



A stroke occurs when an artery to the brain becomes blocked or ruptures, resulting in death of an area of brain tissue due to loss of its blood supply (cerebral infarction). Symptoms occur suddenly.







Most strokes are ischemic (usually due to blockage of an artery), but some are hemorrhagic (due to rupture of an artery).
Transient ischemic attacks resemble ischemic strokes except that no permanent brain damage occurs and the symptoms typically resolve within 1 hour.
Symptoms occur suddenly and can include muscle weakness, paralysis, abnormal or lost sensation on one side of the body, difficulty speaking, confusion, problems with vision, dizziness, loss of balance and coordination, and, in some hemorrhagic strokes, a sudden, severe headache.
Diagnosis is based mainly on symptoms, but imaging and blood tests are also done.
Treatment of ischemic stroke may include medications to make blood less likely to clot or to break up clots and sometimes various procedures to treat blocked or narrowed arteries (such as angioplasty) or surgery to remove a clot (thrombectomy).
Treatment of hemorrhagic stroke may include medications and procedures to control blood pressure and relieve pressure around the brain and surgery to correct the source of bleeding.
Recovery after a stroke depends on many factors, such as the location and amount of brain damage, the person’s age, and the presence of other disorders.
Controlling high blood pressure, high cholesterol levels, and high blood sugar levels and not smoking help prevent strokes.
A stroke is called a cerebrovascular disorder because it affects the brain (cerebro-) and the blood vessels (vascular) that supply blood to the brain.
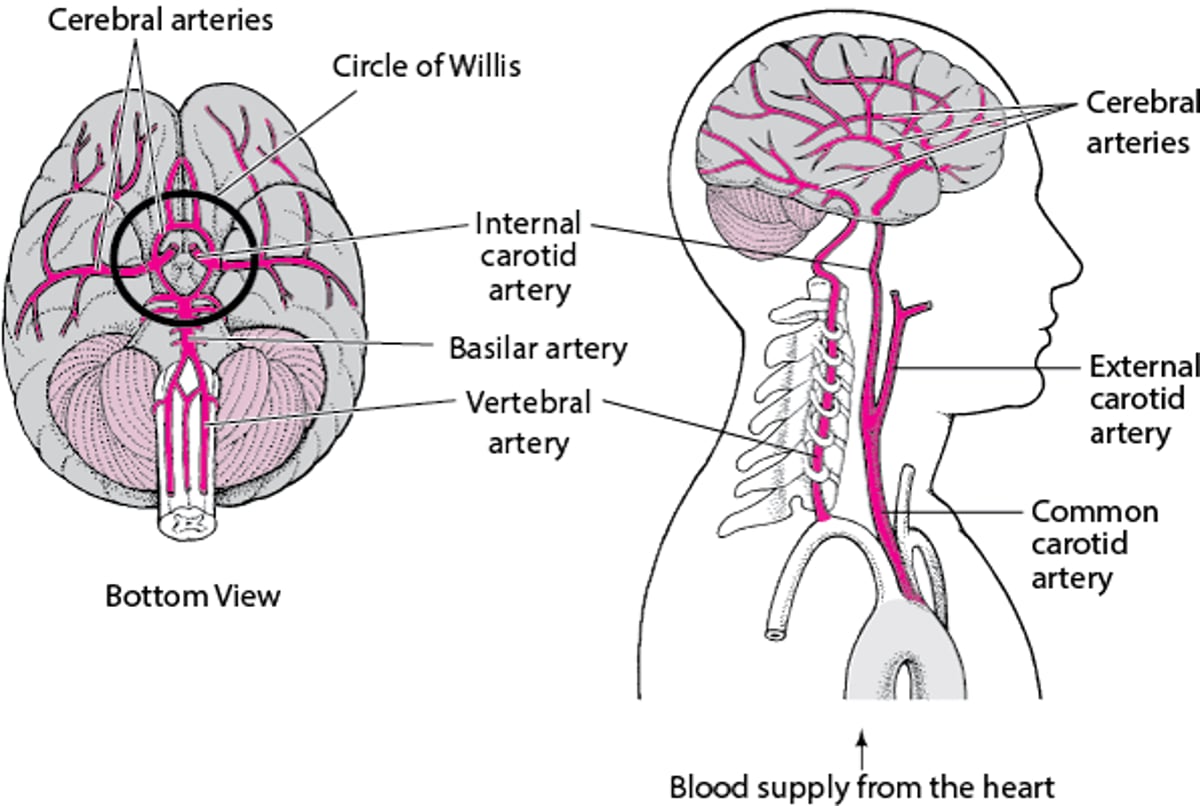
Supplying the Brain With Blood
Blood is supplied to the brain through two pairs of large arteries:
In the skull, the vertebral arteries unite to form the basilar artery (at the back of the head). The internal carotid arteries and the basilar artery divide into several branches, including the cerebral arteries. Some branches join to form a circle of arteries (circle of Willis) that connect the vertebral and internal carotid arteries. Other arteries branch off from the circle of Willis like roads from a traffic circle. The branches carry blood to all parts of the brain. When the large arteries that supply the brain are blocked, some people have no symptoms or have only a small stroke. But others with the same sort of blockage have a massive ischemic stroke. Why? Part of the explanation is collateral arteries. Collateral arteries run between other arteries, providing extra connections. These arteries include the circle of Willis and connections between the arteries that branch off from the circle. Some people are born with large collateral arteries, which can protect them from strokes. Then when one artery is blocked, blood flow continues through a collateral artery, sometimes preventing a stroke. Other people are born with small collateral arteries. Small collateral arteries may be unable to pass enough blood to the affected area, so a stroke results. The body can also protect itself against strokes by growing new arteries. When blockages develop slowly and gradually (as occurs in atherosclerosis), new arteries may grow in time to keep the affected area of the brain supplied with blood and thus prevent a stroke. If a stroke has already occurred, growing new arteries can help prevent a second stroke (but cannot reverse damage that has been done). |

Worldwide, stroke is the second most common cause of death. In the United States, strokes are the fifth most common cause of death and the most common cause of disabling nervous system damage in adults. In the United States, about 795,000 people have a stroke, and about 130,000 die of stroke each year.
Strokes are much more common among older people than among younger adults, usually because the disorders that lead to strokes progress over time. Over two thirds of all strokes occur in people older than 65. Stroke is more common among women than among men, and nearly 60% of deaths due to stroke occur in women, possibly because women are on average older when the stroke occurs.

Black people, Hispanic people, American Indians, and Alaska Natives are more likely than non-Hispanic White people or Asian people to have a stroke. The risk of having a first stroke is nearly twice as high for Black people as for White people. Black people are also more likely to die of a stroke than White people.
Types
There are two types of strokes:
About 80% of strokes are ischemic—usually due to a blocked artery, often blocked by a blood clot. Brain cells, thus deprived of their blood supply, do not receive enough oxygen and glucose (a sugar), which are carried by blood. The damage that results depends on how long brain cells are deprived of blood. If they are deprived for only a brief time, brain cells are stressed, but they may recover. If brain cells are deprived longer, brain cells die, and some functions may be lost, sometimes permanently. How soon brain cells die after being deprived of blood varies. They die after only a few minutes in some areas of the brain but not until after 30 minutes or more in other areas. In some cases, after brain cells die, a different area of the brain can learn how to do the functions previously done by the damaged area.
Transient ischemic attacks (TIAs), sometimes called ministrokes, are often an early warning sign of an impending ischemic stroke. They are caused by a brief interruption of the blood supply to part of the brain. Because the blood supply is restored quickly, brain tissue does not die, as it does in a stroke, and brain function quickly returns.
The other 20% of strokes are hemorrhagic—due to bleeding in or around the brain. In this type of stroke, a blood vessel ruptures, interfering with normal blood flow and allowing blood to leak into brain tissue or around the brain. Blood that comes into direct contact with brain tissue irritates the tissue and, over time, can cause scar tissue to form in the brain, sometimes leading to seizures.
Risk factors for stroke
Some risk factors for stroke can be controlled or modified to some extent—for example, by treating the disorder that increases risk of stroke.
The major modifiable risk factors for both types of stroke are
Insulin resistance (an inadequate response to insulin), which occurs in type 2 diabetes
Cigarette smoking
Obesity, particularly if the excess weight is around the abdomen
Consumption of too much alcohol
Lack of physical activity
An unhealthy diet (such as one that is high in saturated fats, trans fats, and calories)
Depression or other mental stresses
Heart disorders that increase the risk of blood clots forming in the heart, breaking off, and traveling through the blood vessels as emboli (such as a heart attack or an abnormal heart rhythm called atrial fibrillation)
Infective endocarditis (infection of the heart's lining and usually of the heart valves)
Use of cocainecocaine or amphetamines
Inflammation of blood vessels (vasculitis)
Many of these factors are also risk factors for atherosclerosis, which is a common cause of ischemic stroke. In atherosclerosis, arteries are narrowed or blocked by patchy fatty deposits that form in the walls of arteries.
Clotting disorders that result in excessive clotting are a risk factor for ischemic strokes. Disorders that increase bleeding increase the risk of hemorrhagic stoke.
High blood pressure is a particularly important risk factor for ischemic and hemorrhagic stroke.
For ischemic stroke, major modifiable risk factors also include
Narrowing (stenosis) of a carotid artery in the neck
For hemorrhagic stroke, major modifiable risk factors also include
Use of anticoagulants (medications that inhibit blood clotting)
A bulge in arteries of the brain (cerebral aneurysm)
An abnormal connections between arteries and veins (arteriovenous malformation)
The incidence of strokes has declined in recent decades, mainly because people are more aware of the importance of controlling high blood pressure and high cholesterol levels and stopping cigarette smoking. Controlling these factors reduces the risk of atherosclerosis.
Risk factors that cannot be modified include
Having had a stroke previously
Being older
Having relatives who have had a stroke (genetic factors)
Symptoms of Stroke
Symptoms of a stroke or transient ischemic attack occur suddenly. They vary depending on the precise location of the blockage or bleeding in the brain. Each area of the brain is supplied by specific arteries. For example, if an artery supplying the area of the brain that controls the left leg’s muscle movements is blocked, the leg becomes weak or paralyzed. If the area of the brain that senses touch in the right arm is damaged, sensation in the right arm is lost.
When Specific Areas of the Brain Are Damaged
Different areas of the brain control specific functions. Consequently, where the brain is damaged determines which function is lost. |

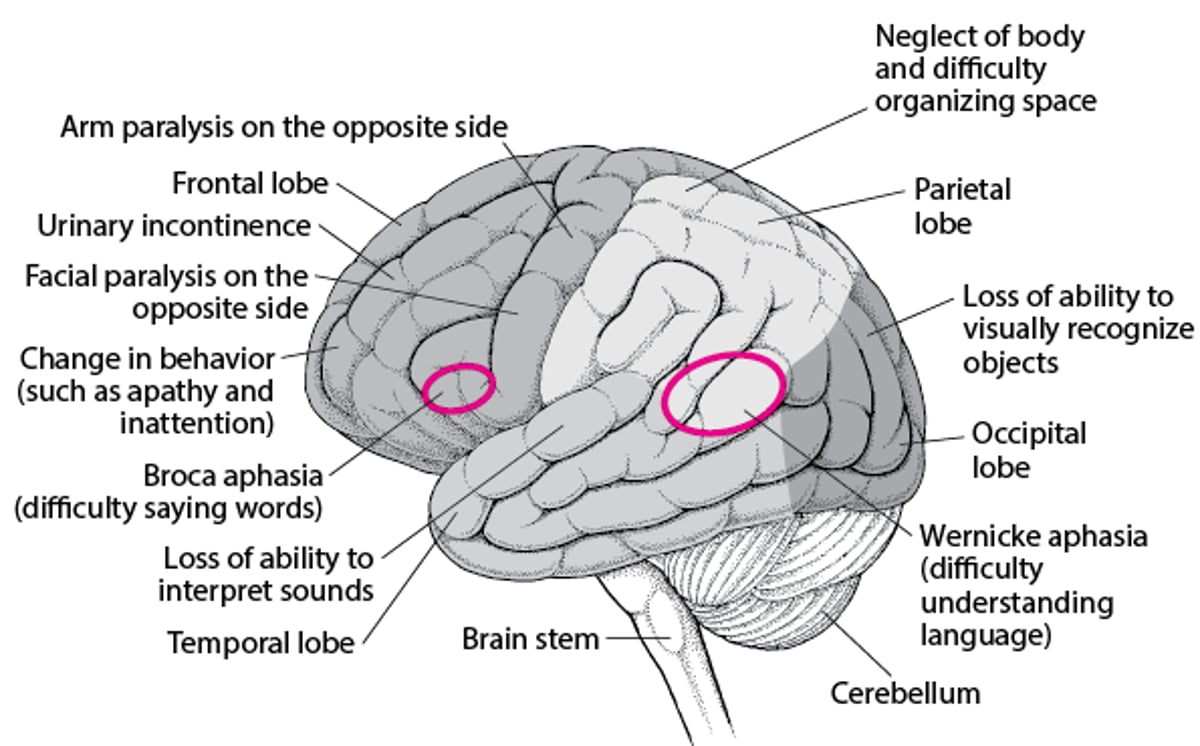
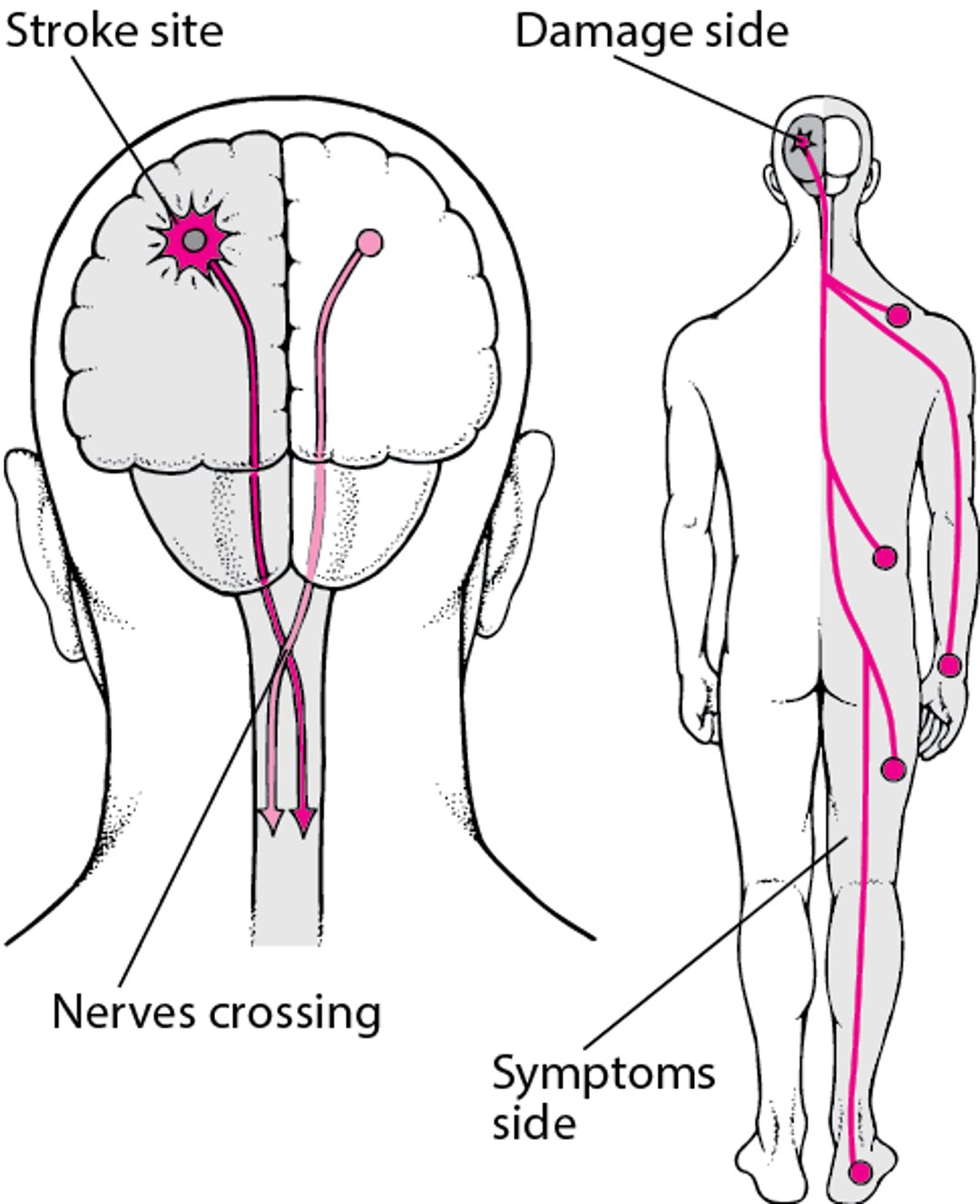
Strokes usually damage only one side of the brain. Because most of the nerves in the brain cross over to the other side of the body, symptoms appear on the side of the body opposite the damaged side of the brain. However, if the stroke damages the brain stem and affects some of the cranial nerves, some symptoms can also appear on the same side as the damaged side of the brain stem. Strokes that damage the brain stem can also affect both sides of the body. (The brain stem connects the cerebrum, which is the largest part of the brain, with the spinal cord. Cranial nerves directly connect the brain and the brain stem with the eyes, ears, nose, and throat and with various parts of the head, neck, and trunk.)
Why Strokes Usually Affect Only One Side of the Body
Strokes usually damage only one side of the brain. Because most nerves in the brain cross over to the other side of the body, symptoms appear on the side of the body opposite the damaged side of the brain. |

Warning symptoms of stroke
Because early treatment of stroke can help limit loss of function and sensation, everyone should know what the early symptoms of stroke are.
People who have any of the following symptoms should see a doctor immediately, even if the symptom goes away quickly:
Sudden weakness or paralysis on one side of the body (for example, half of the face, one arm or leg, or all of one side)
Sudden loss of sensation or abnormal sensations on one side of the body
Sudden difficulty speaking, including difficulty coming up with words and sometimes slurred speech
Sudden confusion, with difficulty understanding speech
Sudden dimness, blurring, or loss of vision, particularly in one eye, and double vision
Sudden dizziness or loss of balance and coordination, leading to falls
One or more of these symptoms are typically present in both hemorrhagic and ischemic strokes. Symptoms of a transient ischemic attack are the same, but they usually disappear within minutes and rarely last more than 1 hour.
Symptoms of a hemorrhagic stroke may also include the following:
Sudden severe headache
Nausea and vomiting
Temporary or persistent loss of consciousness
Very high blood pressure
Other symptoms
Other symptoms that may occur early include problems with memory, thinking, attention, or learning. People may be unable to recognize parts of the body and may be unaware of the stroke’s effects. The peripheral field of vision may be reduced, and hearing may be partially lost. Difficulty swallowing, dizziness, and vertigo may develop.
People may have difficulty controlling their bowels and/or bladder beginning several days or more after the stroke occurred. Loss of control may be permanent.
Later symptoms may also include involuntary stiffening and spasms of the muscles (spasticity) and inability to control emotions. Many people become depressed because of the stroke.
Effects of stroke
In most people who have had an ischemic stroke, loss of function is usually greatest immediately after the stroke occurs. However, in about 15 to 20%, the stroke is progressive, causing greatest loss of function after a day or two. This type of stroke is called an evolving stroke. In people who have had a hemorrhagic stroke, function usually is lost progressively over minutes to hours.
Over days to months, some function is usually regained because even though some brain cells die, others are only stressed and may recover. Also, certain areas of the brain can sometimes switch to the functions previously done by the damaged part—a characteristic called plasticity. However, the early effects of a stroke, including paralysis, can become permanent. Muscles that are not used usually become permanently spastic and stiff, and painful muscle spasms may occur. Walking, swallowing, pronouncing words clearly, and doing daily activities may remain difficult. Various problems with memory, thinking, attention, learning, or controlling emotions may persist. Depression, impairments in hearing or vision, or vertigo may be continuing problems.
Complications of stroke
When a stroke is severe, the brain swells, increasing pressure within the skull. Hemorrhagic strokes involve bleeding in the brain or in the tissues that cover it. This blood can increase pressure within the skull. Increased pressure can damage the brain directly or indirectly by forcing the brain sideways and downward in the skull. The brain may be forced through the rigid structures that separate the brain into compartments, resulting in a dangerous problem called herniation. The pressure affects areas that control consciousness and breathing in the brain stem (which connects the cerebrum with the spinal cord). Herniation can cause loss of consciousness, coma, irregular breathing, and death.
The symptoms caused by a stroke can lead to other problems.
If swallowing is difficult, people may inhale food, fluids, or saliva from the mouth into the lungs. Such inhalation (called aspiration) can cause aspiration pneumonia, which may be serious. Difficulty swallowing can also interfere with eating, resulting in undernutrition and dehydration.
People may have difficulty breathing.
Over time, not being able to move can result in pressure sores, muscle loss, permanent shortening of muscles (contractures), and the formation of blood clots in deep veins of the legs and pelvis (deep vein thrombosis). Clots can break off, travel through the bloodstream and block an artery to a lung (pulmonary embolism).
If bladder control is impaired, urinary tract infections are more likely to develop.
Diagnosis of Stroke
A doctor's evaluation
Computed tomography or magnetic resonance imaging
Laboratory tests including those to measure blood sugar
Symptoms and results of physical examination suggest the diagnosis of stroke, but tests are needed to help doctors determine the following:
Whether stroke has occurred
Whether it is ischemic or hemorrhagic
How severe it is and whether immediate treatment is required
What the best way to prevent future strokes is
Whether rehabilitation therapy is needed and, if so, what it should include
The blood sugar level is measured immediately because a low blood sugar level (hypoglycemia) occasionally causes symptoms similar to those of stroke, such as paralysis on one side of the body.
Computed tomography (CT) or magnetic resonance imaging (MRI) of the brain is used to do the following:
Determine whether a stroke has occurred and estimate how long ago it occurred
Determine whether the stroke is ischemic or hemorrhagic
Identify any large arteries that are blocked with a clot that could be removed mechanically—called endovascular (mechanical) thrombectomy
Check for signs of increased pressure within the skull (intracranial pressure)
These tests can detect most hemorrhagic strokes, except for some subarachnoid hemorrhages. When CT does not detect a stroke, a spinal tap may be done to check for blood due to a subarachnoid hemorrhage. CT and MRI can also detect many ischemic strokes but sometimes not until several hours after symptoms appear.
Other imaging tests include magnetic resonance angiography, CT angiography, and cerebral angiography. Cerebral angiography is done with a thin, flexible tube (catheter) inserted into an artery in the groin, threaded through the aorta to the carotid artery in the neck and into the skull. Contrast dye is injected into the arteries of the brain to make them visible on x-rays. However, CT angiography has largely replaced cerebral angiography because it is less invasive. CT angiography involves injection of a contrast agent into a vein in the arm—a slightly safer option than insertion of a catheter into an artery, as is done in cerebral angiography.
If needed to confirm the diagnosis, a specialized type of MRI, called diffusion-weighted MRI, can show areas of brain tissue that are severely and usually permanently damaged and no longer functioning. Diffusion-weighted MRI can often help doctors differentiate a transient ischemic attack from an ischemic stroke. However, this procedure is not always available.
To identify the cause of stroke, doctors try to determine where the problem is:
The heart: Electrocardiography (ECG), echocardiography, and blood tests are done to check for heart damage that could cause clots to form and then travel to the brain.
Blood vessels: CT, MRI, and ultrasonography are done to check the blood vessels from the heart to the brain.
The blood: Blood tests are done to check for disorders that cause blood clotting.
Doctors also do tests to check for problems that can contribute to or cause a stroke, such as a heart infection, a low blood oxygen level, and dehydration. Doctors check the urine for cocaine.
Additional tests are done as needed. The ability to swallow is evaluated as soon as a stroke is suspected, sometimes by taking x-rays after a substance that can be seen on x-rays (radiopaque contrast agent), such as barium, is swallowed. If people have difficulty swallowing, they are given nothing by mouth, except sometimes medications, until their swallowing improves.
Depending on the type of stroke doctors suspect, more tests are done to identify the cause.
Doctors often use a standardized set of questions and commands to determine how severe the stroke is and how well people are recovering. It includes evaluation of level of consciousness, the ability to answer questions, the ability to obey simple commands, vision, arm and leg function, and speech.
Treatment of Stroke
If needed, measures to support vital functions such as breathing
Various medications to break up clots or to make blood less likely to clot
Various procedures to treat blocked or narrowed arteries, surgery to remove a clot, or insertion of a coil to block an aneurysm
Rehabilitation to regain as much normal function as possible
Treatment of problems after a stroke
Anyone with symptoms of a stroke should seek medical attention immediately. The earlier the treatment, the better the chances for recovery. Thus, emergency medical services and hospitals are continuously developing new and better ways to treat people who have had a stroke as soon as possible after symptoms begin.
Doctors check the person’s vital functions, such as heart rate, breathing, temperature, and blood pressure, to make sure they are adequate. If they are not, measures to correct them are taken immediately. For example, if people are in a coma or unresponsive (as may result from brain herniation), mechanical ventilation (with a breathing tube inserted through the mouth or nose) may be needed to help them breathe. If symptoms suggest that pressure within the skull is high, medications may be given to reduce swelling in the brain, and a monitor may be put in the brain to periodically measure the pressure.
Other treatments used during the first hours and first days depend on the type of stroke.
Treatment of ischemic strokes may include the following:
Medications (such as antiplatelet medications, anticoagulants, medications to break up clots, and medications to control high blood pressure)
Insertion of a thin, flexible tube (catheter) into an artery, usually in the groin, and then through the aorta to an artery in the neck, followed by injection of a medication through the catheter to dissolve a clot (intra-arterial thrombolysis)
Use of instruments threaded through the catheter (called endovascular procedures) to remove a clot (mechanical thrombectomy), to widen a narrowed artery (angioplasty), and/or to place a stent to widen a narrowed artery
Surgery (endarterectomy) to remove fatty deposits blocking blood flow in an artery in the neck
Treatment of hemorrhagic stroke may include the following:
If needed, treatments that help blood clot (such as vitamin K and transfusions of fresh frozen plasma or platelets)
If blood pressure is very high, medications to control it
Occasionally, surgery to remove large areas of accumulated blood or to place a shunt to relieve the increased pressure within the skull
Insertion of small coils or stents through a catheter to the affected area to treat a ruptured brain aneurysm (the most common cause of a subarachnoid hemorrhage—a type of hemorrhagic stroke)
Later and ongoing treatments focus on
Preventing subsequent strokes
Treating and preventing problems that strokes can cause
Helping people regain as much function as possible (rehabilitation)
Preventing and Treating Problems After a Stroke
Problem | Measures |
|---|---|
To prevent blood clots, doctors may give anticoagulants, such as heparin or low molecular weight heparin, put elastic or air-filled support stockings on the person’s legs to improve blood circulation, or both.To prevent blood clots, doctors may give anticoagulants, such as heparin or low molecular weight heparin, put elastic or air-filled support stockings on the person’s legs to improve blood circulation, or both. Moving the legs, which improves blood flow, can also help. People, if able, are encouraged to walk or simply move their legs (for example, extending and flexing their ankles). If people cannot move their legs, a therapist or other staff member moves their legs for them (called passive exercise). | |
Nurses, other staff members, or caregivers should frequently turn or reposition people who are confined to a bed or wheelchair. Areas likely to develop pressure sores should be inspected every day. | |
Permanent shortening of muscles that limits movement (contractures) | Moving the limbs can prevent contractures. People, if able, are encouraged to move and change positions regularly. Or a therapist or other staff member moves their limbs for them and makes sure the limbs are placed in appropriate resting positions. Sometimes splints are used to prevent the limbs' muscles from shortening. |
People are evaluated for difficulty swallowing. If they have difficulty, care is taken to provide them with enough fluids and nourishment. Sometimes learning simple techniques (for example, how to position the head or how to breathe when swallowing) can help the person swallow safely. Tube feeding may be necessary until the ability to swallow returns. The feeding tube may be inserted directly into the stomach through a small incision in the abdomen. | |
If people smoke, they are encouraged to stop. Therapists also teach them to do deep breathing exercises and to cough to clear the airways. Therapists may provide a handheld breathing device. If needed, oxygen is provided through a face mask or a tube inserted in the nose or in the mouth. | |
Health care professionals regularly check for signs of urinary problems. If possible, a urinary catheter, which can cause urinary infections, is not used. If a catheter is needed, it is removed as soon as possible. | |
Discouragement and depression | Doctors discuss the effects of the stroke with affected people and their family members or other caregivers. The discussion includes the type of recovery that can be expected and ways to cope with limitations of function. People and their caregivers are put in contact with stroke support groups. Formal counseling or medications may be necessary to treat depression. |
Rehabilitation
Intensive rehabilitation after a stroke can help many people overcome disabilities. The exercises and training of rehabilitation encourage unaffected areas of the brain to learn to perform functions that were done by the damaged area. Also, people are taught new ways to use muscles unaffected by the stroke to compensate for losses in function.
The goals of rehabilitation are the following:
To regain as much normal function in doing daily activities as possible
To maintain and improve physical condition and to improve walking
To help people relearn old skills and learn new ones as needed
Success depends on the area of the brain damaged and the person’s general physical condition, functional and cognitive abilities before the stroke, social situation, learning ability, and attitude. Patience and perseverance are crucial. Participating actively in the rehabilitation program can help people avoid or lessen depression.
Rehabilitation is started in the hospital as soon as people are physically able—usually within 1 or 2 days of admission. Moving the affected limbs is an important part of rehabilitation. Regularly moving the limbs helps prevent muscles from shortening and becoming tight (called spasticity). It also helps maintain muscle tone and strength. If people cannot move their muscles themselves, a therapist moves their limbs for them. People are encouraged to practice other activities, such as moving in bed, turning, changing position, and sitting up.
Some problems due to stroke require specific therapies—for example, to help with walking (gait or ambulation training), to improve coordination and balance, to reduce spasticity (involuntary tightening of muscles), or to compensate for vision or speech problems.
After discharge from the hospital, rehabilitation can be continued on an outpatient basis, in a nursing home, in a rehabilitation center, or at home. Occupational and physical therapists can suggest ways to make life easier and the home safer for people with disabilities.
Family members and friends can contribute to a person’s rehabilitation by keeping in mind what effects a stroke can have, so that they can better understand and support the person. Support groups can provide emotional encouragement and practical advice for people who have had a stroke and for those who care for them.
Prognosis for Stroke
The sooner a stroke is treated, the less severe brain damage is likely to be and the better the chances for recovery.
Certain factors suggest that the outcome of a stroke is likely to be poor. Strokes that impair consciousness or that affect a large part of the left side of the brain (which is responsible for language) may be particularly grave.
Usually, the more quickly people improve during the days after stroke, the more they will ultimately improve. Improvement commonly continues for 6 months after the stroke. In adults who have had an ischemic stroke, problems that remain after 12 months are likely to be permanent, but children continue to improve slowly for many months. Older people fare less well than younger people. For people who already have other serious disorders (such as dementia), recovery is more limited.
If a hemorrhagic stroke is not massive and pressure within the brain is not very high, the outcome is likely to be better than that after an ischemic stroke with similar symptoms. Blood (in a hemorrhagic stroke) does not damage brain tissue as much as an inadequate supply of oxygen (in an ischemic stroke) does.
Depression often occurs after a stroke and may interfere with recovery. However, depression can be treated. So if a person who has had a stroke is feeling unusually sad or has lost interest or pleasure in doing formerly enjoyable activities, the person should tell the doctor. The doctor may also ask family members whether they have noticed any signs of depression in the person. Then the doctor can determine whether depression is present and, if so, treat it.
End-of-Life Issues
For some people who have had a stroke, function is predicted to remain very limited despite treatment. For such people, quality of their life may be perceived to be poor. Their care may focus on control of pain, comfort measures, and provision of fluids and nourishment.
People who have had a stroke should establish advance directives as soon as possible because the recurrence and progression of strokes are unpredictable. Advance directives can help a doctor determine what kind of medical care people want if they become unable to make these decisions.
Prevention of Stroke
Preventing strokes is preferable to treating them. The main strategy for preventing a first stroke is managing the major risk factors. If people have had a stroke, additional preventive measures are usually needed.
Managing risk factors
High blood pressure and diabetes should be controlled. Cholesterol levels should be measured and, if high, medications to lower cholesterol levels (lipid-lowering medications) are used to reduce the risk of atherosclerosis. Other conditions that increase the risk of stroke, including atrial fibrillation and carotid artery stenosis, should be treated, if present.
Smoking and use of amphetamines or cocaine should be stopped, and alcohol should be limited to no more than two drinks a day. Exercising regularly and, if overweight, losing weight help people control high blood pressure, diabetes, and high cholesterol levels.
Having regular checkups enables a doctor to identify risk factors for stroke so that they can be managed promptly.
Antiplatelet medications
If people have had an ischemic stroke, taking an antiplatelet medication can reduce the risk of another ischemic stroke. Antiplatelet medications make platelets less likely to clump and form clots, a common cause of ischemic stroke. (Platelets are tiny cell-like particles in blood that normally help it clot in response to damaged blood vessels.)
Aspirin, one of the most effective antiplatelet medications, is usually prescribed. One adult’s tablet or 1 children’s tablet (which is about one fourth the dose of an adult Aspirin, one of the most effective antiplatelet medications, is usually prescribed. One adult’s tablet or 1 children’s tablet (which is about one fourth the dose of an adultaspirin) is taken each day. Either dose seems to prevent strokes about equally well. If people have had a TIA or minor stroke, taking a combination of a low dose of aspirin and clopidogrel (an antiplatelet medication) for a short time (about 3 weeks) is slightly more effective at reducing the risk of future strokes than taking ) is taken each day. Either dose seems to prevent strokes about equally well. If people have had a TIA or minor stroke, taking a combination of a low dose of aspirin and clopidogrel (an antiplatelet medication) for a short time (about 3 weeks) is slightly more effective at reducing the risk of future strokes than takingaspirin alone. However, risk is reduced only for the first 3 months after a stroke. After that, the combination has no advantage over aspirin alone. Also, taking clopidogrel plus aspirin for more than 3 months increases the risk of bleeding by a small amount.
Clopidogrel alone may be given to people who cannot tolerate aspirin.Clopidogrel alone may be given to people who cannot tolerate aspirin.
Some people are allergic to antiplatelet medications or similar medications and cannot take them. Also, people who have gastrointestinal bleeding should not take antiplatelet medications.
Anticoagulants
If an ischemic stroke or a transient ischemic attack is due to blood clots originating in the heart, warfarin (also called coumadin), an anticoagulant, may be given to inhibit blood clotting. Because taking warfarin and an antiplatelet medication increases the risk of bleeding, these medications are only occasionally used together for stroke prevention.If an ischemic stroke or a transient ischemic attack is due to blood clots originating in the heart, warfarin (also called coumadin), an anticoagulant, may be given to inhibit blood clotting. Because taking warfarin and an antiplatelet medication increases the risk of bleeding, these medications are only occasionally used together for stroke prevention.
Dabigatran, apixaban, and rivaroxaban are newer anticoagulants that are often used instead of Dabigatran, apixaban, and rivaroxaban are newer anticoagulants that are often used instead ofwarfarin.
Spotlight on Aging: Strokes
After a stroke, older people are more likely to have problems, such as pressure sores, pneumonia, permanent shortening of muscles that limits movement (contractures), and depression. Older people are also more likely to already have disorders that limit treatment of stroke. For example, they may have very high blood pressure or gastrointestinal bleeding that prevents them from taking anticoagulants to reduce the risk of blood clots. Some treatments, such as endarterectomy (surgical removal of fatty deposits in arteries), are more likely to cause complications in older people. Nonetheless, treatment decisions should be based on the person’s health rather than on age itself. Some disorders common among older people can interfere with their recovery after a stroke, as in the following:
A good recovery is more likely when older people have the following:
Because recovery after stroke depends on so many medical, social, financial, and lifestyle factors, rehabilitation and care for older people should be individually designed and managed by a team of health care professionals (including nurses, psychologists, and social workers as well as a doctor or therapist). Team members can also provide information about resources and strategies to help people who have had a stroke and their caregivers with daily living. |







