


Appendicitis is inflammation and infection of the appendix (a thin tube of tissue that is connected to the intestines).
Appendicitis seems to develop when the appendix becomes blocked either by hard fecal material (called a fecalith) or swollen lymph nodes in the intestine that can occur with various infections.
Pain typically starts around the bellybutton (umbilicus) and then moves to the right lower abdomen but may be felt throughout the abdomen.
Children may have nausea and vomiting and be irritable or listless.
Diagnosis is challenging and requires a physical examination, blood tests, and usually an imaging study (such as ultrasonography, computed tomography, or magnetic resonance imaging) or laparoscopy.
An inflamed appendix is usually removed surgically, and if an infected appendix bursts (ruptures), antibiotics and more extensive surgery are needed.
(For adults, see Appendicitis.)

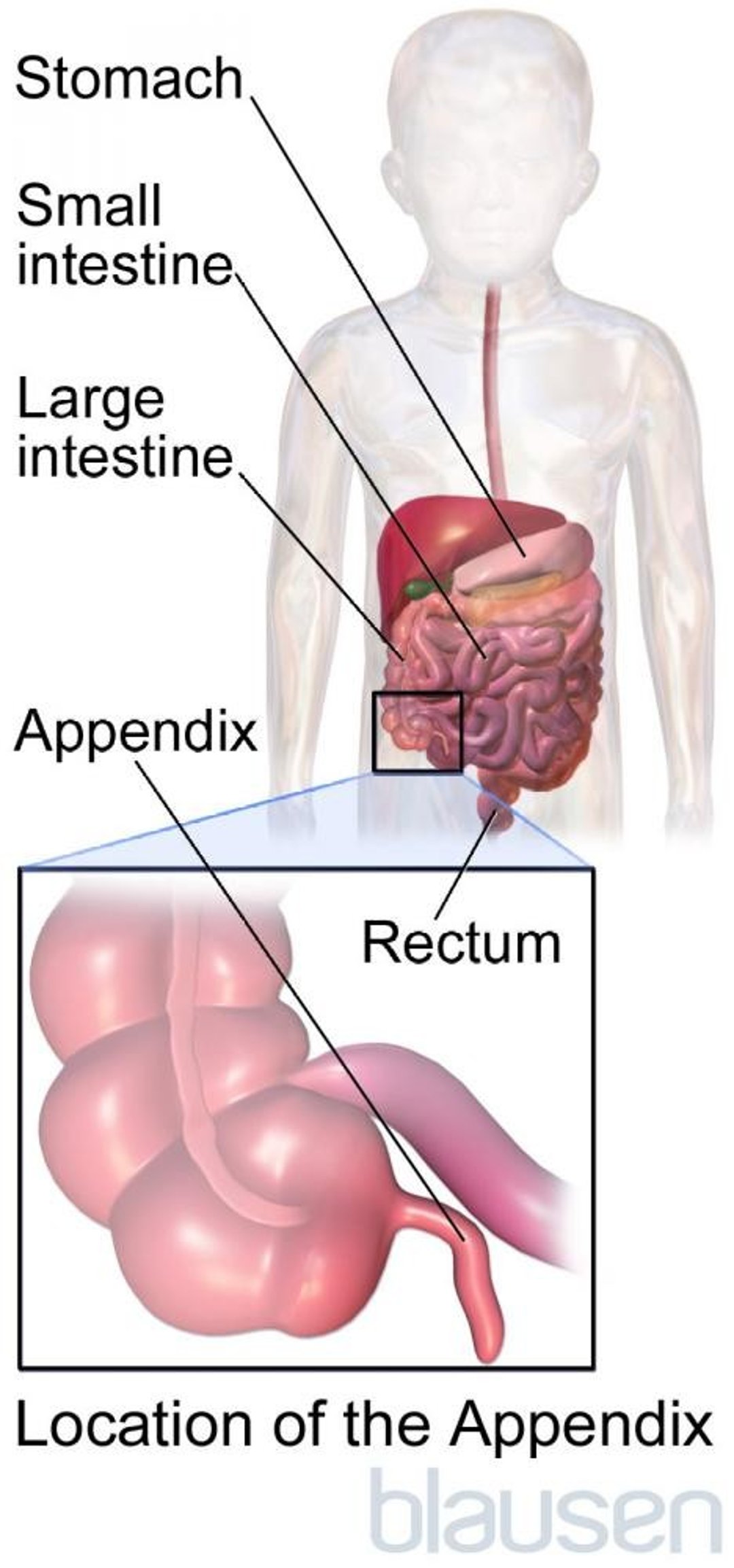
The appendix is a small tube of tissue that is part the of intestines. It is about the length of a finger and is located where the small intestine ends and the large intestine begins. The appendix does not seem to have any essential bodily function.
Appendicitis (inflammation of the appendix) is a medical emergency because it can cause a life-threatening infection. The goal is to detect and treat appendicitis early, before a serious infection occurs.
This disorder is rare in children younger than 1 year but becomes more common as children grow older and is most common among adolescents and adults in their 20s. However, appendicitis may occur at any age.
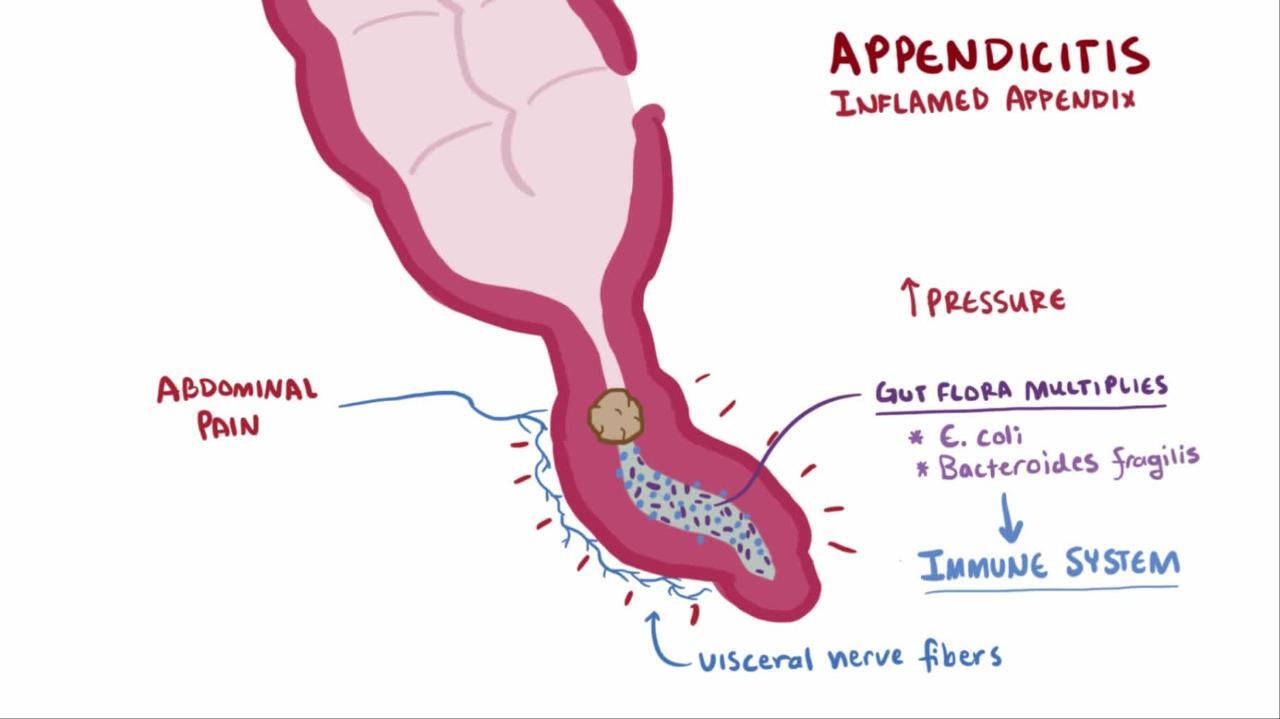
Appendicitis seems to develop when the appendix becomes blocked either by hard fecal material (fecalith) or swollen lymph nodes in the intestine, which can occur with various infections. In either case, the appendix swells, and bacteria in it grow.
Occasionally, swallowed foreign objects, infections with certain parasitic worms (such as strongyloidiasis), or certain types of cancer can also cause appendicitis.
Complications of appendicitis
If appendicitis is unrecognized or untreated, the appendix can rupture (burst open), creating a pocket of infection (abscess) outside the intestine or spilling contents of the intestines into the abdominal cavity, causing a serious infection (peritonitis). The likelihood of the appendix rupturing is higher the younger the child.
Symptoms of Appendicitis
In children who are 2 to 3 years old or older, the order in which symptoms appear is more important than any one symptom itself. The first symptom to develop is pain. Appendicitis almost always causes pain. The pain may start in the middle of the abdomen around the bellybutton and then move to the lower right area of the abdomen. However pain, particularly in infants and children, may be widespread rather than confined to the right lower portion of the abdomen. Younger children may be less able to identify a specific location for the pain and may be only very irritable or listless.
After the pain has begun, many children develop nausea or vomiting and do not want to eat. Then the abdomen is tender when the doctor pushes on it, usually in the area over the appendix. A low-grade fever (100 to 101° F [37.7 to 38.3° C]) develops next and is a common symptom. Lastly, fever is followed by laboratory test results that show infection, such as a high white blood cell count.
This order of symptoms is different from that in children who have viral gastroenteritis, in whom vomiting typically occurs first, and pain and diarrhea develop later. Significant diarrhea is not common among children who have appendicitis.
Diagnosis of Appendicitis
Ultrasonography
Sometimes other imaging tests
Sometimes laparoscopy
The diagnosis of appendicitis in children can be challenging for many reasons. Many disorders can cause similar symptoms, including viral gastroenteritis, Meckel diverticulum, intussusception, and Crohn disease. Often, children, particularly younger children, do not have typical symptoms and physical examination findings, particularly when the appendix is not in its usual position in the right lower part of the abdomen. This lack of typical symptoms can be deceptive.
Most often, doctors do ultrasonography, which does not expose the child to radiation. If the diagnosis is not clear, doctors may do computed tomography (CT) or magnetic resonance imaging (MRI). Doctors who suspect appendicitis usually give fluids and antibiotics by vein. While waiting for results of blood, urine, and imaging tests, the child is asked to stop eating or drinking to prevent complications in case surgery is needed.
If the diagnosis is not clear, doctors may do laparoscopy, in which a small viewing scope is put through the wall of the abdomen to look inside. If appendicitis is found during laparoscopy, doctors can remove the appendix using the laparoscope. Alternatively, especially in children whose symptoms and examination findings are not typical of appendicitis, doctors may do repeated physical examinations. Seeing whether the symptoms and tenderness are getting worse or better with time may help doctors decide whether appendicitis is present. Doctors also note the order in which the symptoms appear.
Treatment of Appendicitis
Appendectomy
Antibiotics by vein
The best treatment for appendicitis is surgical removal of the inflamed appendix (appendectomy). Before surgery, doctors give antibiotics by vein, which decreases the risk of complications. Appendicitis can sometimes be treated successfully with only antibiotics, but even if antibiotic treatment is successful at first, children sometimes develop appendicitis again. Therefore, surgical removal of the appendix is generally the recommended treatment for appendicitis.
Appendectomy is fairly simple and safe, requiring a hospital stay of 1 to 2 days in children who have no complications, such as a ruptured appendix. If the appendix has ruptured, the doctor removes it and may wash out the abdomen with fluid, give antibiotics for several days, and watch for complications, such as infection and bowel blockage. Children who have a ruptured appendix typically need to stay longer in the hospital.
About 15% of the time, surgeons discover a normal appendix while doing an appendectomy. This is because there are no methods that are 100% accurate for diagnosing appendicitis before surgery. Because of the potential life-threatening consequences of appendicitis, proceeding with surgery is considered worth the tradeoff of sometimes doing surgery and finding that the appendix is normal. When this occurs, the surgeon looks in the abdomen for another cause of the pain and treats it if possible. Usually, the doctor removes the appendix, even if it appears normal, because it does not serve any function and removing it will also prevent children from needing an additional surgery if they develop appendicitis in the future.
Prognosis for Appendicitis
With early treatment, the overall prognosis for children who have appendicitis is very good.
If children are not treated until the appendix has ruptured, which occurs most commonly in children under 2 years of age, the prognosis is worse. Some children who have surgery for a ruptured appendix have complications. Some children develop complications even if their appendix did not rupture.
If children are not treated, appendicitis rarely can go away on its own. Usually, however, untreated appendicitis progresses and causes peritonitis, an abdominal abscess, and sometimes death. Appendicitis is rarely fatal; death occurs in fewer than 1 in 1000 children.







