



Stupor is unresponsiveness from which a person can be aroused only by vigorous, physical stimulation. Coma is unresponsiveness from which a person cannot be aroused and in which the person's eyes remain closed, even when the person is stimulated.
Topic Resources



Stupor and coma are usually caused by a disorder, a medication, illicit drugs, or an injury that affects large areas on both sides of the brain or specialized areas of the brain involved in maintaining consciousness.
A physical examination, blood tests, brain imaging, and information from family and friends help doctors identify the cause.
Doctors correct causes if possible, and take measures to support breathing and other body functions (such as mechanical ventilation) and to reduce pressure within the skull if it is increased.
Recovery from coma depends largely on the cause.
Control of consciousness
Normally, the brain can quickly adjust its own levels of activity and consciousness as needed. The brain makes these adjustments based on information it receives from the eyes, ears, skin, and other sensory organs. For example, the brain can adjust its metabolic activity (energy level) and induce sleep.
Whether a person is awake (wakefulness) is controlled by the upper part of the brain stem (the part of the brain that connects the cerebrum with the spinal cord) through a system of nerve cells and fibers (the reticular activating system). The cerebrum (the largest part of the brain) interacts with the upper part of the brain stem to maintain consciousness and alertness. The cerebrum consists of two parts (the right and left hemispheres).
The brain’s ability to adjust its activity and consciousness levels is impaired when
Both cerebral hemispheres malfunction, particularly when they are suddenly and severely damaged.
The reticular activating system malfunctions.
The brain’s ability to adjust its activity and consciousness levels is also impaired in the following situations:
When people are severely deprived of sleep
When and immediately after a seizure occurs
When blood flow or the amount of nutrients (such as oxygen or sugar) going to the entire brain decreases
When blood flow going to certain parts of the brain decreases, as occurs in certain strokes
When toxic substances damage nerve cells in the brain or make them function less well
When bleeding or swelling due to brain tumors or injury puts pressure on parts of the brain
Toxic substances may be taken into the body (for example, by consuming or inhaling them). Or they may be produced in the body as a waste product of normal processes but are not broken down and removed as they normally are.
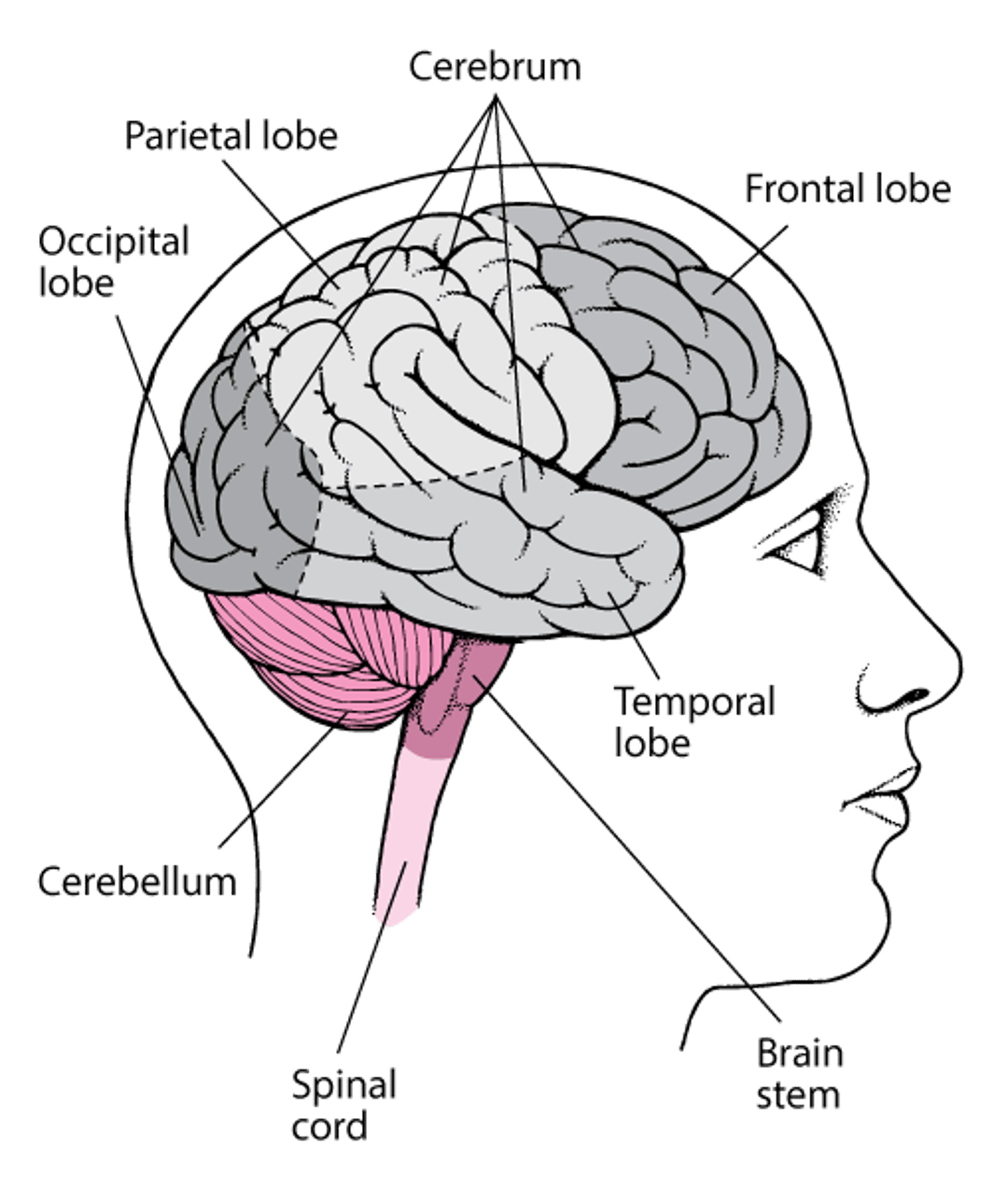
Viewing the Brain
The brain consists of the cerebrum, brain stem, and cerebellum. Each half (hemisphere) of the cerebrum is divided into lobes. |

Levels of impaired consciousness
Periods of impaired consciousness can be short or long. The degree of impairment can range from slight to severe. Doctors use various terms to describe the different levels of consciousness:
Lethargy is a slight reduction in alertness or mild mental fogginess (clouding of consciousness). People tend to be less aware of what is happening around them and to think more slowly than usual. They may feel tired and lack energy.
Obtundation, an imprecise term, refers to a moderate reduction in alertness or moderate clouding of consciousness.
Delirium is a disturbance of consciousness and mental function that occurs suddenly, typically fluctuates, and can usually be reversed. People cannot pay attention or think clearly. They are disoriented and may not know where they are or what time it is. They may be overly alert, attentive, and able to think clearly one moment and be sluggish, distracted, and confused the next.
Altered mental status, a very imprecise term, is sometimes used by doctors to refer to a change in consciousness, such as lethargy, obtundation, delirium, or sometimes stupor or coma.
Stupor is an excessively deep state of unresponsiveness. People can be aroused from it only briefly by vigorous stimulation, such as repeated shaking, loud calling, or pinching.
Coma is a state of complete unresponsiveness (except for certain automatic reflexes). People cannot be aroused at all. Their eyes stay closed. People in a deep coma lack purposeful responses, such as moving a limb away from something that hurts.
Causes of Stupor and Coma
The various levels of impaired consciousness—lethargy, obtundation, stupor, and coma—have the same causes, of which there are many.
Most commonly, the cause is
A toxic substance, such as carbon monoxide
A medication or illicit drug, such as an opioid or a sedative
A metabolic abnormality, such a very low blood sugar level (hypoglycemia) or very high blood sugar level (hyperglycemia)
A disorder that makes nerve cells in the brain malfunction and communicate less well, such as liver failure or kidney failure
A severe infection in or around the brain, such as meningitis or a brain abscess
A severe infection elsewhere in the body, such as sepsis (a bodywide infection)
Severe or prolonged seizures
Inadequate blood flow to the brain, as occurs when the heart stops (cardiac arrest)
Head injuries, such as concussion or bleeding in or around the brain
Disorders that increase pressure within the skull (intracranial pressure), including certain brain tumors and strokes
Disorders
Some disorders interfere with the delivery of needed substances to the brain or with the body’s ability to use them. Examples are
A very low or very high blood sugar level (hypoglycemia or hyperglycemia)
A very low level of oxygen in the blood, as occurs in respiratory (lung) failure or heart failure
The sudden stopping of the heart’s pumping (cardiac arrest) or breathing (respiratory arrest)
Blood delivers oxygen and essential nutrients (such as fats, sugars, minerals, and vitamins) to the body's tissues. Thus, when blood flow to the brain is decreased, the brain is deprived of oxygen and essential nutrients. The brain may also be deprived of oxygen when the lungs are not functioning normally, as occurs in respiratory failure. The brain can be deprived of nutrients when a disorder (such as hypoglycemia) causes levels of nutrients in the blood to be low.
Having diabetes increases the risk of stupor or coma because diabetes can cause the blood sugar level to become too high or, when treatment is too aggressive, too low. When blood sugar levels are very high, people become dehydrated, causing the brain to function less well. When blood sugar levels are low, the brain is deprived of its main source of energy (sugar) and can malfunction or become damaged. Over time, diabetes damages the blood vessels and nerve cells in the brain. As a result, the brain may not get enough oxygen, and brain tissue may die.
Other disorders can cause cells throughout the body to malfunction. Often, brain cells are affected the most. These disorders include
An underactive thyroid gland (hypothyroidism)
A very low or high body temperature (hypothermia or hyperthermia)
Infections, such as sepsis, meningitis, and viral infections, including encephalitis, COVID-19, and severe acute respiratory syndrome (SARS)
Other common causes are disorders that affect the areas of the brain that control consciousness. These disorders include the following:
A head injury may jar but not physically damage these areas, directly damage them, or indirectly damage them by causing bleeding (hemorrhage) in or around the brain.
Strokes and tumors can also directly damage areas of the brain that control consciousness.
Any disorder that increases pressure within the skull (intracranial pressure) can impair consciousness. A mass in the brain, such as an accumulation of blood (hematoma), a tumor, or an abscess, can impair consciousness indirectly by putting pressure on the areas of the brain that control consciousness.
A structural abnormality can block the flow of cerebrospinal fluid in the brain, increasing pressure within the skull. Cerebrospinal fluid is the fluid that flows through the tissues covering the brain and spinal cord and fills the spaces within the brain. Some structural abnormalities are present at birth.
A large mass can push the brain against the relatively rigid structures inside the skull, damaging brain tissue. If the areas of the brain that control consciousness are affected, stupor or coma results. If the pressure is high enough, the brain may be forced through a small natural opening in the relatively rigid sheets of tissue that separate the brain into compartments. This life-threatening disorder is called brain herniation. Herniation can further damage brain tissue, making an already dire condition worse.
Having had a stroke or having another disorder that affects brain function makes the brain more susceptible to other disorders that can impair consciousness.
Substances
Commonly, consciousness is impaired by drinking too much alcohol or taking too much of certain medications or illicit drugs, such as sedatives and opioids (narcotics). In addition to making brain cells function slowly, alcohol and some medications and illicit drugs can damage brain cells indirectly. They can slow breathing so much that the oxygen level in blood becomes low enough to cause brain damage.
Taking several medications (to treat several disorders) is also a common cause, partly because taking several medications increases the risk of interactions between medications.
Overdoses of marijuana, including medical marijuana, sometimes causes the brain to malfunction, resulting in impaired consciousness and sometimes seizures.
Occasionally, taking certain antipsychotic medications results in an unresponsive state called neuroleptic malignant syndrome. This syndrome is characterized by muscle rigidity, fever, and high blood pressure, as well as changes in mental function (such as confusion and lethargy).
Mental health disorders and stress
Occasionally, people who have a mental health disorder or those who are psychologically stressed may appear unresponsive. For example, people who learn that they have cancer or that their spouse is going to leave them may collapse and not respond when they are spoken to or touched. Yet, such people may be aware of what is happening around them, and their brain may be functioning normally.
Based on the results of the examination, doctors can usually determine how much a mental health disorder or psychological distress contributes to what appears to be impaired consciousness and whether the person is pretending.
Older age
Aging alone does not increase the risk of impaired consciousness. However, age-related changes make impaired consciousness in older adults a particular concern (see Essentials for Older Adults: Stupor and Coma). For example, some disorders that are more common among older adults (such as high blood pressure or diabetes) can increase the risk of impaired consciousness if another problem develops.
Common problems that can trigger impaired consciousness in older adults include
Reactions to medications
Infections
Development of a new disorder (such as stroke or heart failure) or worsening of a disorder they already have
Some Causes of Stupor and Coma
Condition | Process | Effects |
|---|---|---|
Brain disorders | ||
Seizures that recur frequently or last a long time can
Such seizures can damage brain tissue. | Consciousness is often impaired during a seizure. After a seizure, most people feel sluggish (lethargic) and confused, and some feel weak or are paralyzed. They may remain that way for minutes to hours after the seizure. | |
Strokes occur when blood flow to parts of the brain, including to the brain stem, are blocked. | If blood flow to the upper brain stem is blocked, consciousness may be suddenly lost, and coma can result. If blood flow to the entire brain stem is blocked and not restored within several minutes, most or all of the brain stem is damaged, and death may result. | |
Strokes may result from bleeding in the brain (intracerebral hemorrhage) or between the layers of the tissue covering the brain (subarachnoid hemorrhage). Blood can directly damage or increase pressure on brain tissue. | Consciousness may be impaired, and coma may result. Seizures may also occur. Even a small amount of bleeding in the brain stem can cause coma. | |
A large tumor or abscess can push the brain against the relatively rigid structures inside the skull and put pressure on brain tissue, causing it to malfunction. Sometimes the pressure pushes brain tissue through a natural opening in the relative rigid sheets of tissue that divide the brain into parts. This abnormal protrusion of brain tissue is called brain herniation. Tumors can directly invade and damage brain tissue and cause swelling that disrupts communication between different areas of the brain. | If the areas of the brain that control consciousness are affected, coma results. | |
Other disorders | ||
Cardiac arrest or respiratory arrest | In cardiac arrest, the heart stops pumping. As a result, not enough blood reaches the brain, and the brain is deprived of oxygen because blood delivers oxygen to the body's tissues. In respiratory arrest, the person stops breathing. As a result, not enough oxygen enters the blood and the brain is deprived of oxygen. Usually, cardiac and respiratory arrest occur together. | Consciousness is lost within a minute or 2. If people are deprived of oxygen for even 4 to 5 minutes, the lack of oxygen triggers death of nerve cells in certain parts of the brain. Coma results and may quickly become irreversible. |
Heart or lung disorders if severe | Severe heart disorders (such as heart failure) can reduce blood flow to the brain. Severe lung disorders (such as chronic obstructive pulmonary disease, pulmonary edema, pulmonary embolism, and severe and long-lasting asthma attacks) can reduce the amount of oxygen in the blood. | With either type of disorder, the brain may not receive enough oxygen. Lack of oxygen can cause delirium or coma, depending on how much oxygen is in the blood. |
If the kidneys or liver cannot remove toxic waste products from the blood as they normally do, waste products accumulate in the blood and cause the brain to malfunction. | Treating chronic kidney or liver failure can usually reverse the coma that they cause. If coma results from acute, severe liver failure, the brain swells because fluid accumulates in brain cells. Death often results. | |
Over time, high blood pressure damages blood vessels in the brain. | If blood vessels in the brain are damaged, blood flow and oxygen supply to the brain are reduced. Also, damaged blood vessels may burst, resulting in a stroke (due to bleeding in the brain). | |
Metabolic abnormalities | ||
Diabetes may cause the blood sugar level to become too high (hyperglycemia) or, when treatment is too aggressive, too low (hypoglycemia—see below). Also, when there is not enough insulin (as may occur in type 1 diabetes), the body breaks fat cells down to produce energy. During this process, ketones are produced. Ketones make the blood too acidic (a condition called diabetic ketoacidosis). | Stupor or coma can result. Without treatment, diabetic ketoacidosis or hypoglycemia can result in coma and death. | |
The blood sugar level is abnormally high. High blood sugar levels can cause dehydration, drawing fluid from the brain and causing it to shrink. | Stupor or coma can result. | |
The blood sugar level is abnormally low. The brain malfunctions or is damaged if it is deprived of sugar, which is its main source of energy in combination with oxygen. | Coma can result. People with hypoglycemia must be treated immediately to prevent permanent brain damage or death. Treatment consists of giving them glucose (a sugar) intravenously | |
The blood sodium level is high. Hypernatremia is usually due to dehydration and can reduce the amount of water in brain cells. | An abnormal amount of water in brain cells interferes with chemical reactions there. Stupor or coma may result. | |
The blood sodium level is low. Hyponatremia may be due to the following:
Hyponatremia can increase the amount of water in brain cells and cause the brain to swell. | An abnormal amount of water in brain cells interferes with chemical reactions there. Whether the brain is damaged and how badly it is damaged depends on how quickly the amount of water in brain cells increases. If the amount increases slowly. the brain may be able to adjust, and damage is usually avoided. | |
The thyroid gland is underactive. | Untreated hypothyroidism may cause mental confusion and slowed thinking. The confusion may progress to stupor and coma. | |
Deficiency of a nutrient, such as thiamin or certain electrolytes or minerals (such as magnesium) | Deficiency of the vitamin thiamin or a mineral such as magnesium causes nerve cells in the brain to malfunction. Some minerals (including magnesium) are also electrolytes. Electrolytes help regulate nerve and muscle function and maintain acid-base balance in the body. | Thiamin deficiency may result in confusion, stupor, and coma. The eye muscles may not work normally, resulting in double vision. Very low or high levels of certain electrolytes or minerals (such as magnesium) can cause sleepiness, weakness, and, rarely, seizures and coma. |
Infections | ||
Encephalitis (infection of the brain) Meningitis (infection of the layers of tissue covering the brain and spinal cord) Sepsis (a serious bodywide response to a bloodstream infection) Severe acute respiratory syndrome (SARS) Urinary tract infections in older adults | If brain tissue becomes infected, the brain may malfunction. Other infections, such as sepsis, can cause high fevers, which may make the brain malfunction or may damage brain tissue. Age-related changes in the brain make older adults more susceptible to disturbances in mental function caused by minor disorders, such as urinary tract infections. | Coma may result. In older adults, urinary tract infections can cause confusion, disorientation, and delirium. |
Accidents and injuries | ||
Asphyxiation | The brain is deprived of oxygen. | Consciousness is quickly lost, and coma and death may follow. |
Head injuries may damage the brain in the following ways:
Blood may directly irritate brain tissue or may accumulate as a mass (hematoma), which puts pressure on the brain (as in epidural or a subdural hematoma). | Depending on the injury, coma may develop immediately or gradually over several hours. Seizures may also result, particularly if a large amount of blood leaks from blood vessels and comes into direct contact with brain tissue, irritating it. | |
A body temperature above 104° F (40° C), as occurs in high fevers or heatstroke, can damage the brain. | Coma can result. Nerve cells die much more quickly when body temperature is very high. | |
A body temperature below 96.8° F (36° C) slows brain function. A body temperature below 80° F (26.7° C) causes coma. However, low temperatures can sometimes protect the brain by slowing the damage caused by lack of blood or oxygen. Also, nerve cells die much more slowly when body temperature is very low. For example, a child may fully recover after being submersed for 30 minutes in an icy lake. Being submersed that long in warm water is usually fatal. | Stupor or coma can result, but if people survive, there is usually no permanent damage. | |
Substances | ||
Alcohol slows brain function. Consumed in large amounts, it may affect brain tissue directly or indirectly by slowing breathing so much that the oxygen level in blood becomes low enough to cause brain damage. | A high blood alcohol level, especially when it exceeds 0.2%, can cause stupor or coma. | |
Carbon monoxide or similar substances inhaled in large amounts | Carbon monoxide attaches to the hemoglobin in red blood cells. It takes the place of oxygen and prevents red blood cells from carrying oxygen to tissues, including the brain. | Severe carbon monoxide poisoning can cause coma or irreversible brain damage because the brain does not receive enough oxygen. |
Medications and illicit drugs | Many medications and illicit drugs, even if not given in high doses, can slow brain function, sometimes by slowing breathing. They include
| Coma can result. If treated early, this type of coma can be completely reversed. |
Symptoms of Stupor and Coma
Consciousness is impaired to varying degrees. People in a stupor are usually unconscious but can be aroused with vigorous stimulation. People in a coma are unconscious, with their eyes closed, and they cannot be aroused.
The brain damage or dysfunction that causes stupor and coma affects other parts of the body.
The pattern of breathing is usually abnormal. People may breathe too rapidly, too slowly, too deeply, or irregularly. Or they may alternate between these abnormal patterns.
Blood pressure may increase or decrease, depending on the cause of the impaired consciousness. For example, if a head injury causes massive bleeding in the brain, pressure within the skull rapidly increases, and blood flow to the brain decreases. The nerves that control blood pressure respond by increasing blood pressure to try to maintain normal blood flow to the brain. If the cause of impaired consciousness is a severe infection, severe dehydration, major blood loss, overdoses of certain medications or illicit drugs, or cardiac arrest, blood pressure decreases dramatically.
Muscles may contract and remain contracted in unusual positions. For example, the head may be tilted back with the arms and legs extended—a position called decerebrate rigidity. Or the arms may be flexed with both legs extended—a position called decorticate rigidity. Or the entire body may be limp. Sometimes muscles contract sporadically or involuntarily.
The eyes may be affected. One or both pupils of the eyes may be widened (dilated) and may not react to changes in light. Or the pupils may be tiny. The eyes may not move or may move in abnormal ways.
The disorder that is impairing consciousness may cause other symptoms. For example, if the cause is meningitis (infection of the layers of tissue covering the brain and spinal cord), early symptoms may include fever, vomiting, headache, and a painful, stiff neck that makes lowering the chin to the chest difficult or impossible.
Being unable to move (immobilization) for a long time, as occurs in coma, can also cause problems, such as pressure sores, nerve damage in the limbs, blood clots, and urinary tract infections (see Problems Due to Bed Rest).
Diagnosis of Stupor and Coma
A doctor's evaluation
Neurologic examination
Laboratory and imaging tests
Doctors can tell that consciousness is impaired based on observation and examination. Doctors try to identify the parts of the brain that are impaired and the cause of impairment because treatment differs and because impairment may progress, leading to coma and brain death.
Stupor is diagnosed when vigorous, repeated attempts arouse the person only briefly. Coma is diagnosed when the person cannot be aroused at all and the eyes remain closed.
People who become stuporous or comatose must be taken to the hospital immediately because either state may be caused by a life-threatening disorder. Health care practitioners try to identify the cause and provide emergency medical care at the same time. For example, a quick test is done to estimate the blood sugar level. Then if people have a low blood sugar level (which can quickly and permanently damage the brain), it can be treated immediately.
A stuporous or comatose person cannot communicate. So the doctor usually checks whether the person is wearing a medical alert identification bracelet or necklace, which may suggest the cause. The doctor may check the person's wallet, purse, or pockets for medical identification (such as a hospital identification card and a list of medications the person is taking), which may also help identify the cause. Thus, a person with a disorder that increases the risk of stupor or coma (such as diabetes or a seizure disorder) should carry or wear some form of medical identification.
The doctor asks any witnesses of the change in consciousness about the circumstances in which it occurred and any other symptoms the person had. For example, if the person's limbs jerked repeatedly when consciousness was affected, the cause may have been a seizure. The doctor also talks to family members and friends, who should honestly provide emergency medical personnel or the doctor with any relevant information about the person, which includes the following:
Whether the person uses medications, illicit drugs, alcohol, or other toxic substances and which ones are used
Whether the person was injured before the change in consciousness
When and how the problem began
Whether the person has or has had any infections, other disorders (such as diabetes, high blood pressure, a seizure, or a thyroid, kidney, or liver disorder), or other symptoms (such as headaches or vomiting)
When the person last seemed normal
Whether the person had eaten any unusual foods or been traveling
Whether they have any hunches about what might be the cause (for example, if the person was recently depressed or talked about suicide)
This information can help doctors identify possible causes and helps them assess how likely the person is to recover. Many such causes would not be identified, even with extensive diagnostic testing, if this information was unavailable. For example, if people have eaten unusual foods, the cause may be a toxin (such as those in poison mushrooms). If people have traveled recently, the cause may be an infection that is common in the area they visited. If empty pill containers or paraphernalia for taking illicit drugs were found nearby, the cause may be a substance overdose. If a medication, illicit drug, or toxic substance was ingested, family members or friends should give a sample of that substance or its container to the doctor if possible.
Did You Know...
|
Information from the family and friends is usually valuable and is more likely to lead to the correct diagnosis than examination or testing. For example, no test can rule out all possible substance overdoses.
Physical examination
Body temperature is checked. An abnormally high temperature may indicate infection, heatstroke, or an overdose of a substance that stimulates the body (such as cocaine or an amphetamine). An abnormally low temperature may indicate prolonged exposure to cold, an underactive thyroid gland, alcohol intoxication, a sedative overdose or, in older adults, infection.
Doctors examine the head, face, and skin for clues to the cause, such as the following:
Black eyes, cuts, bruises, or leakage of cerebrospinal fluid (the fluid that surrounds the brain) from the nose or ears suggests a head injury.
Needle marks suggest an overdose of a substance, such as heroin.
Fever with a rash often suggests an infection, such as sepsis (a serious bodywide response to a bloodstream infection) or a brain infection.
Certain odors on the breath suggest diabetic ketoacidosis or consumption of a poison or large amounts of alcohol.
If people have bitten their tongue, seizures may be the cause.
Neurologic examination
A thorough neurologic examination is done. This examination helps doctors determine
How severely consciousness is impaired
Whether the brain stem is functioning normally
What part of the brain is damaged
What the cause may be
If people are unconscious, doctors try to rouse them first by speaking to them, then by touching their limbs, chest, or back. If these measure do not work, doctors use stimuli that cause discomfort or pain, such as pressure on a nail bed or a pinch. If people open their eyes or grimace when a painful stimulus is applied or if they purposefully withdraw from it, consciousness is not severely impaired. If people can make sounds, the cerebral hemispheres are functioning to some degree. If the eyes open, some parts of the brain stem are probably functioning.
Doctors sometimes use a standardized scoring system, such as the Glasgow Coma Scale, to help track changes in a person's level of consciousness. This scale assigns points based on responses to stimuli. Eye movement, speech, and movements are evaluated. This scale is a relatively reliable, objective measure of how unresponsive people are.
Abnormal breathing patterns can provide clues to which parts of the brain are malfunctioning.
Checking responses to painful stimulation can help determine whether parts of the brain and spinal cord are malfunctioning. When coma is present, using painful stimuli may trigger unusual body positions. For example, the head may be tilted back with the arms and legs extended (called decerebrate rigidity). Or the arms may be flexed with both legs extended (called decorticate rigidity). This test helps identify the area of the brain that is not functioning normally.
Limpness of the entire body and no movements in response to pain are the worst possible response. They indicate severe dysfunction in the central nervous system (brain and spinal cord). However, if muscle tone and movements return, the cause may be a reversible one, such as a sedative overdose.
Automatic reflexes in specific parts of the body are checked by maneuvers, such as striking the joints with a reflex hammer. Doctors check for differences in the strength of reflexes in different parts of the body. This information sometimes helps them identify which areas of the brain are not functioning normally.
All automatic reflexes are normal if unresponsiveness is caused by a mental health disorder that does not impair consciousness.
The eyes also provide important clues about how well the brain stem is functioning and what may be impairing consciousness. Doctors check the position of the pupils, their size, their reaction to bright light, their ability to follow a moving object (in people who are alert and awake), and the appearance of the retina. Normally, pupils widen (dilate) when light is dim and become smaller (constrict) when light is shined on them. However, the pupils may not respond normally to light in people in a coma. How the pupils respond to light or whether they respond helps doctors determine the cause of the coma.
To accurately evaluate the person, doctors need to know whether the person takes a medication to treat glaucoma, which can affect pupil size, and they usually need to know whether the person’s pupils are normally different sizes.
Doctors also examine the inside of the eye with an ophthalmoscope for signs that the pressure within the skull is increased.
If findings suggest that the pressure within the skull is increased, doctors do imaging tests immediately to check for swelling, bleeding, a structural abnormality that blocks the flow of cerebrospinal fluid, or a mass in the brain (such as a tumor, an accumulation of blood, or an abscess). If imaging test results indicate increased pressure, doctors may drill a small hole in the skull and insert a device into one of the fluid-filled spaces (ventricles) in the brain. This device is used to reduce the pressure and monitor it during treatment.
The person’s response to certain maneuvers can help doctors determine whether the brain stem is functioning normally:
Rotating the head and observing eye movements.
If the person is unconscious, gently flushing ice-cold water into one ear, then the other ear and observing eye movements (called caloric testing)
Caloric testing is done only if people are unconscious and doctors cannot check eye movements any other way. If people are conscious, flushing ice-cold water into their ear can cause severe vertigo, nausea, and vomiting.
Laboratory tests
These tests provide further clues about the possible cause of stupor or coma.
Blood levels of substances including sugar, electrolytes (such as sodium), alcohol, oxygen, minerals (such as magnesium), and carbon dioxide are measured. High levels of carbon dioxide may indicate that the person's breathing is impaired and that mechanical ventilation is required. Red and white blood cell counts are determined. Blood tests to check liver function and kidney function are done.
Urine is analyzed to determine whether any commonly used or suspected toxic substances are present. Samples of blood and urine may be sent to a laboratory to be cultured (to grow any microorganisms present) to check for infections.
Doctors measure the oxygen level in blood with a sensor placed on a finger (called pulse oximetry). They also measure levels of oxygen, carbon dioxide, and sometimes other gases in a sample of blood withdrawn from an artery (arterial blood gas tests). These tests are done to check for heart and lung disorders.
Other laboratory tests may be done, depending on which causes of coma doctors suspect.
Other tests
Electrocardiography (ECG) is done to check for heart disorders, which may reduce blood flow to the brain. Chest x-ray may be done to check for lung disorders, which may reduce the amount of oxygen in the blood.
If no cause has been quickly identified, computed tomography (CT) or magnetic resonance imaging (MRI) of the head is done to check for a mass, bleeding, swelling, or other structural brain damage.
If the cause is unclear after imaging tests or if meningitis or bleeding between the layers of tissue covering the brain (subarachnoid hemorrhage) is possible, a spinal tap (lumbar puncture) may be done to withdraw a sample of cerebrospinal fluid. The fluid is examined and analyzed to check for various causes. CT or MRI of the head is typically done before the spinal tap to determine whether pressure inside the skull (intracranial pressure) is increased—for example, by a tumor or bleeding within the brain (intracerebral hemorrhage). If pressure is increased, a spinal tap may be dangerous and should not be done. It could make the brain shift sideways and downward by rapidly reducing the pressure below the brain, and thus at least theoretically, cause or worsen brain herniation. However, herniation after a spinal tap is relatively uncommon. If intracranial pressure is increased, it is monitored continuously, and measures to decrease it are taken.
If doctors suspect the cause of impaired consciousness is seizures or if the cause is unclear after other tests are done, electroencephalography (EEG) may be done to check the brain’s electrical activity, which may be abnormal if the brain is not functioning normally. Occasionally, EEG indicates that the person is having seizures even though the limbs are not jerking (a disorder called nonconvulsive status epilepticus). Sometimes, when a person who has behavior or mental health problems appears unresponsive, EEG with video monitoring is done in the hospital. This test is done to determine whether brain function is normal. Results of the test can help doctors identify the problem and treat it appropriately.
Treatment of Stupor and Coma
Measures to help people breathe and to improve blood flow to the brain
Treatment of the cause
Immediate treatment
If a person is rapidly becoming less alert and more difficult to arouse, immediate treatment is required, often before a diagnosis is made. This rapid deterioration in consciousness is considered a medical emergency.
The first steps in treatment, sometimes done by emergency medical personnel, are to check
Whether the airway is open
Whether breathing is adequate
Whether pulse, blood pressure, and heart rate are normal (to make sure blood is reaching the brain)
If possible, any problems present are corrected.
People are treated first in an emergency department and then admitted to a hospital intensive care unit. In both places, nurses can monitor heart rate, blood pressure, temperature, and the oxygen level in the blood. Any abnormalities in these measurements are immediately corrected to prevent further damage to the brain. Oxygen is often given immediately, and a tube is inserted into a vein (an intravenous line) so that medications or sugar (glucose) can be given quickly.
If people have a very high or low body temperature, measures are taken to cool (heatstroke treatment) or warm them (hypothermia treatment). Any other disorders (such as heart or lung disorders), if present, are treated.
Blood pressure is closely monitored to make sure it is not too high or too low. High blood pressure can further impair consciousness and lead to other problems, such as stroke. Low blood pressure can impair consciousness because the brain does not get enough blood and oxygen.
Treatment of the cause
The cause of stupor or coma is treated when possible.
For a low blood sugar level, glucose (a sugar) is immediately given intravenously. Giving glucose often results in instant recovery if the coma is caused by a low blood sugar level. Thiamin is always given with glucose because if people are undernourished (usually because of alcohol abuse), glucose alone can trigger or worsen a brain disorder called Wernicke encephalopathy.
If a head injury is the cause, the neck must be immobilized until doctors can check for damage to the spine. Some people in a stupor or coma after a head injury benefit from treatment with medications that can help nerve cells function better, such as amantadine. Such treatment may help people regain some level of function more quickly. However, such treatment may not make any difference in improvement over the long term.is the cause, the neck must be immobilized until doctors can check for damage to the spine. Some people in a stupor or coma after a head injury benefit from treatment with medications that can help nerve cells function better, such as amantadine. Such treatment may help people regain some level of function more quickly. However, such treatment may not make any difference in improvement over the long term.
If opioid overdose is suspected, the antidote naloxone is given. Recovery may be almost immediate if the opioid is the only cause of impaired consciousness. If people take opioids, their doctor may prescribe a naloxone auto-injector for them. This device enables a family member or other caregiver to give them naloxone immediately if an opioid overdose is suspected.overdose is suspected, the antidote naloxone is given. Recovery may be almost immediate if the opioid is the only cause of impaired consciousness. If people take opioids, their doctor may prescribe a naloxone auto-injector for them. This device enables a family member or other caregiver to give them naloxone immediately if an opioid overdose is suspected.
Rarely, when a person may have ingested certain toxic substances, illicit drugs, or medications within about 1 hour, doctors may insert a large tube through the person's mouth and into the stomach so that the stomach can be pumped. Pumping the stomach is done to identify its contents and to prevent more of the substances from being absorbed. Activated charcoal may also be given through the tube or through a smaller tube inserted through the nose (nasogastric tube). The charcoal prevents the stomach from absorbing more of the substances.
Treatment to control breathing
People in a deep stupor or a coma may require a breathing tube and mechanical ventilation. Mechanical ventilation is especially important if breathing is too slow or shallow or otherwise impaired (for example, because the brain is damaged or malfunctions) or if the person has very low blood pressure, vomiting, or a seizure.
The breathing tube is inserted through the mouth and into the windpipe (trachea)—called endotracheal intubation. Oxygen is delivered directly into the lungs through the tube. The tube also prevents people from inhaling stomach contents after vomiting. Before inserting the tube, doctors may spray the person's throat with a numbing spray or give the person a medication to prevent the muscles from contracting involuntarily (a paralytic medication). The tube is then attached to a mechanical ventilator.
Mechanical ventilation can cause agitation, which can be treated with a sedative.
Treatment of increased pressure within the skull
If the pressure within the skull (intracranial pressure) is increased, the following measures may be taken to lower it:
The head of the bed may be elevated.
Mechanical ventilation may be used to help people breathe faster (called hyperventilation), particularly during the first half hour it is used. Breathing faster removes carbon dioxide from the lungs and reduces the level of carbon dioxide in the blood. As a result, blood vessels in the undamaged part of the brain narrow, and less blood reaches the brain. This measure quickly but temporarily lowers pressure within the skull (for about 30 minutes) and does not damage the brain further. Lowering the pressure for a time gives doctors time to start to treat the cause—for example, to do emergency brain surgery.
Diuretics or other medications may be used to reduce fluids in the brain and rest of the body. Diuretics help eliminate excess fluid by causing the kidneys to excrete more sodium and water into urine.
A sedative may be given to control excess involuntary muscle contractions or agitation caused by mechanical ventilation. These problems can increase pressure within the skull.
Blood pressure is lowered if it is very high.
Sometimes doctors insert a drain (shunt) into the ventricles of the brain to drain cerebrospinal fluid. Removing excess fluid can help lower pressure within the skull.
If pressure is increased because of a brain tumor or abscess, corticosteroids, such as dexamethasone, may help reduce pressure. However, corticosteroids are not used when increased pressure is caused by certain other disorders, such as intracerebral hemorrhage or a stroke, because corticosteroids may make these conditions worse.If pressure is increased because of a brain tumor or abscess, corticosteroids, such as dexamethasone, may help reduce pressure. However, corticosteroids are not used when increased pressure is caused by certain other disorders, such as intracerebral hemorrhage or a stroke, because corticosteroids may make these conditions worse.
If other measures do not work, the following may be tried:
When pressure within the skull is increased after a head injury or cardiac arrest, measures to lower body temperature may be tried. These measures may help some people who have had cardiac arrest. However, use of this measure is controversial.
Pentobarbital (a barbiturate) may be used to reduce blood flow to the brain and brain activity. This treatment may improve the prognosis for some people. However, it is not beneficial for everyone, and it has side effects, such as low blood pressure and abnormal heart rhythms.Pentobarbital (a barbiturate) may be used to reduce blood flow to the brain and brain activity. This treatment may improve the prognosis for some people. However, it is not beneficial for everyone, and it has side effects, such as low blood pressure and abnormal heart rhythms.
The skull may be opened surgically (craniectomy), creating more room for the swollen brain and thus reducing pressure on the brain. This treatment can prevent death, but it may not improve a person's ability to function.
Long-term care
People in a coma require comprehensive care. They are fed through a tube inserted through the nose and into the stomach (called tube feeding). Sometimes they are fed through a tube inserted directly into the stomach or small intestine through an incision in the abdomen. Medications may also be given through these tubes.
Many problems result from being unable to move (immobility), and measures to prevent them are essential (see Problems Due to Bed Rest). For example, the following can happen:
Pressures sores: Lying in one position can cut off the blood supply to some areas of the body, causing skin to break down and pressure sores to form.
Weak muscles: When muscles are not used, they waste away (atrophy) and become weak. People with muscle weakness may have trouble breathing on their own when they are taken off the ventilator.
Contractures: Lack of movement can also lead to permanent stiffening and shortening of muscles (contractures) causing joints to become permanently bent.
Blood clots: Lack of movement makes blood clots more likely to form in leg veins. The blood clots can break off, travel to the lungs, and block arteries there (called pulmonary embolism).
Damage to muscles and nerves in the arms and legs: Lack of movement or lying in one position for a long time can put pressure on a nerve that runs close to the surface of the body near a prominent bone, such as a nerve in an elbow, a shoulder, a wrist, or a knee. Such pressure can injure the nerve. As a result, the muscles that the nerve controls function less well.
Pressure sores can be prevented by frequently repositioning the person and placing protective padding under parts of the body that are in contact with the bed, such as the heels, to protect them.
To prevent contractures, physical therapists gently move the person’s joints in all directions (passive range-of-motion exercises) or splint joints in certain positions. Starting physical therapy early can help people who have not been able to move recover function.
Preventing blood clots includes use of medications and compression or elevation of the person's legs. Moving the limbs, as occurs in passive-range-of-motion exercises, may also help prevent blood clots.
Because people cannot blink, their eyes may become dry. Eye drops can help.
If people are incontinent, care should be taken to keep the skin clean and dry. If the bladder is not functioning and urine is being retained, a tube (catheter) may be placed in the bladder to drain urine. Catheters are carefully cleaned and regularly examined to prevent urinary tract infections from developing.
Prognosis for Stupor and Coma
In general, if people with impaired consciousness start to respond to sounds, touch, or other stimuli within 6 hours, they are more likely to recover. Recovery is also likely if one or more of the following occur within the first days:
Speech returns, even if it is incomprehensible.
The eyes can follow an object.
People can follow commands.
Muscle tone returns to normal.
The likelihood of recovery also depends on the cause and duration of impaired consciousness, as in the following:
Overdose of a sedative: Recovery is likely unless people stopped breathing long enough to cause brain damage.
A low blood sugar level: Complete recovery is possible if the brain was not deprived of sugar for more than about 1 hour.
Head injury: Substantial recovery may occur, even if the coma lasts several weeks (but not if it lasts more than 3 months).
Stroke: Permanent brain damage is likely if coma lasts 6 hours or longer.
Infection: Complete recovery is often possible if people are promptly treated.
Having another disorder (such as diabetes mellitus, high blood pressure, or a lung or heart disorder), if it is severe, may negatively affect recovery. Also, spending a long time in intensive care unit (ICU) can cause problems such as nerve damage, weak muscles, pulmonary embolism, pressures sores, and urinary tract infections.
After cardiac arrest, full recovery is rare if people have any of the following:
Certain disorders such as heart disorders, high blood pressure, or diabetes mellitus
Coma for more than 6 hours
Unintended (involuntary) muscle movements (usually muscle twitches)
Abnormal extension of the limbs (decerebrate rigidity) or no response to painful stimulation
Pupils that do not react to light after 1 to 3 days
Seizures that occur within 24 to 48 hours after cardiac arrest and that recur repeatedly
If people cannot move their limbs after cardiac arrest, recovery is difficult.
However, if doctors have used cooling to treat people after cardiac arrest, they usually wait an extra 3 days for these responses to occur. Cooling the body may preserve brain function after cardiac arrest, but it also tends to slow recovery of brain function.
Sometimes doctors use a test called somatosensory evoked responses to determine whether the brain stem or cerebral hemispheres can function. For this test, electrodes, which produce a mild electrical signal, are placed on parts of the body, and EEG is used to detect and record how long the electrical signal takes to reach the brain. Similarly, auditory evoked responses use clicking sounds in each ear to test if hearing signals reach the brain. If evoked response signals repeatedly do not reach the brain, the prognosis tends to be poor.
Children and sometimes young adults recover more fully than older adults because brain cells repair themselves more quickly and completely in the young.
For people who remain in a deep coma longer than a few weeks, decisions about continued use of a ventilator, feeding tube, and medications should be made. Family members should discuss these issues with the doctors. If people have advance medical directives, such as a living will or durable power of attorney for health care, the directives should guide decisions about continuing care.
Essentials for Older Adults: Coma and Stupor
Impaired consciousness, including lethargy, stupor, and coma, is a particular concern among older adults for the following reasons:
Age-related changes in the brain: As people age, the number of nerve cells in the brain decreases and blood flow to the brain decreases. Thus, medications and illicit drugs are more likely to impair consciousness and mental function in older adults because the older brain is slower and less able to compensate for a medication's or illicit drug's effects on the brain. Also, blood vessels in the brain become more fragile, increasing the risk of stroke.
Other age-related changes: Changes in other parts of the body also make older adults more sensitive to the effects of medications and illicit drugs. For example, as people age, the kidneys are less able to excrete medications into urine, and the liver is less able to break down (metabolize) many medications. Thus, medications are less readily removed from the body. More of the medication may remain in the blood and may remain there longer. More of the medication may then reach the brain and affect brain function. As a result, even a low dose of a medication can make older adults feel confused or drowsy. Often, older adults need a lower dose than is typically used.
Use of several medications: Many older adults take several medications (called polypharmacy) because they have one or more chronic disorders such as high blood pressure, diabetes, or arthritis. Taking several medications increases the risk of drug interactions with foods, nutritional supplements, and other substances, possibly negatively affecting the brain. For example, one medication may cause the level of another medication to increase.
A complex medication schedule: Also, if older adults have to take many medications, the schedule for taking them may be complex. As a result, they are more likely to make mistakes and may take too much or too little of a medication.
Effect of minor disorders: Relatively minor disorders, such as a urinary tract infection or dehydration, are more likely to impair consciousness in older adults than in younger people.
Presence of other disorders: Many disorders that are more common among older adults can impair consciousness. They include strokes, brain tumors, bulges in weakened arteries (aneurysms) in the brain, metabolic disorders, severe lung disorders, severe infections, and heart failure. Other disorders (such as diabetes) increase the risk of impaired consciousness if another problem (such as dehydration or an infection) develops.
Higher risk of falls and head injury: Older adults are at higher risk of head injury after a fall or a motor vehicle crash. Injury may occur when the brain is jarred or when tissues are torn, causing bleeding within the skull. Subdural hematomas (bleeding between the outer and middle layer of tissues that cover the brain) often result from such injuries. Older adults more often take aspirin or other medications that decrease the blood’s ability to clot (such as anticoagulants). These medications increase the risk of bleeding in or around the brain when a head injury occurs. Also, with aging, the brain shrinks, stretching the blood vessels between the layers. As a result, the blood vessels may tear and bleed.
Lifetime exposure to toxins: Over a lifetime, exposure to toxins in foods and the environment can damage brain cells and increase the risk of consciousness becoming impaired.
Difficulty recognizing impaired consciousness: Impaired consciousness may be harder to recognize in older adults. If older adults become less alert or less conscious of things around them, family members and friends may not notice or may assume that the change results from aging. (Impaired consciousness is not a normal part of aging.) Also, a change in consciousness may be harder to discern in older adults who have dementia or another brain disorder or who have had a stroke.
Ability to recover: Older adults are less likely to recover from stupor or coma because the brain becomes less able to repair itself as people age.
In older adults, consciousness is commonly impaired by reactions to medications, illicit drugs, dehydration, and infections.







