


Infective endocarditis is an infection of the lining of the heart (endocardium) and usually also of the heart valves.
Infective endocarditis occurs when bacteria enter the bloodstream and travel to and attach to previously injured heart valves.
Acute infective endocarditis usually begins suddenly with a high fever, fast heart rate, fatigue, and rapid and extensive heart valve damage.
Subacute infective endocarditis gradually causes such symptoms as fatigue, mild fever, a moderately fast heart rate, weight loss, sweating, and a low red blood cell count.
Echocardiography is used to detect the damaged heart valves, and blood cultures are used to identify the microorganism causing infective endocarditis.
People with artificial heart valves or certain birth defects of the heart need to take antibiotics to prevent endocarditis before they undergo certain dental or surgical procedures.
High doses of antibiotics are given intravenously, but sometimes surgery is needed to repair or replace damaged heart valves.
Infective endocarditis affects twice as many men as women at all ages. It is more common among older adults.
Infective endocarditis refers specifically to infection of the lining of the heart, but the infection usually also affects the heart valves and any areas with abnormal connections between the chambers of the heart or its blood vessels (birth defects of the heart).
There are 2 forms of infective endocarditis:
Acute infective endocarditis develops suddenly and may become life threatening within days.
Subacute infective endocarditis (also called subacute bacterial endocarditis) develops gradually and subtly over a period of weeks to several months but also can be life threatening.
Prosthetic valve endocarditis is acute infective endocarditis in a heart valve that has been replaced (prosthetic valve).
Endocarditis can also be noninfective. In noninfective endocarditis, blood clots that do not contain microorganisms form on heart valves and adjacent endocardium. Noninfective endocarditis sometimes leads to infective endocarditis because microorganisms can attach to and grow within the fibrous blood clots.
In both infective and noninfective endocarditis, accumulations of blood clots (and bacteria in infectious endocarditis) can break free from the heart wall (becoming emboli), travel through the bloodstream, and block an artery. This blockage may cause a stroke or damage to the spleen, kidneys, or other organs.

Causes of Infective Endocarditis
Bacteria (or, less often, fungi) that are introduced into the bloodstream can sometimes lodge on heart valves and infect the endocardium. Abnormal, damaged, or replacement (prosthetic) valves are more susceptible to infection than normal valves. The bacteria that cause subacute infective endocarditis nearly always infect abnormal, damaged, or replacement valves. However, normal valves can be infected by some aggressive bacteria, especially if many bacteria are present.
Although bacteria are not normally found in the blood, an injury to the skin, lining of the mouth, or gums (even an injury from a normal activity such as chewing or brushing the teeth) can allow a small number of bacteria to enter the bloodstream. Gingivitis (inflammation of the gums) with infection, minor skin infections, and infections elsewhere in the body may introduce bacteria into the bloodstream.
Certain surgical, dental, and medical procedures may also introduce bacteria into the bloodstream. Rarely, bacteria are introduced into the heart during open-heart surgery or heart valve replacement surgery. In people with normal heart valves, usually no harm is done, and the body's white blood cells and immune responses rapidly destroy these bacteria. However, damaged heart valves may trap the bacteria, which can then lodge on the endocardium and start to multiply.
Sepsis, a severe blood infection, introduces a large number of bacteria into the bloodstream. When the number of bacteria in the bloodstream is large enough, endocarditis can develop, even in people who have normal heart valves.


If the cause of infective endocarditis is injection of illicit drugs or prolonged use of intravenous lines (sometimes used by doctors to deliver long-term intravenous therapies for people who have serious medical conditions), the tricuspid valve (which opens from the right atrium into the right ventricle) is most often infected. In most other cases of endocarditis, the mitral valve or the aortic valve is infected.
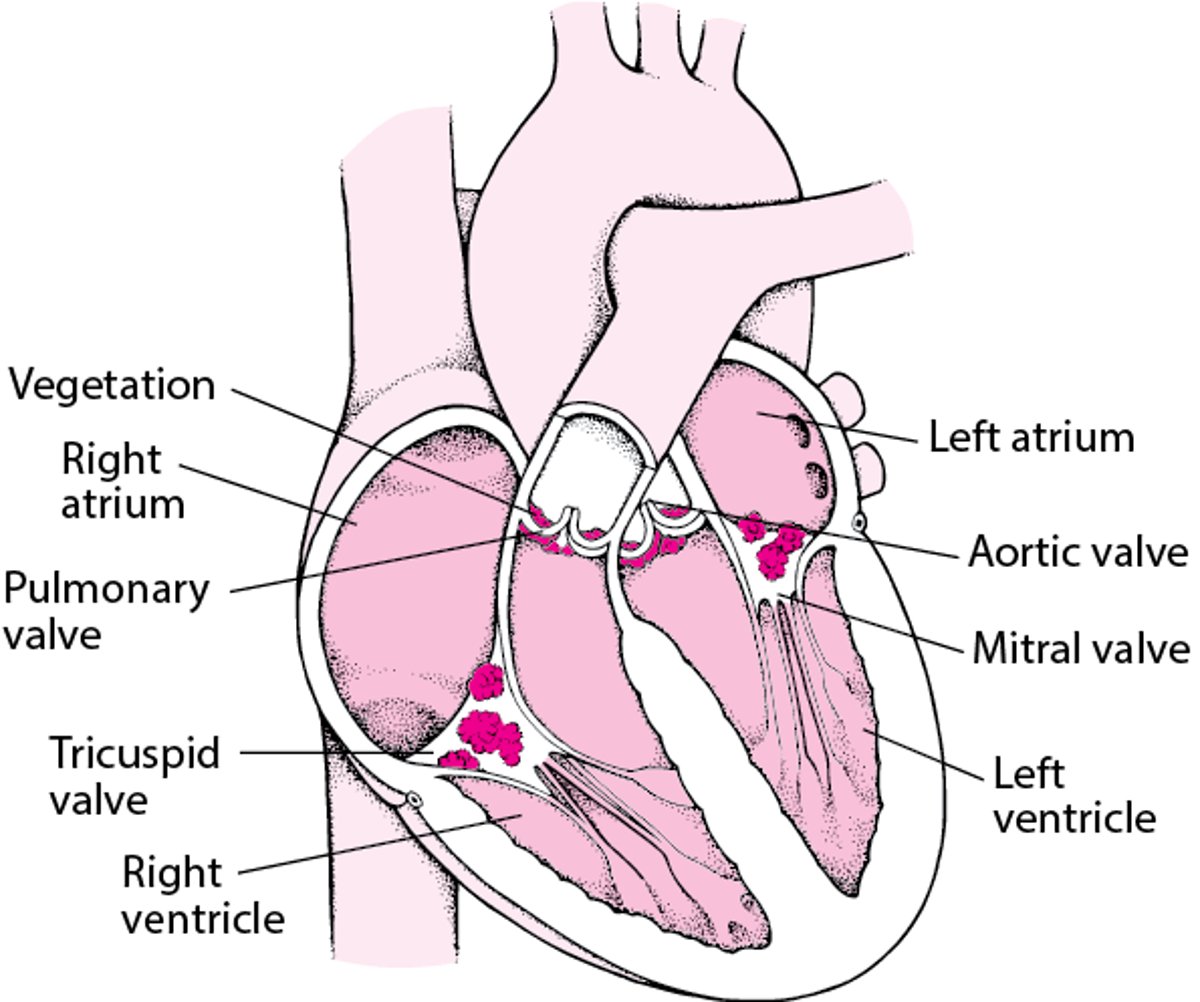
An Inside View of Infective Endocarditis
This cross-sectional view shows vegetations (accumulations of bacteria and blood clots) on the 4 valves of the heart. |

Risk Factors for Infective Endocarditis
The highest risk of endocarditis is in people who
Inject illicit drugs
Have a weakened immune system
Have a prosthetic (artificial) heart valve, pacemaker, or defibrillator
People who inject illicit drugs are at high risk of endocarditis because they are likely to inject bacteria directly into their bloodstream through dirty needles, syringes, or drug solutions.
People who have weakened immune system are less able to remove or inactivate bacteria from the bloodstream and prevent them from infecting the heart.
People who have a replacement heart valve or heart device are also at high risk. For people who have a replacement heart valve, the risk of infective endocarditis is greatest during the first year after heart valve surgery. After the first year, the risk decreases but remains slightly higher than normal.
Other risk factors for infective endocarditis are
Birth defects of the heart (including defects of the heart valves), or major blood vessels, particularly a defect that allows blood to leak from one part of the heart to another
Heart valve damage due to rheumatic fever
Degeneration of the heart valves that occurs with aging
Birth defects are risk factors for children and young adults.
Damage to the heart by rheumatic fever during childhood (rheumatic heart disease) is also a risk factor. Rheumatic fever has become a less common risk factor in countries where antibiotics are widely available. In such countries, rheumatic fever is a risk factor for people who did not have the benefit of antibiotics during their childhood.
One risk factor for older adults is degeneration of the heart valves such as a floppy mitral valve (which opens from the left atrium into the left ventricle) or calcium deposits on the aortic valve (which opens from the left ventricle into the aorta).
Symptoms of Infective Endocarditis
Acute infective endocarditis usually begins suddenly with a high fever (102° to 104°F [38.9° to 40°C]), fast heart rate (typically > 100 beats per minute), fatigue, and rapid and extensive heart valve damage, causing symptoms of heart failure.
Subacute infective endocarditis may cause such symptoms as fatigue, mild fever (99° to 101° F [37.2° to 38.3°C]), a moderately fast heart rate (faster than their usual heart rate), weight loss, sweating, and a low red blood cell count (anemia). These symptoms can be subtle and may occur for months before endocarditis results in blockage of an artery or damages heart valves and thus makes the diagnosis clear to doctors.
In both acute and subacute infective endocarditis, arteries may become blocked if accumulations of bacteria and blood clots on the valves (called vegetations) break loose (becoming emboli), travel through the bloodstream to other parts of the body, and lodge in an artery, blocking it. Sometimes blockage can have serious consequences. Blockage of an artery to the brain can cause a stroke, and blockage of an artery to the heart can cause a heart attack. Emboli can also cause an infection in the area in which they lodge and/or block small blood vessels and damage organs. Organs that are often affected include the lungs, kidneys, spleen, and brain. Emboli also often travel to the skin and back of the eye (retina). Collections of pus (abscesses) may develop at the base of infected heart valves or wherever infected emboli settle.
Heart valves may become perforated and may start to leak (causing regurgitation) — within a few days. Some people go into shock, and their kidneys and other organs stop functioning (a condition called septic shock). Infections in arteries can weaken artery walls, causing them to bulge or rupture. A rupture can be fatal, particularly if it occurs in the brain or near the heart.
Other symptoms of acute and subacute infective endocarditis may include
Chills
Joint pain
Paleness (pallor)
Painful nodules under the skin
Confusion
Tiny reddish spots that resemble freckles may appear on the skin and in the whites of the eyes. Small streaks of red (called splinter hemorrhages) may appear under the fingernails. These spots and streaks are caused by tiny emboli that have broken off the heart valves. Larger emboli may cause stomach pain, blood in the urine, or pain or numbness in an arm or a leg as well as a heart attack or a stroke. Heart murmurs may develop, or preexisting ones may change. The spleen may enlarge.


Reddish spots on the palm and finger of the hand can be seen in people who have endocarditis.
© Springer Science+Business Media


Reddish spots in the white of the eye can be seen in people who have endocarditis.
© Springer Science+Business Media


Small streaks of red can be seen under the fingernails in people who have infective endocarditis.
Image courtesy of CDC/Dr. Thomas F. Sellers via the Centers for Disease Control and Prevention Public Health Image Library.
Reddish spots on the palm and finger of the hand can be seen in people who have endocarditis.
© Springer Science+Business Media
Reddish spots in the white of the eye can be seen in people who have endocarditis.
© Springer Science+Business Media
Small streaks of red can be seen under the fingernails in people who have infective endocarditis.
Image courtesy of CDC/Dr. Thomas F. Sellers via the Centers for Disease Control and Prevention Public Health Image Library.
Prosthetic valve endocarditis may be an acute or subacute infection. Compared with infection of a natural valve, infection of a replacement valve is more likely to spread to the heart muscle at the base of the valve and can loosen the attachment of the valve to the heart. Alternatively, the heart's electrical conduction system may be interrupted, resulting in slowing of the heartbeat, which may lead to a sudden loss of consciousness or even death.
Diagnosis of Infective Endocarditis
Echocardiography
Blood cultures
Because many of the symptoms are vague and general, doctors may have difficulty making a diagnosis. Usually, people suspected of having acute or subacute infective endocarditis are hospitalized promptly for diagnosis as well as treatment.
Doctors may suspect endocarditis in people with a fever and no obvious source of infection, especially if they have
Characteristic symptoms such as reddish spots on fingers or the whites of the eyes
A heart valve disorder
A replacement heart valve
Recently had certain surgical, dental, or medical procedures
Injected illicit drugs
Development of a heart murmur or a change in a preexisting heart murmur further supports the diagnosis.
To help make the diagnosis, doctors usually do echocardiography and obtain blood samples to test for the presence of bacteria. Usually, 3 or more blood samples are taken at different times on the same day. These blood tests (blood cultures) may identify the specific disease-causing bacteria and the best antibiotics to use against them. In people with heart abnormalities, doctors test their blood for bacteria before giving them antibiotics.
Echocardiography, which uses ultrasound waves, can produce images showing heart valve vegetations and damage to the heart. Typically, transthoracic echocardiography (a procedure in which the ultrasound probe is placed on the chest) is done. If this procedure does not provide enough information, the person may undergo transesophageal echocardiography (a procedure in which the ultrasound probe is passed down the throat into the esophagus just behind the heart). Transesophageal echocardiography is more accurate and detects smaller bacterial deposits, but it is invasive.
Computed tomography (CT) is used occasionally when transesophageal echocardiography does not provide enough information. Positron emission tomography (PET) is sometimes used for the diagnosis of infective endocarditis of prosthetic heart valves and other devices placed in the heart.
Sometimes bacteria that cause endocarditis cannot be cultured from blood samples. Special techniques may be needed to grow the particular bacteria, or the person may have taken antibiotics that did not cure the infection but did reduce the number of bacteria enough to be undetectable. Another possible explanation is that the person does not have endocarditis but has another condition, such as a heart tumor or noninfective endocarditis, that causes symptoms very similar to those of endocarditis.
Treatment of Infective Endocarditis
Antibiotics given by vein (intravenously)
Sometimes heart surgery
Treatment usually consists of at least 2 weeks and often up to 8 weeks of antibiotics given by vein (intravenously) in high doses. Antibiotic therapy is almost always started in the hospital but may be finished at home with the help of a home nurse. Some people with certain types of infection may be able to switch to antibiotics taken by mouth after a period of intravenous treatment.
Antibiotics alone do not always cure an infection, particularly if the valve is one that has been replaced. One reason is that the bacteria that cause endocarditis in a person with a replacement valve are often resistant to antibiotics. Because antibiotics are given before heart valve replacement surgery to prevent infection, any bacteria that survive this treatment to cause infection are probably resistant. Another reason is that it is generally harder to cure infection on artificial, implanted material than in human tissue.
Heart surgery may be needed to repair or replace damaged valves, remove vegetations, or drain abscesses if antibiotics do not work, a valve leaks significantly, or a birth defect connects one chamber to another.
Dental treatment to eliminate any sources of infection due to mouth or gum disease is usually needed. Doctors usually also remove any devices (such as catheters) that may be a source of infection.
Doctors may use a series of echocardiography examinations to ensure that the infected area is decreasing. They may also do echocardiography at the end of treatment to have a record of the appearance of heart valves because infective endocarditis may recur. Because of the risk of recurrence, ongoing dental care and good skin hygiene (to prevent any bacteria from entering the body through sores or wounds) is needed.
Prognosis for Infective Endocarditis
If untreated, infective endocarditis is always fatal. When treatment is given, the risk of death depends on factors such as the person's age, duration of the infection, the presence of a replacement heart valve, the type of infecting organism, and the amount of damage done to the heart valves. Nonetheless, with aggressive antibiotic treatment, most people survive.
Prevention of Infective Endocarditis
As a preventive measure, people at high risk of infective endocarditis are given antibiotics before certain surgical, dental, and medical procedures. People at high risk include those with
Replacement valves
Some birth defects of the heart
A transplanted heart that has an abnormal valve
A previous episode of infective endocarditis
Consequently, surgeons, dentists, and other health care practitioners need to know if a person has such risk factors. People who simply have an abnormal heart valve alone do not require antibiotics.
Examples of Procedures That Require Preventive Antibiotics in the United States*
Type of Procedure† | Examples |
|---|---|
Dental | Tooth extraction Periodontal procedures such as gum surgery, scaling, root planing, and probing Placement of dental implants Replacement of a tooth that was knocked out Root canal surgery beyond the end of the root Cleanings if bleeding is expected to result |
Lungs and respiratory tract | Removal of tonsils or adenoids Sometimes bronchoscopy Procedures done in a person who has an infection |
* In people at high risk of developing infective endocarditis, antibiotics are needed. | |
† Antibiotics may be needed before some procedures of the digestive tract, genital or urinary tract, skin, or muscles if an infection is already present in the tissue. | |







