischemic brain and should be treated.
In adults, targeted temperature management is recommended for patients who remain unresponsive after spontaneous circulation has returned (6, 7). Current recommendations are to target normothermia (< 37.5º C), although many researchers and clinicians continue to advocate for hypothermia (body temperature of 32 to 36° C). Regardless of the chosen target temperature, active temperature management is begun as soon as spontaneous circulation has returned. Techniques to induce and maintain hypothermia can be either external or internal. External cooling methods are easy to apply and range from the use of external ice packs to several commercially available external cooling devices that circulate high volumes of chilled water over the skin. For internal cooling, chilled IV fluids (4° C) can be rapidly infused to lower body temperature, but this method may be problematic in patients who cannot tolerate much additional fluid volume. Also available are external heat-exchange devices that circulate chilled saline to an indwelling IV heat-exchange catheter using a closed-loop design in which chilled saline circulates through the catheter and back to the device, rather than into the patient. Another internal method for cooling uses an extracorporeal device that circulates and cools blood externally then returns it to the central circulation. Regardless of the method chosen, the goal is to cool the patient rapidly and to maintain the core temperature at target (< 37.5º C for normothermia or between 32° C and 36° C for hypothermia) for 24 hours after restoration of spontaneous circulation. There is no evidence that any specific temperature within this range is superior, but it is imperative to avoid hyperthermia (1, 8).
Numerous pharmacologic treatments, including free radical scavengers, antioxidants, glutamate inhibitors, and calcium channel blockers, are of theoretic benefit. Many have been successful in animal models, but none has proved effective in human trials.
Blood pressure support
Current recommendations are to maintain a mean arterial pressure (MAP) of > 65 mm Hg and systolic blood pressure > 90 mm Hg (9). In patients known to be hypertensive, a reasonable target is systolic blood pressure 30 mm Hg below prearrest level. MAP is best measured with an intra-arterial catheter. Use of a flow-directed pulmonary artery catheter for hemodynamic monitoring has been largely discarded.
Blood pressure support includes
IV crystalloid infusion (normal saline or lactated Ringer's)
Inotropic or vasopressor medications with a goal of maintaining systolic blood pressure of at least 90 mm Hg and MAP of at least 65 mm Hg
Rarely intra-aortic balloon counterpulsation
Patients with low MAP and low central venous pressure should have an IV fluid challenge with 0.9% saline infused in 250-mL increments.

Although use of inotropic and vasopressor medications has not proved to enhance long-term survival, older adults with moderately low MAP (70 to 80 mm Hg) and normal or high central venous pressure may receive an infusion of an inotrope (eg, dobutamine started at 2 to 5 mcg/kg/minute). Amrinone or milrinone are alternatives that are rarely used (see table Although use of inotropic and vasopressor medications has not proved to enhance long-term survival, older adults with moderately low MAP (70 to 80 mm Hg) and normal or high central venous pressure may receive an infusion of an inotrope (eg, dobutamine started at 2 to 5 mcg/kg/minute). Amrinone or milrinone are alternatives that are rarely used (see tableMedications Commonly Used for Resuscitation).
If this therapy is ineffective, the inotrope and vasoconstrictor dopamine may be considered. Alternatives are epinephrine and the peripheral vasoconstrictors norepinephrine and phenylephrine (see table If this therapy is ineffective, the inotrope and vasoconstrictor dopamine may be considered. Alternatives are epinephrine and the peripheral vasoconstrictors norepinephrine and phenylephrine (see tableMedications Commonly Used for Resuscitation). However, vasoactive medications should be used at the minimal dose necessary to achieve low-normal MAP because they may increase vascular resistance and decrease organ perfusion, especially in the mesenteric bed. They also increase the workload of the heart at a time when its capability is decreased because of postresuscitation myocardial dysfunction.
If MAP remains < 70 mm Hg in patients who may have sustained a myocardial infarction (MI), intra-aortic balloon counterpulsation should be considered. Patients with normal MAP and high central venous pressure or widened inferior vena cava may improve with either inotropic therapy or afterload reduction with nitroprusside or nitroglycerin.(MI), intra-aortic balloon counterpulsation should be considered. Patients with normal MAP and high central venous pressure or widened inferior vena cava may improve with either inotropic therapy or afterload reduction with nitroprusside or nitroglycerin.
Intra-aortic balloon counterpulsation can assist low-output circulatory states due to left ventricular pump failure that is refractory to medication. A balloon catheter is introduced via the femoral artery, percutaneously or by arteriotomy, retrograde into the thoracic aorta just distal to the left subclavian artery. The balloon inflates during each diastole, augmenting coronary artery perfusion, and deflates during systole, decreasing afterload. Its primary value is as a temporizing measure when the cause of shock is potentially correctable by surgery or percutaneous intervention (eg, acute MI with major coronary obstruction, acute mitral regurgitation, ventricular septal defect).
Post-return of spontaneous circulation arrhythmia treatment
Although ventricular fibrillation (VF) or ventricular tachycardia (VT) may recur after resuscitation, prophylactic antiarrhythmic medications do not improve survival and are not routinely used. However, patients manifesting such rhythms may be treated with procainamide, lidocaine (see (VT) may recur after resuscitation, prophylactic antiarrhythmic medications do not improve survival and are not routinely used. However, patients manifesting such rhythms may be treated with procainamide, lidocaine (seeOther medications), or amiodarone (see ), or amiodarone (seeFirst-line medications) in addition to defibrillation.
Patients who had arrest caused by VF or VT not associated with acute myocardial infarction are candidates for an implantable cardioverter-defibrillator (ICD). ICDs are implanted similarly to pacemakers and have intracardiac leads and sometimes subcutaneous electrodes. They can sense arrhythmias and deliver either cardioversion or cardiac pacing as indicated.
Depending on the specific arrhythmia, postresuscitation rapid supraventricular tachycardias can be treated with medications used when such arrhythmias occur in other contexts.
Postresuscitative care references
1. Wyckoff MH, Greif R, Morley PT, et al: 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation 146(25):e483–e557, 2022. doi:10.1161/CIR.0000000000001095
2. Spoormans EM, Lemkes JS, Janssens GN, et al: Ischaemic electrocardiogram patterns and its association with survival in out-of-hospital cardiac arrest patients without ST-segment elevation myocardial infarction: a COACT trials' post-hoc subgroup analysis. Eur Heart J Acute Cardiovasc Care 11(7):535-543, 2022. doi:10.1093/ehjacc/zuac060
3. CARES: Cardiac Arrest Registry to Enhance Survival. CARES 2023 Annual Report. https://mycares.net/
4. Jennett B, Bond M: Assessment of outcome after severe brain damage. Lancet 1(7905):480–484, 1975. doi:10.1016/s0140-6736(75)92830-5
5. Safar P. Resuscitation after Brain Ischemia. In: Grenvik A, Safar P, editors. Brain Failure and Resuscitation. 1981. pp. 155–184.
6. Bernard SA, Gray TW, Buist MD, et al: Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 346:557–563, 2002. doi: 10.1056/NEJMoa003289
7. Nielsen N, Wetterslev J, Cronberg T, et al: Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med 369:2197–2206, 2013. doi: 10.1056/NEJMoa1310519
8. Granfeldt A, Holmberg MJ, Nolan JP, Soar J, Andersen LW; International Liaison Committee on Resuscitation (ILCOR) Advanced Life Support Task Force: Targeted temperature management in adult cardiac arrest: Systematic review and meta-analysis. Resuscitation 167:160–172, 2021. doi:10.1016/j.resuscitation.2021.08.040
9. Nolan JP, Sandroni C, Böttiger BW, et al: European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med 47(4):369–421, 2021. doi:10.1007/s00134-021-06368-4
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association 2020 CPR and ECC Guidelines: These guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) are based on the most recent review of resuscitation science, protocols, and education.







