



- Anal Cancer
- Benign Esophageal Tumors
- Colorectal Cancer
- Colorectal Cancer Screening
- Esophageal Cancer
- Familial Adenomatous Polyposis
- Gastrointestinal Stromal Tumors (GISTs)
- Lynch Syndrome
- MUTYH Polyposis Syndrome
- Pancreatic Cancer
- Peutz-Jeghers Syndrome
- Polyps of the Colon and Rectum
- Small-Bowel Tumors
- Stomach Cancer
An intestinal polyp is any mass of tissue that arises from the bowel wall and protrudes into the lumen. Most are asymptomatic except for minor bleeding, which is usually occult. The main concern is malignant transformation; most colon cancers arise in a previously benign adenomatous polyp. Diagnosis is by endoscopy. Treatment is endoscopic removal.
Topic Resources



Polyps may be sessile or pedunculated and vary considerably in size. Incidence of polyps ranges from 7 to 50%; the higher figure includes very small polyps (usually hyperplastic polyps or adenomas) found at autopsy. Polyps, often multiple, occur most commonly in the rectum and sigmoid and decrease in frequency toward the cecum. Multiple polyps may represent familial adenomatous polyposis. About 25% of patients with cancer of the large bowel also have satellite adenomatous polyps.
Adenomatous (neoplastic) polyps are of greatest concern. Such lesions are classified histologically as tubular adenomas, tubulovillous adenomas (villoglandular polyps), or villous adenomas. The likelihood of cancer in an adenomatous polyp at the time of discovery is related to size, histologic type, and degree of dysplasia; a 1.5-cm tubular adenoma has a 2% risk of containing a cancer vs a 35% risk in 3-cm villous adenomas. Serrated adenomas, a somewhat more aggressive type of adenoma, may develop from hyperplastic polyps.
Nonadenomatous (nonneoplastic) polyps include hyperplastic polyps, hamartomas (see Peutz-Jeghers Syndrome), juvenile polyps, pseudopolyps, lipomas, leiomyomas, and other rarer tumors. Juvenile polyps occur in children, typically outgrow their blood supply, and autoamputate some time during or after puberty. Treatment is required only for uncontrollable bleeding or intussusception. Inflammatory polyps and pseudopolyps occur in chronic ulcerative colitis and in Crohn disease of the colon. Multiple juvenile polyps (but not sporadic ones) convey an increased cancer risk. The specific number of polyps resulting in increased risk is not known.

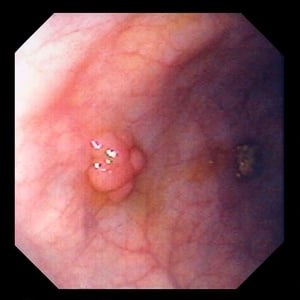
This image shows a sessile, multilobulated polyp, which, on biopsy, turned out to be a benign tubular adenoma.
Image provided by David M. Martin, MD.

This image shows a pedunculated polyp, which, on biopsy, turned out to be a benign tubular adenoma.
Image provided by David M. Martin, MD.

This image shows a sessile polyp, which, on biopsy, turned out to be a tubulovillous adenoma.
Image provided by David M. Martin, MD.
This image shows a sessile, multilobulated polyp, which, on biopsy, turned out to be a benign tubular adenoma.
Image provided by David M. Martin, MD.
This image shows a pedunculated polyp, which, on biopsy, turned out to be a benign tubular adenoma.
Image provided by David M. Martin, MD.
This image shows a sessile polyp, which, on biopsy, turned out to be a tubulovillous adenoma.
Image provided by David M. Martin, MD.
Symptoms and Signs of Colorectal Polyps
Most polyps are asymptomatic. Rectal bleeding, usually occult and rarely massive, is the most frequent complaint.
Cramps, abdominal pain, or obstruction may occur with a large lesion.
Rectal polyps may be palpable by digital examination. Occasionally, a polyp on a long pedicle may prolapse through the anus.
Large villous adenomas may rarely cause watery diarrhea that may result in hypokalemia.
Diagnosis of Colorectal Polyps
Colonoscopy
Diagnosis of colonic polyps is usually made by colonoscopy. Barium enema, particularly double-contrast examination, is effective, but colonoscopy is preferred because polyps also may be removed during that procedure. Because rectal polyps are often multiple and may coexist with cancer, complete colonoscopy to the cecum is mandatory even if a distal lesion is found by flexible sigmoidoscopy.
During colonoscopy, any polyps seen are removed and evaluated for possible cancer.
Treatment of Colorectal Polyps
Complete removal during colonoscopy
Sometimes follow with surgical resection
Follow-up surveillance colonoscopy
Polyps should be removed completely with a snare or biopsy forceps during total colonoscopy. If colonoscopic removal is unsuccessful, laparotomy should be done.
Subsequent treatment depends on the histology of the polyp. If dysplastic epithelium does not invade the muscularis mucosa, the line of resection in the polyp’s stalk is clear, and the lesion is well differentiated, endoscopic excision and close endoscopic follow-up should suffice. Patients with deeper invasion, an unclear resection line, or a poorly differentiated lesion should have segmental resection of the colon. Because invasion through the muscularis mucosa provides access to lymphatics and increases the potential for lymph node metastasis, such patients should have further evaluation (as in colon cancer).
The scheduling of follow-up examinations after polypectomy is controversial and varies by the number, size, and type of polyps removed (1). For example, guidelines recommend a repeat total colonoscopy (or barium enema if total colonoscopy is impossible) 3 years after removal of a tubular adenoma ≥ 10 mm or a villous adenoma of any size.
Treatment reference
1. Gupta S, Lieberman D, Anderson JC, et al: Recommendations for Follow-Up After Colonoscopy and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 115(3):415-434, 2020. doi: 10.14309/ajg.0000000000000544
Prevention of Colorectal Polyps
Aspirin and COX-2 inhibitors may help prevent formation of new polyps in patients with polyps or colon cancer (Aspirin and COX-2 inhibitors may help prevent formation of new polyps in patients with polyps or colon cancer (1). The potential benefits of long-term therapy with these agents must be weighed against the potential adverse effects (eg, bleeding, renal dysfunction).
Prevention reference
1. Cook NR, Lee IM, Zhang SM, et al: Alternate-day, low-dose aspirin and cancer risk: Long-term observational follow-up of a randomized trial. Ann Int Med 159:77–85, 2013. doi: 10.7326/0003-4819-159-2-201307160-00002
Key Points
Colonic polyps are common; the incidence ranges from 7 to 50% (depending on the diagnostic method used).
The main concern is malignant transformation, which occurs at different rates depending on the size and type of polyp.
The main symptom is bleeding, usually occult and rarely massive.
Colonoscopy is the recommended diagnostic and therapeutic procedure.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
U.S. Multi-Society Task Force on Colorectal Cancer: Recommendations for Follow-Up After Colonoscopy and Polypectomy: A Consensus Update (2020)







