












Cardiac arrest is when the heart stops pumping blood and oxygen to the brain and other organs and tissues. Sometimes a person can be revived after cardiac arrest, particularly if treatment is started immediately. However, the more time that passes without blood being pumped to the brain, the less likely it is that the person can be revived, and, if revived, the more likely it is that the person will have permanent brain damage.
Brain damage is likely if cardiac arrest lasts for more than 5 minutes without the first aid intervention of cardiopulmonary resuscitation (CPR), which pumps oxygen-containing blood from the heart and lungs to the brain and other organs. Death is likely if cardiac arrest lasts for more than 8 minutes without CPR. Thus, CPR for cardiac arrest must be started as quickly as possible.
Cardiac arrest can be caused by anything that makes the heart stop beating. One common cause, especially in adults, is an abnormal heart rhythm (arrhythmia). Another possible cause is stopping breathing (respiratory arrest), such as when a person drowns or has a severe lung infection (pneumonia) or a severe asthma attack.
A person in cardiac arrest lies motionless and does not respond to questions or to stimulation, such as shaking. The person may not be breathing or may have gasping, irregular breaths called agonal breathing. More than two-thirds of all cardiac arrests occur in the home. Therefore, it is important for people to learn to recognize that a friend or family member who is unresponsive and not breathing, or breathing abnormally, is likely in cardiac arrest and requires immediate first aid (CPR) and activating local emergency medical services.
First-Aid Treatment for Cardiac Arrest
The crucial steps that should be done to maximize a person's chance of survival are called the cardiac arrest chain of survival. The survival chain begins with bystander recognition of cardiac arrest and continues through calling for emergency services, providing cardiopulmonary resuscitation (CPR) and defibrillation when available, and prehospital EMS personnel giving high-quality post-arrest care while en route to the hospital and in a hospital. Without successful accomplishment of each of these steps, it is unlikely that a person will survive.
Recognition and treatment of cardiac arrest should ideally occur at virtually the same time. A rescuer, usually a family member or friend, who finds someone unconscious should first determine if the person is unresponsive by shaking the person and loudly asking, "Are you okay?" If there is no response, the rescuer should turn the person's body face up and look to determine whether breathing has also stopped or is not normal.
If the person does not respond to stimulation and is not breathing or is breathing abnormally (for example, gasping), emergency resuscitation with CPR is begun and the local emergency medical service is called (in the United States, by calling 9-1-1). Rescuers should not try to check for a pulse but should start CPR as soon as possible because the risk of doing chest compressions on a person not in cardiac arrest is much lower than the risk of not doing chest compressions when needed.
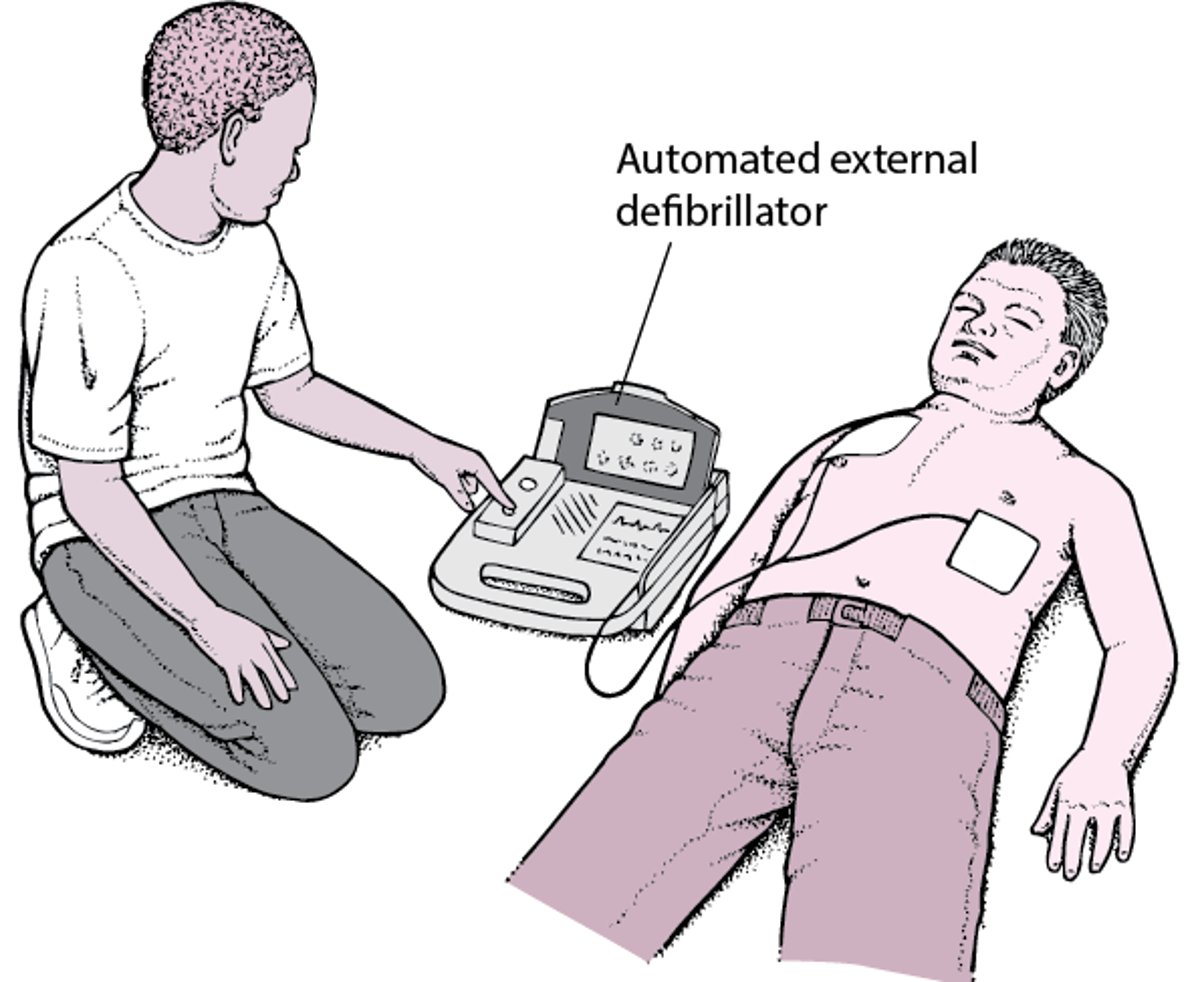
CPR should be started immediately by one rescuer, while a second rescuer contacts emergency services and retrieves an automated external defibrillator (AED) if available. CPR should not be delayed while the AED is retrieved, and the AED may be used as soon as it is available. Some emergency services dispatchers provide instructions over the telephone to help direct care, including giving instruction in how to do compression-only CPR.
An AED can rapidly determine whether the person has an abnormal heart rhythm that can be treated by an electric shock (called defibrillation). If the AED detects an abnormal rhythm that could be corrected, it delivers a shock, which may start the heart beating again. AEDs are easy to use and are available in many public gathering places. Written instructions for use are available on each AED and should be followed. Most AEDs also provide voice prompts on how to use the AED. Several organizations provide training on CPR and the use of AEDs. Taking periodic refresher training can help to remind community members how to perform CPR and use an AED, because procedures may change over time.
The Chain of Survival
The crucial links in the chain of survival include
People who are resuscitated need advanced monitoring and treatment and eventually rehabilitation and other measures to improve recovery. |


Automated External Defibrillator: Jump-Starting the Heart
An automated external defibrillator (AED) is a device that can detect and correct a type of abnormal heart rhythm called ventricular fibrillation. Ventricular fibrillation causes cardiac arrest. AEDs are easy to use. Many organizations provide training sessions on the use of AEDs. Most training sessions take only a few hours, but it is possible to use an AED even if you have never participated in a training course. Different AEDs have somewhat different instructions for use. The instructions are written on the AED, and most AEDs also use voice prompts to direct the user in each step. AEDs are available in many public gathering places, such as stadiums, airports, and concert halls. People who are told by their doctor that they are likely to develop ventricular fibrillation but who do not have an implanted defibrillator may want to purchase an AED for home use by family members, who should be trained in its use. |

There are 2 CPR methods:
Compression-only or hands-only CPR (done by rescuers untrained in—or reluctant to do—rescue breaths)
Standard CPR (done by rescuers trained to provide chest compressions and rescue breaths)
Studies have shown that compressions-only CPR is as effective as standard CPR for adolescents and adults in the first few minutes of cardiac arrest. Standard CPR may be more effective for children and infants, and for people whose cardiac arrest is due to respiratory causes, but only if the rescuer has been trained.
CPR: How Effective Is It Really?
On television and in the movies, people who collapse due to cardiac arrest and receive cardiopulmonary resuscitation (CPR) often awaken during, or after, CPR is performed. In real life, it is much less likely that people will be revived by CPR itself. Instead, CPR is done to circulate oxygen-containing blood from the lungs to the brain and organs until the heart can be restarted with a defibrillator, often with the help of special medications given by emergency medical services personnel. Only a small percentage of people who suffer cardiac arrest will survive until they reach a hospital. Even those who reach the hospital alive often die as a result of the underlying heart problem. Of those people who are able to leave the hospital, many will not regain their normal mental function. The most important factors that influence whether a person will survive cardiac arrest and return to normal life after hospital discharge are early initiation of CPR and early defibrillation. Usually in television or film, CPR is done on a young, relatively healthy person, sometimes someone who has suffered a serious injury. In reality, most people who need CPR are older adults who often have many serious underlying illnesses. These people are much less likely to have a good outcome after CPR. Also, CPR is rarely effective if the cause of cardiac arrest is a traumatic injury. In television and film, the person either dies or recovers fully. In reality, many people who survive cardiac arrest have serious disabilities as a result of the lack of blood flow to the brain. |
Compression-Only CPR
Compression-only (sometimes called hands-only) CPR involves giving continuous chest compressions without rescue breathing. Compression-only CPR is recommended when the rescuer does not have training in standard CPR or is unable or unwilling to do rescue breathing. For infants, children, and people in whom the cause of cardiac arrest seems to be from stopping breathing, such as those who have drowned, standard CPR with rescue breaths is preferred. However, if rescuers are unwilling or unable to do artificial respiration, they should still do compression-only CPR even on people who are thought to have cardiac arrest due to a problem with breathing.
Doing Chest Compressions in an Adult
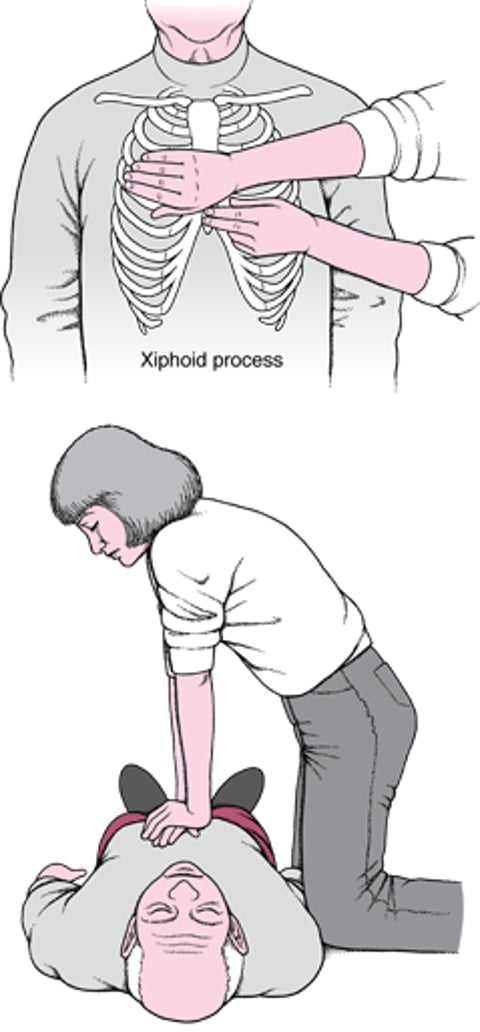
To do chest compressions for cardiopulmonary resuscitation (CPR), a rescuer kneels to one side and, with the arms held straight, leans over the person and places both hands, one on top of the other, just above (about 2 finger widths) the lowest part of the breastbone (called the xiphoid process). The rescuer compresses the chest to at least 2 inches (5 centimeters) in adults. The chest is compressed about 100 to 120 times per minute, allowing it to fully rise back up to its starting height between each compression. |

Doing Chest Compressions in an Infant

Standard CPR
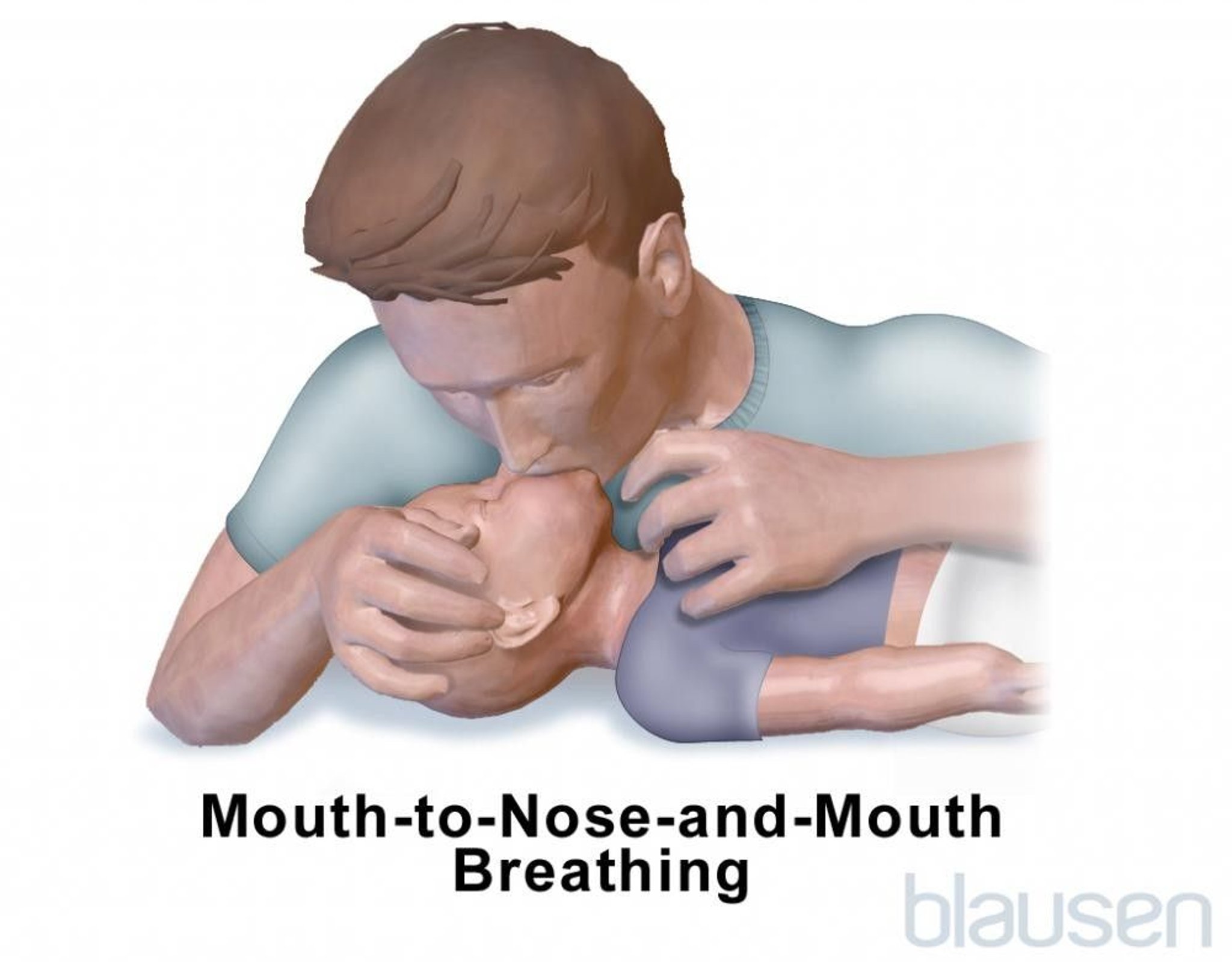
Standard CPR for adults and children combines rescue breathing (mouth-to-mouth resuscitation to supply oxygen to the lungs) with chest compressions that force oxygen-containing blood out of the heart to the brain and other vital organs. Standard CPR for infants combines mouth-to-nose-and-mouth rescue breathing with chest compressions.


MICROGEN IMAGES/SCIENCE PHOTO LIBRARY

The sequence of CPR begins with 30 chest compressions, followed by 2 rescue breaths, and continues in a ratio of 30:2 until the rescuer is relieved by emergency personnel. Chest compressions can quickly tire a person, resulting in compressions that are too weak to circulate blood effectively. Thus, if 2 or more rescuers are present, they should switch every 2 minutes, or sooner if the rescuer performing compressions begins to feel tired.
To do chest compressions in an adult or child, the rescuer lays the person face up, rolling the head, body, and limbs at the same time. The rescuer extends his or her arms and "locks" them straight at the elbows, leans over the person, and places both hands, one on top of the other, in the center of the chest (between the nipples on the breastbone). The rescuer then compresses the chest to a depth of at least 2 inches (5 centimeters) in adults.
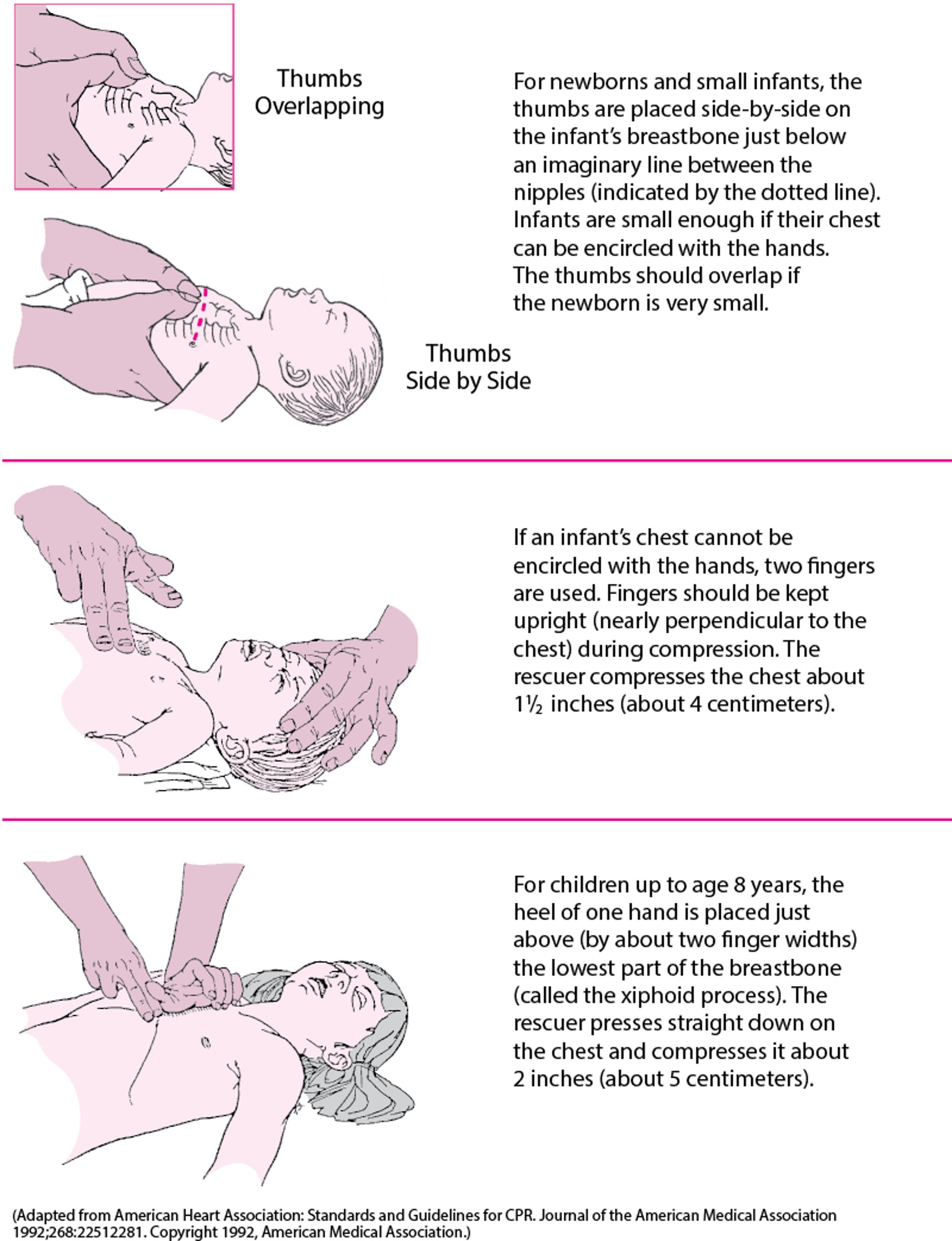
In children, the rescuer compresses the chest about 2 inches (5 centimeters), and may need to use only one hand to compress in a smaller child.
For an infant (up to 1 year old), the rescuer may use 2 fingers to compress the infant's breastbone just below the nipples to a depth of about 1½ inches (about 4 centimeters) or ⅓ the diameter of the chest. Alternatively, trained rescuers may choose to encircle the infant's chest with 2 hands and do compressions with their thumbs.
It is important to allow the chest to fully rise back up to its starting height between each compression.
Opening an Airway in an Adult or Child
After doing 30 compressions, the rescuer tilts the person's head back slightly and lifts the chin, which moves the tongue away from blocking the airway. The rescuer then pinches the person's nose shut, takes a normal breath, seals the mouth over the person's mouth, and blows into the person's mouth for long enough to make the person's chest just rise (about 1 second). This is repeated a second time, followed immediately by another 30 compressions. |

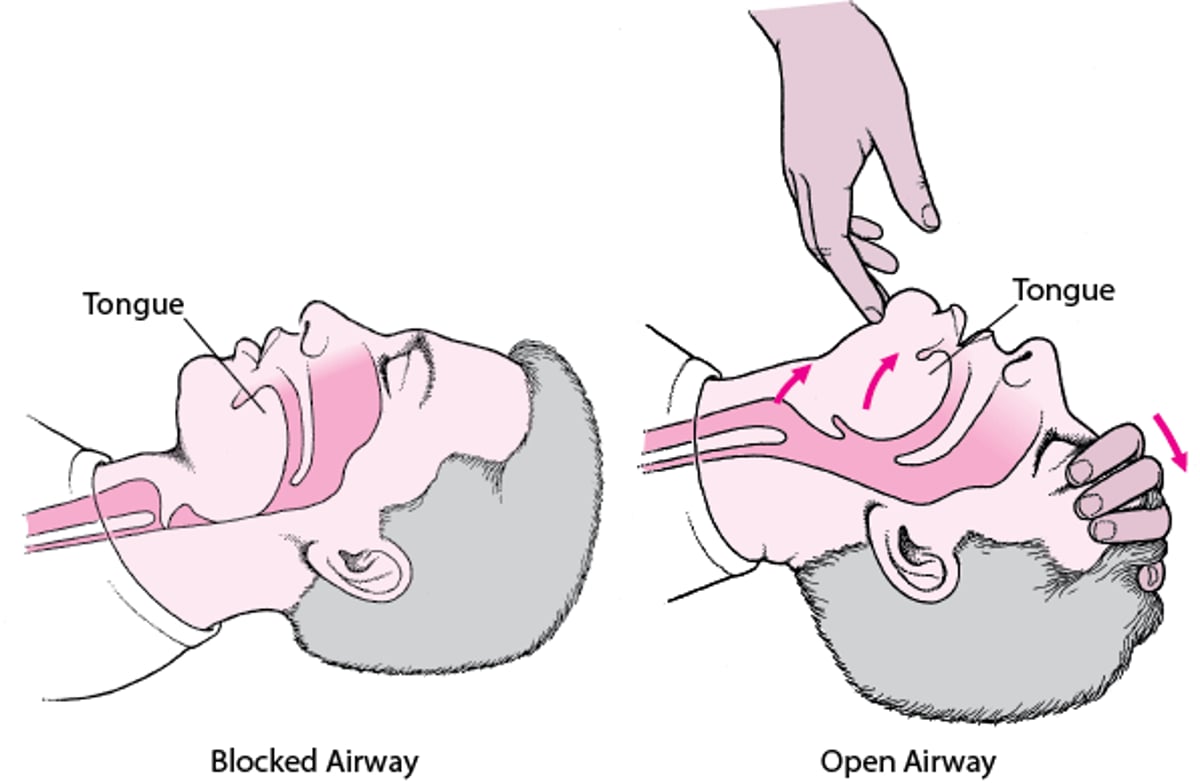
To do rescue breaths, the rescuer first looks in the mouth and throat for any visible objects that may be blocking the airway and, if any are present, removes them. The rescuer then opens the airway by tilting the person's head and lifting the chin (see figure Opening an Airway in an Adult or Child). If a neck or spine injury is suspected, the rescuer should not tilt the person's head. Instead the angle of the jaw is lifted while the head is kept in a neutral position without flexing or extending the neck. The rescuer's mouth covers the person's mouth and then the rescuer exhales air into the person's lungs (rescue breaths). The person's airway must remain open during artificial respiration. To prevent air from escaping from the person's nose, the person's nose can be pinched shut as the rescuer exhales into the mouth (see photo Mouth-to-Mouth Breathing for an Adult or Child). Artificial respiration is very similar in children and adults.
For artificial respiration on an infant, the rescuer's mouth covers the infant's mouth and nose. To prevent damaging the infant's smaller lungs, the rescuer exhales with less force than with adults. If the chest rises, the rescuer should give 2 deep, slow breaths. If the chest does not rise after properly delivering rescue breaths, it is likely that the infant's airway is blocked; however, CPR should continue. The compressions themselves can force air out of the lungs, dislodging the object that is blocking the infant's airway. Each time the airway is opened during CPR to provide rescue breaths, the rescuer should look for an object in the infant’s mouth and, if one is found, remove it.
Standard CPR can be done by one person (a single person alternately does rescue breaths and chest compressions) or by 2 people (one to do rescue breaths and one to do chest compressions). In standard CPR, a single rescuer gives 30 compressions and then 2 breaths. If 2 rescuers are present, when children or infants need CPR, a ratio of 15:2 is preferred. In newborns, a ratio of 1 breath to every 3 compressions (3:1) is recommended, for a total of 40 to 60 breaths per minute. Compressions are done at a rate of 100 to 120 times per minute in people of all ages. CPR is continued until medical assistance arrives or the person begins to move or breathe on their own.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
American Heart Association, Cardiopulmonary Resuscitation (CPR) & First Aid Emergency Cardiovascular Care (ECC): This resource offers access to CPR courses and training programs, kits with useful teaching aids (including practice dummies), and information on resuscitation science.
American Red Cross, Cardiopulmonary Resuscitation (CPR) Training: This resource offers access to online CPR training and certification courses in adult CPR, hands-only CPR, child and baby CPR, and pet CPR; supplies and products; and a locator for finding online and live training sessions.




