


Relapsing polychondritis is a rare systemic rheumatic disease characterized by episodes of inflammation of the cartilage of the ear and nose and sometimes other tissues and organs.
Affected ear or nose cartilage becomes inflamed and tender.
Other cartilage in the body can be damaged, leading to various symptoms, such as red or painful eyes, hoarseness, cough, difficulty breathing, rashes, and pain around the breastbone.
The results of blood, laboratory, and imaging tests may be used for diagnosis.
If symptoms or complications are severe, corticosteroids and other immunosuppressants usually help.
This disorder affects men and women equally, usually in middle age.
The cause of relapsing polychondritis is unknown, but an autoimmune reaction to cartilage is suspected. In an autoimmune disease, antibodies or cells produced by the body attack the body’s own tissues.
Symptoms of Relapsing Polychondritis
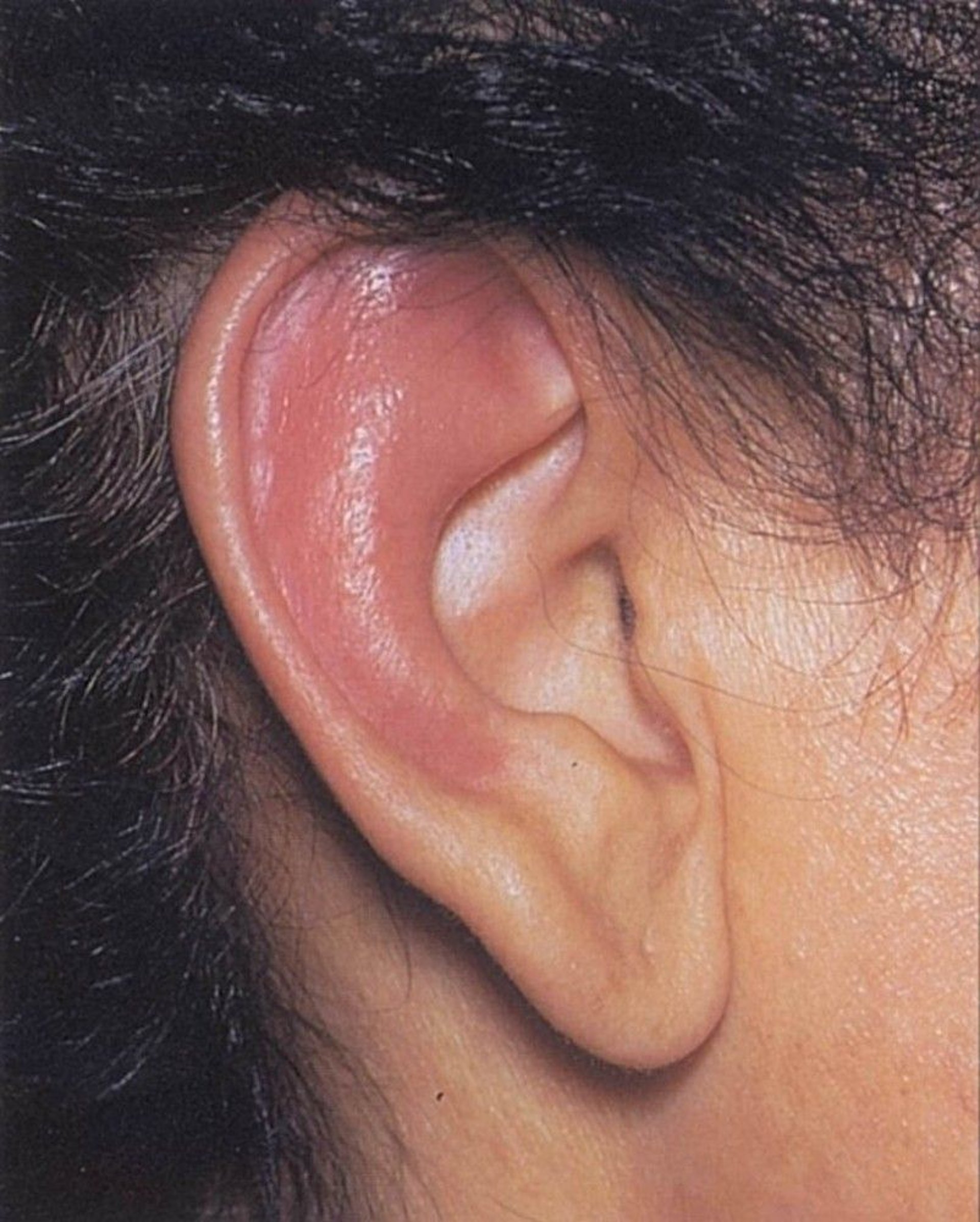
Typically, the cartilage (pinna) of one or both ears (but not the ear lobes) becomes red, swollen, and very painful.
Cartilage in the nose is the next most common site of inflammation. The nose may become tender, and cartilage can collapse.
At the same time or later, a person can develop joint inflammation (arthritis) and pain, which may be mild or severe. Cartilage in any joint may be affected, and the knees and the cartilage that connects the ribs to the breastbone are often affected.

© Springer Science+Business Media
Other affected sites include the eyes, resulting in inflammation. Rarely, the cornea may develop a hole (perforation), resulting in blindness. The middle and inner ears may be affected, leading to hearing loss. The voice box (larynx), windpipe (trachea), or airways of the lungs can be affected, resulting in hoarseness, a nonproductive cough, shortness of breath, and tenderness over the Adam’s apple. Less often, the heart is involved, leading to heart murmurs and occasionally to heart failure. Rarely, the kidneys and skin are affected.
Flare-ups of inflammation and pain last days to months, subside, then recur over a period of several years. Eventually, the supporting cartilage can be damaged, resulting in floppy or cauliflower ears, a sloping saddle nose, and a hollow at the lower part of the chest (pectus excavatum). The nerve in the inner ear can be affected, causing eventual problems with balance and hearing, and eventually vision problems can occur.
Diagnosis of Relapsing Polychondritis
Symptoms
Blood and other tests
Rarely biopsy
To diagnose relapsing polychondritis, doctors examine the person and do tests to rule out other disorders that cause similar symptoms.

Blood tests, such as the erythrocyte sedimentation rate, can detect evidence of inflammation. Blood tests also reveal whether the person has a low number of red blood cells or a high number of white blood cells and whether certain antibodies are present. Although blood test results can help doctors diagnose relapsing polychondritis, they alone cannot confirm a definite diagnosis of relapsing polychondritis because sometimes the abnormalities they detect are present in healthy people or in people who have other disorders.
Doctors also evaluate the airways with tests that include spirometry (see Lung volume and flow rate measurements) and computed tomography (CT) of the chest.
Doctors may do echocardiography to evaluate the heart.
Rarely, doctors do a biopsy of inflamed cartilage to confirm the diagnosis.
Treatment of Relapsing Polychondritis
Corticosteroids
Sometimes other immunosuppressants for severe disease
Mild relapsing polychondritis of the ear or nose can be treated with nonsteroidal anti-inflammatory drugs
Surgery may be needed to correct collapse or narrowing of the trachea.
People who take corticosteroids are at risk of fractures related to osteoporosis. To prevent osteoporosis, these people are given and sometimes medications for osteoporosis.
People who are receiving immunosuppressants are also given medications to prevent infections such as by the fungus Pneumocystis jirovecii (see prevention of pneumonia in people with a weakened immune system) and vaccines against common infections such as pneumonia, influenza, and COVID-19.
Prognosis for Relapsing Polychondritis
Newer therapies have decreased the rate of death.
Death may result if the cartilage in the airways collapses, blocking the flow of air, or if the heart and blood vessels are severely damaged.







