



Topic Resources

Clinicians should evaluate the cause, severity, and nature of the pain and its effect on activities, mood, cognition, and sleep. Evaluation of the cause of acute pain (eg, back pain, chest pain) differs from that of chronic pain.
(See also Overview of Pain.)
The history should include the following information about the pain:
Timing (onset, persistence [whether constant or intermittent], pattern and degree of fluctuation and frequency of remissions, duration)
Quality (eg, sharp, dull, crampy, burning, aching, shooting)
Severity
Location (localized, diffuse, deep, superficial)
Radiation pattern
Exacerbating and relieving factors
Information from the history and physical examination help guide choice of laboratory and imaging tests to identify possible causes of pain.
Clinicians should assess the patient’s level of function and the pain's effect on function, focusing on activities of daily living (eg, dressing, bathing), employment, avocations, and personal relationships (including sexual).
A personal or family history of chronic pain can often illuminate the current problem. Whether family members perpetuate chronic pain (eg, by constantly asking about the patient's health) should be considered.
The patient's perception of pain and other factors may influence the clinical presentation. What pain means to the patient should be determined, with emphasis on psychologic issues, depression, and anxiety. Reporting pain may be more socially acceptable than reporting anxiety or depression, and appropriate therapy often depends on identifying any additional issues. Pain and suffering should also be distinguished, especially pain in cancer patients; suffering may be due as much to loss of function and fear of impending death as to pain.
In some patients, secondary gain (external, incidental benefits of a disorder—eg, time off, disability payments) may contribute to pain or pain-related disability.
Patients and sometimes family members and caregivers should be asked about the use, efficacy, and adverse effects of prescription and over-the-counter drugs and other treatments. If misuse of opioids or other substances is suspected, further evaluation is required.
Pain severity
Pain severity should be assessed before and after potentially painful interventions. In verbal patients, self-report is the gold standard, and external signs of pain or distress (eg, crying, wincing, rocking) are secondary. For patients who have difficulty communicating and for young children, nonverbal indicators (behavioral and sometimes physiologic) may need to be the primary source of information.
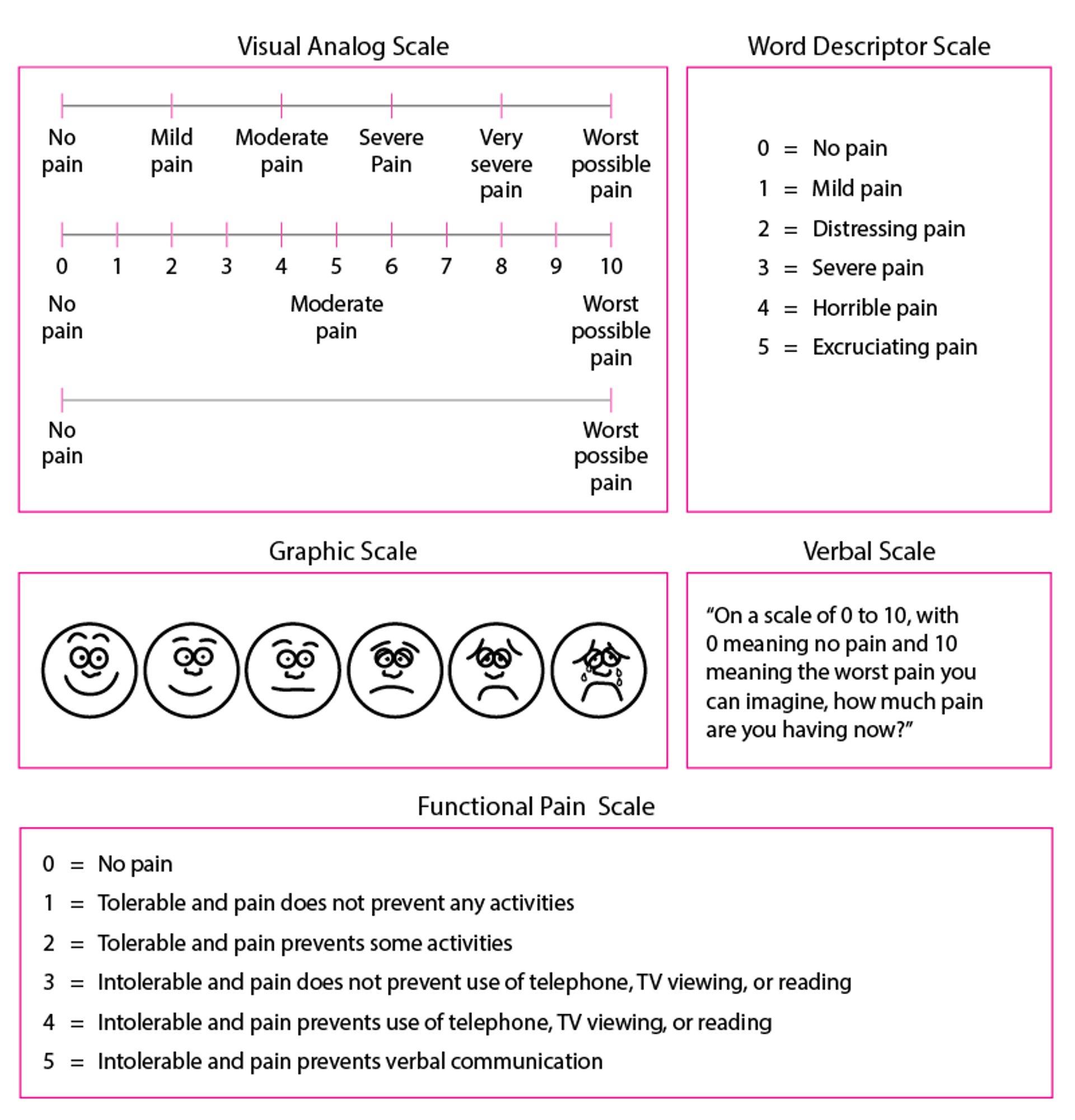
Formal measures (see figure Some pain scales for quantifying pain as it is occurring) include
Verbal category scales (eg, mild, moderate, severe)
Numeric scales
The Visual Analog Scale (VAS)
For a numeric scale, patients are asked to rate their pain from 0 to 10 (0 = no pain; 10 = “the worst pain ever”). For the VAS, patients make a hash mark representing their degree of pain on an unmarked 10-cm line with the left side labeled “no pain” and the right side labeled “unbearable pain.” The pain score is distance in mm from the left end of the line. Children and patients with limited literacy or known developmental problems may select from images of faces ranging from smiling to contorted with pain or from fruits of varying sizes to convey their perception of pain severity. When measuring pain, the examiner should specify a time period (eg, “on average during the past week”).
Some pain scales for quantifying pain as it is occurring
For the Functional Pain Scale, examiners should clearly explain to the patient that functional limitations are relevant to the evaluation only if they are due to the pain being evaluated; treatment aims to relieve pain as much as possible, at least to a tolerable level (0–2). Adapted from the American Geriatrics Society (AGS) Panel on Chronic Pain in Older Persons: The management of chronic pain in older persons. Journal of the American Geriatrics Society 46:635–651, 1998; used with permission; from Gloth FM III, Scheve AA, Stober CV, et al: The functional pain scale (FPS): Reliability, validity, and responsiveness in a senior population. Journal of the American Medical Directors Association 2 (3):110–114, 2001; and from Gloth FM III: Assessment. In Handbook of Pain Relief in Older Adults: An Evidence-Based Approach, edited by FM Gloth III. Totowa (NJ), Humana Press, 2003, p. 17; used with permission; copyright © FM Gloth, III, 2000. |

Patients with dementia or aphasia
Assessing pain in patients with disorders affecting cognition, speech, or language (eg, dementia, aphasia) can be difficult. Pain is suggested by facial grimacing, frowning, or repetitive eye blinking. Sometimes caregivers can describe behaviors that suggest pain (eg, sudden social withdrawal, irritability, grimacing). Pain should be considered in patients who have difficulty communicating and who inexplicably change their behavior. Many patients who have difficulty communicating can communicate meaningfully when an appropriate pain scale is used. For example, the Functional Pain Scale has been validated and can be used in nursing home patients who have Mini-Mental State Examination scores of ≥ 17.
Patients receiving neuromuscular blockade
No validated instruments are available to assess pain when neuromuscular blockade is used to facilitate mechanical ventilation.
If the patient is given a sedative, the dose can be adjusted until there is no evidence of consciousness. In such cases, specific analgesics are not needed. If, however, the patient is sedated but continues to have evidence of consciousness (eg, blinking, some eye movement, response to command), pain treatment should be considered based on the degree of pain usually caused by the condition (eg, burns, trauma). If a potentially painful procedure (eg, turning a bedbound patient) is required, pretreatment with the selected analgesic or anesthetic should be given.







