



Neuromyelitis optica spectrum disorder affects mainly the nerves in the eyes and spinal cord, causing patches of myelin (the substance that covers most nerve fibers) and the nerve fibers under them to be damaged or destroyed.
Topic Resources


Neuromyelitis optica spectrum disorder is a demyelinating disorder. It causes symptoms similar to those of multiple sclerosis (MS) and used to be considered a variant of multiple sclerosis. However, neuromyelitis optica spectrum disorder typically affects mainly the eyes and the spinal cord, and multiple sclerosis also affects the brain.

The risk of becoming disabled is greater with neuromyelitis optica spectrum disorder than with multiple sclerosis. Thus, people with symptoms suggesting neuromyelitis optica spectrum disorder should see a doctor promptly.
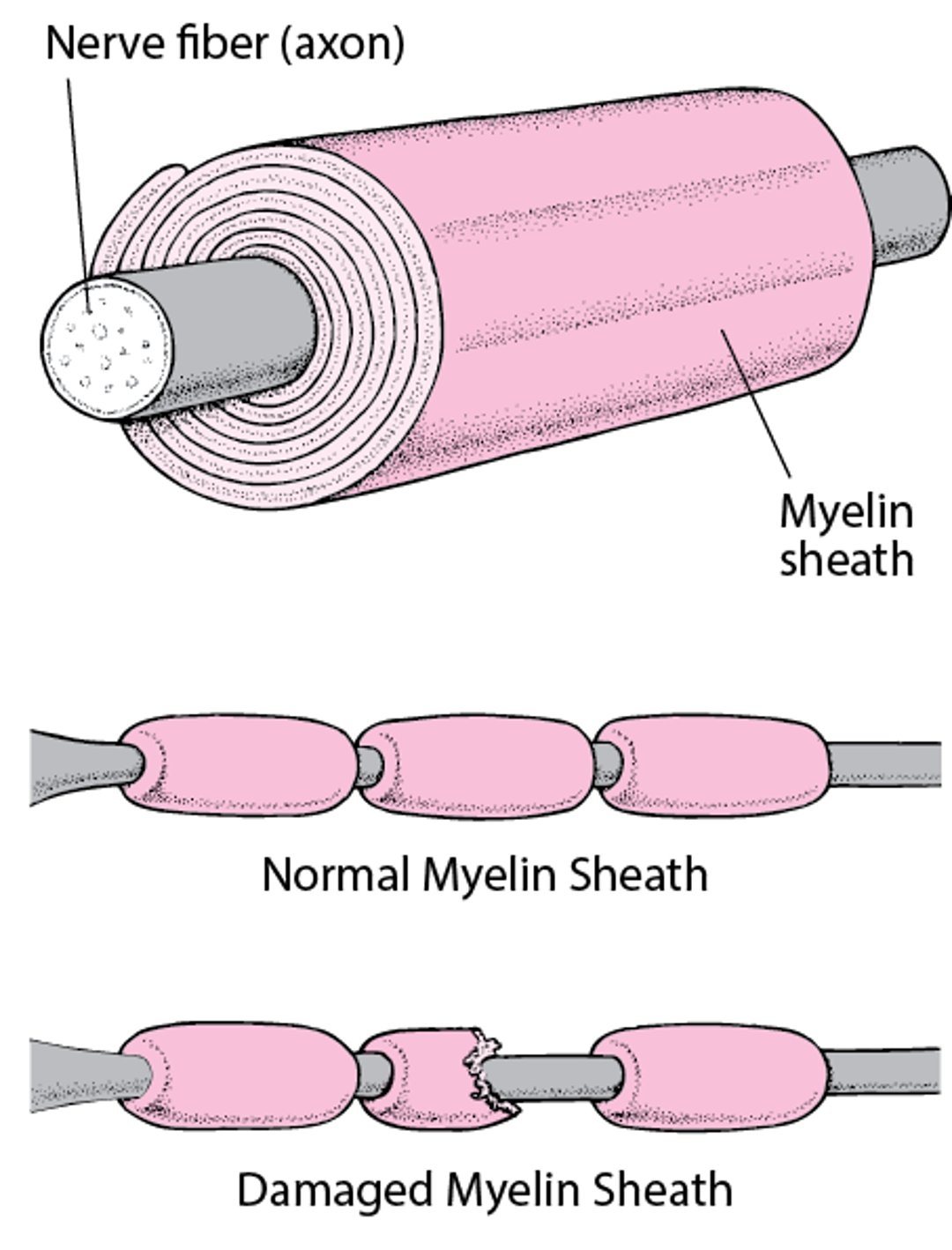
Insulating a Nerve Fiber
Most nerve fibers inside and outside the brain are wrapped with many layers of tissue composed of a fat (lipoprotein) called myelin. These layers form the myelin sheath. Much like the insulation around an electrical wire, the myelin sheath enables nerve signals (electrical impulses) to be conducted along the nerve fiber with speed and accuracy. When the myelin sheath is damaged (called demyelination), nerves do not conduct electrical impulses normally. |

Neuromyelitis optica spectrum disorder is also an autoimmune disorder. Autoimmune disorders occur when the immune system malfunctions and attacks the body’s own tissues. In neuromyelitis optica spectrum disorder, the target of the autoimmune attack is one of the following proteins:
A protein called aquaporin 4: This protein is present on the surface of support cells in the brain, spinal cord, and optic nerves. These support cells are called astrocytes.
Myelin oligodendrocyte glycoprotein: This protein is present in the cells that form a coating around nerve cell axons in the brain, spinal cord, and optic nerves. These cells are called oligodendrocytes. (Axons are nerve fibers that send messages.)
Damage to astrocytes or oligodendrocytes is thought to lead to demyelination. In some people with neuromyelitis optica spectrum disorder, the immune system targets another protein called myelin oligodendrocyte glycoprotein (MOG), which is present on the outer layer of myelin.
Symptoms of NMOSD
Neuromyelitis optica spectrum disorder causes inflammation of the optic nerve (optic neuritis). One or both eyes may be affected. The disorder causes episodes of eye pain and dim, blurred, or lost vision.
Days to weeks (sometimes years) later, the limbs are affected. People may temporarily lose sensation. They may have painful muscle spasms, and the arms and legs may become weak and sometimes paralyzed. People may be unable to control the bladder (urinary incontinence) and bowels (fecal incontinence).
Some people have hiccups that will not stop (persistent or intractable hiccups) or nausea and vomiting.
In some people, the part of the spinal cord that controls breathing is inflamed, leading to difficulty breathing, which is life threatening.
Neuromyelitis optica spectrum disorder progresses differently in each person. As the disorder progresses, people may have brief, frequent, painful muscle spasms. Eventually, blindness, loss of sensation and muscle weakness in the limbs, and bladder and bowel dysfunction may become permanent.
Diagnosis of NMOSD
A doctor's evaluation
Magnetic resonance imaging
Visual evoked responses
Blood tests
To diagnose neuromyelitis optica spectrum disorder, doctors evaluate the nervous system (neurologic examination) during a physical examination. The optic nerve is examined with an ophthalmoscope.
Usually, tests include magnetic resonance imaging (MRI) of the brain to rule out multiple sclerosis. MRI of the spinal cord and evoked responses are done to help confirm the diagnosis of neuromyelitis optica spectrum disorder.
When the visual evoked responses test is used to diagnose neuromyelitis optica spectrum disorder, stimuli for sight (such as a flashing light) are used to activate certain areas of the brain. Then, electroencephalography is used to detect the response to the stimuli. Based on these responses, doctors can tell how well the optic nerve is working.
Blood tests to detect specific antibodies to aquaporin 4 and to myelin oligodendrocyte glycoprotein may be done to distinguish neuromyelitis optica spectrum disorder from multiple sclerosis. (Antibodies are proteins produced by the immune system to help defend the body against a particular attacker.)
Treatment of NMOSD
Corticosteroids
Plasma exchange
Medications that suppress the immune system
There is no cure for neuromyelitis optica spectrum disorder. However, treatments can stop episodes, control symptoms, prevent episodes from recurring, and may help delay disability in the short term.
A corticosteroid (such as methylprednisolone) and a medication that suppresses the immune system (an immunosuppressant, such as azathioprine) are often used to stop and prevent episodes.A corticosteroid (such as methylprednisolone) and a medication that suppresses the immune system (an immunosuppressant, such as azathioprine) are often used to stop and prevent episodes.
Rituximab (a Rituximab (amonoclonal antibody used as an immunosuppressant) may be used to reduce the number of abnormal antibodies and to control the disorder.
Eculizumab (another monoclonal antibody) can sometimes help. This medication suppresses complement, which is a component of the immune system. Side effects of this medication include life-threatening Eculizumab (another monoclonal antibody) can sometimes help. This medication suppresses complement, which is a component of the immune system. Side effects of this medication include life-threateningmeningococcal meningitis, pneumonia, upper respiratory infections, and headache. Doctors usually give people who take eculizumab the , pneumonia, upper respiratory infections, and headache. Doctors usually give people who take eculizumab themeningococcal vaccine and closely monitor them.
Satralizumab and inebilizumab (both monoclonal antibodies) can be used to treat neuromyelitis optica spectrum disorder when aquaporin-4 antibodies are present. People taking these medications are closely monitored for infections, such as urinary tract and respiratory infections.Satralizumab and inebilizumab (both monoclonal antibodies) can be used to treat neuromyelitis optica spectrum disorder when aquaporin-4 antibodies are present. People taking these medications are closely monitored for infections, such as urinary tract and respiratory infections.
Plasma exchange may help people who do not respond to corticosteroids. For this treatment, blood is removed, then abnormal antibodies are removed, and the blood is returned to the person.
Treatment of symptoms is similar to that for multiple sclerosis. Baclofen or tizanidine may relieve muscle spasms.is similar to that for multiple sclerosis. Baclofen or tizanidine may relieve muscle spasms.







