


High blood pressure (hypertension) is persistently high pressure in the arteries.
")


Often no cause for high blood pressure can be identified, but sometimes it occurs as a result of an underlying disorder of the kidneys or a hormonal disorder.
Obesity, a sedentary lifestyle, stress, smoking, and excessive amounts of alcohol or sodium (salt) in the diet all can play a role in the development of high blood pressure in people who have an inherited tendency to develop it.
In most people, high blood pressure causes no symptoms.
Doctors make the diagnosis after measuring blood pressure on 2 or more occasions.
People are advised to lose weight, stop smoking, and decrease the amounts of sodium and fats in their diet.
Antihypertensive medications are given.
To many people, the word hypertension suggests excessive tension, nervousness, or stress. In medical terms, hypertension refers to persistently high blood pressure, regardless of the cause. Because it usually does not cause symptoms for many years—until a vital organ is damaged—high blood pressure has been called the silent killer. Uncontrolled high blood pressure increases the risk of problems such as stroke, aneurysm, heart failure, heart attack, and chronic kidney disease.
Nearly half of adults in the United States have high blood pressure. Many people are not aware that they have high blood pressure. About 80% of adults with high blood pressure have had treatment recommended, but only about half of them actually receive treatment.
High blood pressure occurs more often in non-Hispanic Black adults (58%) compared with 49% of non-Hispanic White adults and 45% of non-Hispanic Asian adults, or 39% of Hispanic adults. High blood pressure occurs more often in older adults—in about two-thirds of people over the age of 65 years. People who have normal blood pressure at age 55 have a 90% risk of developing high blood pressure at some point in their life. High blood pressure is twice as common among people who have obesity as among those who do not.
When blood pressure is checked, 2 values are recorded. The higher value reflects the highest pressure in the arteries, which is reached when the heart contracts (called systole). The lower value reflects the lowest pressure in the arteries, which is reached just before the heart begins to contract again (called diastole). Blood pressure is written as systolic pressure/diastolic pressure—for example, 120/80 mm Hg (millimeters of mercury). This reading is referred to as "120 over 80."

Classification of blood pressure
Blood pressure in adults is classified as normal, elevated blood pressure, stage 1 (mild) hypertension, or stage 2 hypertension. However, these classifications are somewhat arbitrary since the higher the blood pressure, the greater the risk of contributions - even within the normal blood pressure range.
Classification of Blood Pressure in Adults*
Classification | Blood Pressure (mm Hg) |
|---|---|
Normal blood pressure | Less than 120/80 |
Elevated blood pressure | 120–129/less than 80 |
Stage 1 high blood pressure | 130–139 (systolic blood pressure) or 80–89 (diastolic blood pressure) |
Stage 2 high blood pressure | 140 (systolic blood pressure) or higher or 90 (diastolic blood pressure) or higher |
* People who have systolic and diastolic blood pressures in different categories are considered to be in the higher blood pressure category. | |
Information is based on the 2017 Guidelines for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults issued by the American College of Cardiology and the American Heart Association. | |
Ahypertensive urgency is a systolic blood pressure that is more than 180 mm Hg and/or a diastolic blood pressure that is more than 120 mm Hg but has not yet caused any organ damage that is apparent to people or their doctors. A hypertensive urgency usually does not cause symptoms.
A hypertensive emergency is a particularly severe form of high blood pressure. Systolic blood pressure is at least 180 mm Hg and/or diastolic blood pressure is at least 120 mm Hg, and there is evidence of progressive damage in one or more vital organs (typically the brain, heart, and kidneys), often accompanied by a variety of symptoms. If untreated, a hypertensive emergency can be fatal.
The Body's Control of Blood Pressure
The body has many mechanisms to control blood pressure. The body can change the
Amount of blood the heart pumps
Diameter of arteries
Volume of blood in the bloodstream
To increase blood pressure, the heart can pump more blood by pumping more forcefully or more rapidly. Small arteries (arterioles) can narrow (constrict), forcing the blood from each heartbeat through a narrower space than normal. Because the space in the arteries is narrower, the same amount of blood passing through them increases the blood pressure. Veins can constrict to reduce their capacity to hold blood, forcing more blood into the arteries. As a result, blood pressure increases. Fluid can be added to the bloodstream to increase blood volume and thus increase blood pressure.


To decrease blood pressure, the heart can pump slower or less forcefully, arterioles and veins can widen (dilate), and fluid can be removed from the bloodstream.
These mechanisms are controlled by the sympathetic division of the autonomic nervous system (the part of the nervous system that regulates internal body processes requiring no conscious effort) and by the kidneys.
The sympathetic division uses several means to temporarily increase blood pressure during the fight-or-flight response (the body's physical reaction to a threat).
The sympathetic division stimulates the adrenal glands to release the hormones epinephrine (adrenaline) and norepinephrine (noradrenaline). These hormones stimulate the heart to beat faster and more forcefully, most arterioles to constrict, and some arterioles to dilate. The arterioles that dilate are those in areas where an increased blood supply is needed (such as in skeletal muscle—the muscles controlled by conscious effort).
The sympathetic division also stimulates the kidneys to decrease their excretion of sodium and water, thereby increasing blood volume. The body controls the movement of sodium in and out of cells, to prevent an excess of sodium inside cells. Excessive amounts of sodium inside cells can cause the body to become overly sensitive to stimulation by the sympathetic division.

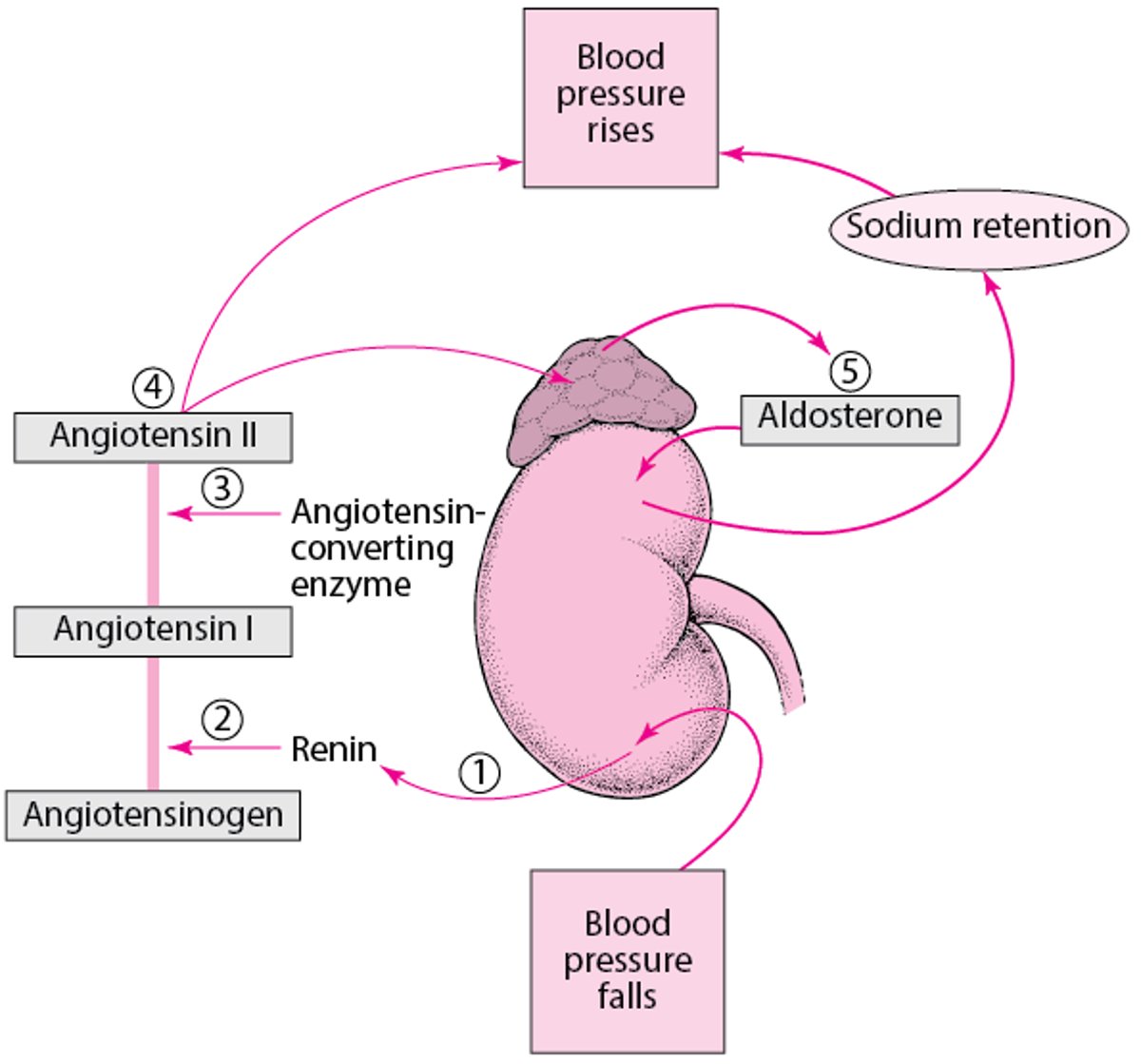
The kidneys also respond directly to changes in blood pressure. If blood pressure increases, the kidneys increase their excretion of sodium and water, so that blood volume decreases and blood pressure returns to normal. Conversely, if blood pressure decreases, the kidneys decrease their excretion of sodium and water, so that blood volume increases and blood pressure returns to normal. The kidneys can increase blood pressure by secreting the enzyme renin, which eventually results in the production of the hormone angiotensin II.
Angiotensin II helps increase blood pressure by
Causing the arterioles to constrict
Triggering the sympathetic division of the autonomic nervous system
Triggering the release of 2 other hormones, aldosterone and vasopressin (also called antidiuretic hormone), which cause the kidneys to increase retention of sodium and water
The kidneys normally produce substances that cause arterioles within the kidneys to dilate. This helps balance the effects of hormones that cause constriction of arterioles.
Blood pressure varies naturally over a person’s life. Infants and children normally have much lower blood pressure than adults. For almost everyone living in industrialized countries such as the United States, blood pressure increases with aging.
Regulating Blood Pressure: The Renin-Angiotensin-Aldosterone System
The renin-angiotensin-aldosterone system is a series of reactions designed to help regulate blood pressure.
|

Activity temporarily affects blood pressure, which is higher when a person is active and lower when a person rests. Blood pressure also varies with the time of day. It is highest in the morning and lowest at night during sleep. These variations are normal. Whenever a change causes a transient increase in blood pressure, one of the body's compensatory mechanisms is triggered to counteract the change and keep blood pressure at normal levels. For example, an increase in the amount of blood pumped out by the heart—which tends to increase blood pressure—causes dilation of blood vessels and an increase in the kidneys' excretion of sodium and water—which tend to reduce blood pressure.
Causes of High Blood Pressure
High blood pressure may be
Primary
Secondary
Primary hypertension


High blood pressure with no known cause is called primary (formerly called essential) hypertension. About 85% of people with high blood pressure have primary hypertension.
Several changes in the heart and blood vessels probably combine to increase blood pressure. For instance, the amount of blood pumped per minute (cardiac output) may be increased, and the resistance to blood flow may be increased because blood vessels are constricted. Blood volume may be increased also. The reasons for such changes are not fully understood but appear to involve an inherited abnormality affecting the constriction of arterioles, which help control blood pressure.
Other changes may contribute to increases in blood pressure, including accumulation of excessive amounts of sodium inside cells and decreased production of substances that dilate arterioles.
Secondary hypertension
High blood pressure with a known cause is called secondary hypertension. About15% of people with high blood pressure have secondary hypertension.
In many of these people, high blood pressure results from
A kidney disorder
Many kidney disorders can cause high blood pressure because the kidneys are important in controlling blood pressure. Damage to the kidneys may impair their ability to remove enough sodium and water from the body, increasing blood volume and blood pressure. Kidney disorders that cause high blood pressure include renal artery stenosis (narrowing of the artery supplying one of the kidneys which may be due to atherosclerosis), kidney infection (pyelonephritis), glomerulonephritis, kidney tumors, polycystic kidney disease, injury to a kidney, and radiation therapy affecting a kidney.
In other people, secondary hypertension is caused by another disorder, such as
Hormonal disorders
Use of certain medications or other substances
Hormonal disorders that cause high blood pressure include hyperaldosteronism (overproduction of aldosterone, often by a noncancerous tumor in one of the adrenal glands), Cushing syndrome (a disorder characterized by high levels of cortisol), hyperthyroidism (an overactive thyroid gland), and, rarely, a pheochromocytoma (a tumor that is located in an adrenal gland and that produces the hormones epinephrine and norepinephrine).
Substances that can cause or worsen high blood pressure include alcohol (excessive use), stimulants (eg amphetamines, cocaine), medications such as corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives (birth control pills), sympathomimetics (certain decongestants in cold remedies, such as pseudoephedrine and phenylephrine), and licorice. ), medications such as corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives (birth control pills), sympathomimetics (certain decongestants in cold remedies, such as pseudoephedrine and phenylephrine), and licorice.
Arteriosclerosis interferes with the body's control of blood pressure, increasing the risk of high blood pressure. Arteriosclerosis makes arteries stiff, preventing the dilation that would otherwise return blood pressure to normal.
Other disorders that may cause high blood pressure include coarctation of the aorta, preeclampsia, acute intermittent porphyria, and acute lead poisoning.
Contributing factors
Obesity, a sedentary lifestyle, stress, smoking, and excessive amounts of alcohol or sodium in the diet all can play a role in the development of high blood pressure in people who have an inherited tendency to develop it. Additionally, sleep apnea can contribute to or aggravate existing high blood pressure.
Stress tends to cause blood pressure to increase temporarily, but blood pressure usually returns to normal once the stress is over. An example is "white coat hypertension," in which the stress of visiting a doctor's office causes blood pressure to increase to a level considered elevated or even high blood pressure. These temporary increases are one of the reasons why doctors now measure blood pressure several times on several different visits before making the diagnosis of high blood pressure. One high reading out of several may be due to stress, but if blood pressure is consistently high, it is unwise to chalk it up to stress. If doctors think the stress of visiting a doctor's office may be contributing to a person's high blood pressure readings, 24-hour blood pressure monitoring may be used.
Anxiety can also cause high blood pressure, and doctors can determine whether treatment for anxiety is appropriate, which may in turn lower the person's blood pressure.
Symptoms of High Blood Pressure
In most people, high blood pressure causes no symptoms. Certain symptoms are widely, but erroneously, attributed to high blood pressure (such as headaches, nosebleeds, dizziness, a flushed face, and fatigue). These symptoms are common in the entire population and occur no more frequently in people with high blood pressure than in people with normal blood pressure.
However, in some cases when the blood pressure elevation is severe (defined as systolic blood pressure ≥ 180 mm Hg and/or diastolic blood pressure ≥ 120 mm Hg) and untreated, it can lead to symptoms caused by damage to the brain, eyes, heart, and kidneys. People who develop such symptoms and have severely elevated blood pressure have a hypertensive emergency and require emergency treatment. The symptoms can include nausea, vomiting, shortness of breath, restlessness, and an unusual or unexplained headache or fatigue. Occasionally, severe high blood pressure can cause the brain to swell, resulting in nausea, vomiting, worsening headache, drowsiness, confusion, seizures, sleepiness, and even coma. This condition is called hypertensive encephalopathy.
Severe high blood pressure increases the workload of the heart and may cause chest pain and/or shortness of breath. Sometimes very high blood pressure causes the large artery that carries blood from the heart (the aorta) to tear, causing chest or abdominal pain.
If high blood pressure is due to a pheochromocytoma (a rare tumor in the adrenal glands), symptoms may include severe headache, anxiety, an awareness of a rapid or irregular heart rate (palpitations), excessive perspiration, tremor, and paleness. These symptoms result from high levels of the hormones epinephrine and norepinephrine, which are secreted by the pheochromocytoma.
Did You Know...
|
Complications of high blood pressure
Long-standing high blood pressure can damage the heart and blood vessels and increase the risk of
With longstanding high blood pressure, the heart enlarges and the heart's walls thicken because the heart has to work harder to pump blood. The thickened walls are stiffer than normal. Consequently, the heart's chambers do not expand normally and are harder to fill with blood, further increasing the heart's workload. These changes in the heart may result in abnormal heart rhythms or heart failure.
High blood pressure causes thickening of the walls of blood vessels and also makes them more likely to develop hardening of the arteries (atherosclerosis). People with thickened blood vessel walls and atherosclerosis are at higher risk of stroke, heart attack, vascular dementia, and kidney failure. Stroke and heart attack are considered atherosclerotic cardiovascular disease (ASCVD).
Diagnosis of High Blood Pressure
Measuring blood pressure
For the most accurate readings, those that are used to diagnose someone with high blood pressure as opposed to a casual check, doctors follow a specific protocol when measuring blood pressure (see Measuring Blood Pressure). Blood pressure is measured after a person sits for 5 minutes. The person must have had no exercise, caffeine, or tobacco use for at least 30 minutes before the measurement. A reading of 130/80 mm Hg or more is considered high, but a diagnosis cannot be based on a single high reading. Sometimes, even several high readings are not enough to make the diagnosis—because, for example, the readings may vary too much. If a person has an initial high reading, blood pressure is measured again during the same visit and then measured twice on at least 2 other days to make sure that the high blood pressure is still present.
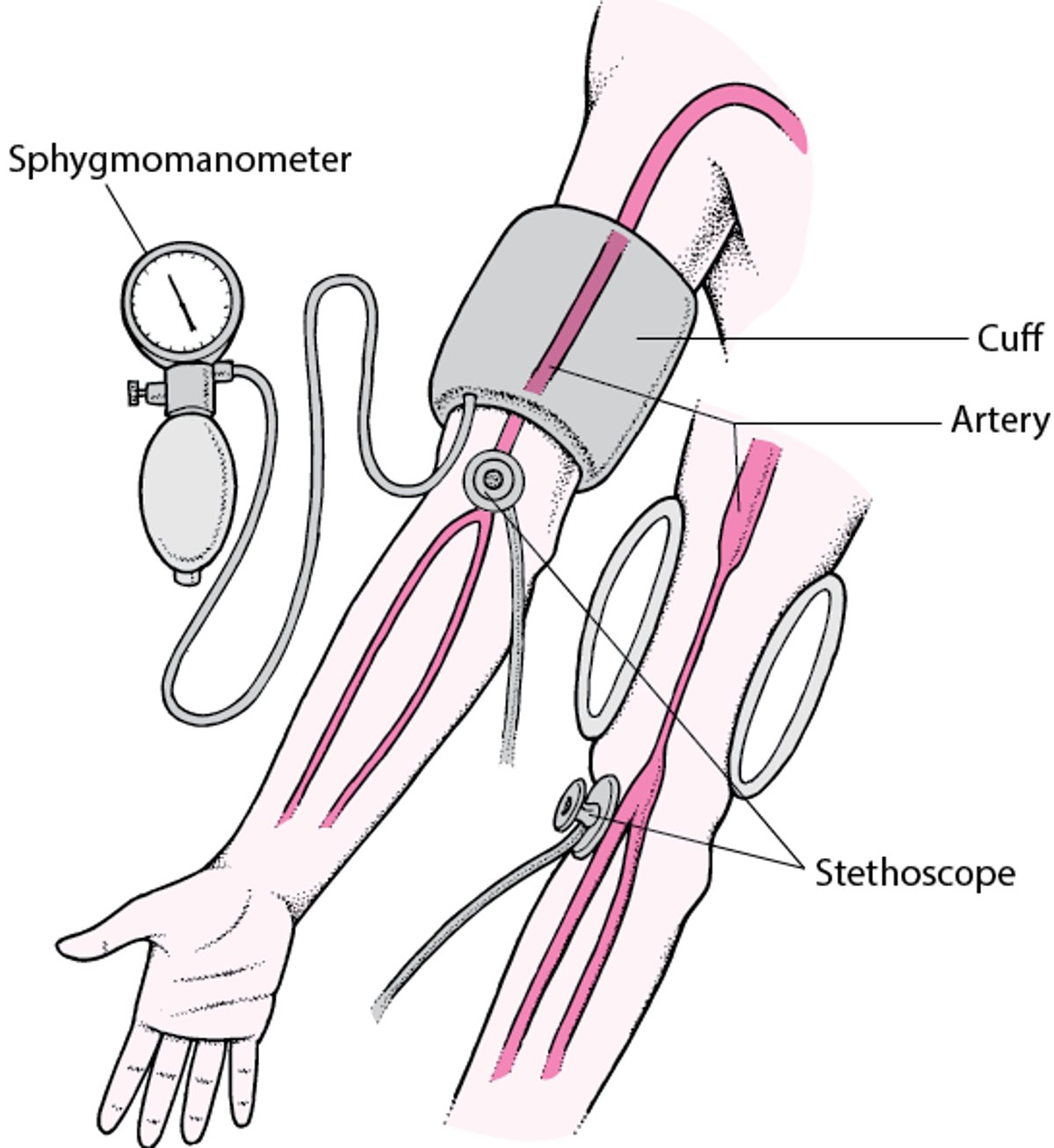
Measuring Blood Pressure
Several instruments can measure blood pressure quickly and with little discomfort. A sphygmomanometer is commonly used. It consists of a soft rubber cuff connected to a rubber bulb that is used to inflate the cuff and a meter that registers the pressure of the cuff. The meter may be a dial, digital meter, or a glass column filled with mercury. Blood pressure is measured in millimeters of mercury (mm Hg) because the first instrument used to measure it was a mercury column. When a sphygmomanometer is used, a person sits with legs uncrossed and back supported. An arm is bared (if a sleeve is rolled up, caution is needed to ensure that it is not tight around the arm), bent, and resting on a table, so that the arm is about the same level as the heart. The cuff is wrapped around the arm. Using a cuff that is proportional to the size of the arm is important. If the cuff is too small, the blood pressure reading is too high. If the cuff is too large, the reading is too low. Listening with a stethoscope placed over the artery below the cuff, a health care professional inflates the cuff by squeezing the bulb until the cuff compresses the artery tightly enough to temporarily stop blood flow, usually to a pressure that is about 30 mm Hg higher than the person's usual systolic pressure (the pressure exerted when the heart beats). Then the cuff is gradually deflated. The pressure at which the professional first hears a pulse in the artery is the systolic pressure. The cuff continues to be deflated, and at some point, the sound of blood flowing stops. The pressure at this point is the diastolic pressure (the pressure exerted when the heart relaxes, between beats). Some instruments can measure blood pressure automatically, without use of a stethoscope or rubber bulb. These devices may fit around the upper arm, finger, or wrist. For people older than 50, blood pressure measured at the upper arm is the most accurate. Sometimes a precise measurement of blood pressure is needed—for example, for a person in an intensive care unit. In such cases, a catheter can be inserted inside an artery to measure blood pressure directly. Instruments to measure blood pressure are available for home use and may be helpful for monitoring blood pressure and response to treatment in people who have high blood pressure. |



JIM VARNEY/SCIENCE PHOTO LIBRARY
If there is still doubt, a 24-hour blood pressure monitor may be used. It is a portable battery-operated device, worn on the hip, connected to a blood pressure cuff, worn on the arm. This monitor repeatedly records blood pressure throughout the day and night over a 24-hour or 48-hour period. The readings determine not only whether high blood pressure is present but also how severe it is.
Pseudohypertension, blood pressure that is measured as high when it is not, occurs in people with very stiff arteries (most commonly, older adults). It occurs when the artery in the arm is too stiff to be compressed by the blood pressure cuff, and as a result, blood pressure cannot be measured accurately.
Masked hypertension occurs when blood pressure is measured as normal when it is high. Masked hypertension affects 10 to 30% of people who have high blood pressure. Recognizing this type of high blood pressure may be impossible unless blood pressure is measured at home or if a complication (for example, heart failure) is suspected to have been caused by high blood pressure.
After high blood pressure has been diagnosed, its effects on key organs, especially the blood vessels, heart, brain, eyes, and kidneys, are usually evaluated. Doctors also look for the cause of high blood pressure. The number and type of tests that are done to look for organ damage and to determine the cause of high blood pressure vary from person to person. In general, routine evaluation for all people with high blood pressure involves a medical history, a physical examination, electrocardiography (ECG), blood tests (including the hematocrit level [the portion of total blood volume made up of red blood cells], potassium and sodium levels, and tests of kidney function), and urine tests.
The physical examination includes checking the area of the abdomen over the kidneys for tenderness and placing a stethoscope over the abdomen to listen for a bruit (the sound caused by blood rushing through a narrowed artery) in the artery supplying each kidney.
The retina in each eye is examined with an ophthalmoscope. The retina is the only place doctors can directly view the effects of high blood pressure on arterioles. The assumption is that the changes in the arterioles of the retina are similar to changes in arterioles and other blood vessels elsewhere in the body, such as in the kidneys. By determining the degree of damage to the retina (hypertensive retinopathy), doctors can classify the severity of high blood pressure.
A stethoscope is used to detect heart sounds. An abnormal heart sound, called the fourth heart sound, is one of the earliest changes in the heart caused by high blood pressure. This sound develops because the left atrium of the heart has to contract harder to fill the enlarged, stiff left ventricle, which pumps blood to all of the body except the lungs.
Electrocardiography (ECG) is usually done to detect changes in the heart—particularly thickening (hypertrophy) of the heart muscle or heart enlargement. If enlargement is suspected, the person may undergo echocardiography.
Kidney damage can be detected by urine and blood tests. Urine tests can detect early evidence of kidney damage. The presence of blood cells and albumin (the most abundant protein in blood) in the urine may indicate such damage. People do not usually develop symptoms of kidney damage (such as lethargy, poor appetite, and fatigue) until much later, when much of kidney function has been lost.
Diagnosis of cause
The higher the blood pressure and the younger the person, the more extensive the search for a cause is likely to be, even though a cause is identified in less than 10% of people. A more extensive evaluation may include x-rays, ultrasound, and other imaging of the kidneys and their blood supply as well as a chest x-ray. Blood and urine tests are done to measure the levels of certain hormones, such as epinephrine, aldosterone, and cortisol.
The cause may be suggested by abnormal results of a physical examination or by the symptoms. For example, a bruit (an abnormal sound doctors hear with a stethoscope) in the artery to a kidney may suggest renal artery stenosis (narrowing of the artery supplying a kidney).
Various combinations of symptoms may suggest high levels of the hormones epinephrine and norepinephrine produced by a pheochromocytoma. The presence of a pheochromocytoma is confirmed when the breakdown products of these hormones are detected in the urine.
Other causes of high blood pressure may be detected by certain routine tests. For example, measuring the potassium level in the blood can help detect hyperaldosteronism.
Treatment of High Blood Pressure
Diet and exercise
Medications to lower blood pressure
Primary hypertension cannot be cured, but it can be controlled to prevent complications. People with elevated blood pressure or any stage of hypertension should change their lifestyle. The decision to prescribe medications is based on the actual blood pressure level and whether people have atherosclerotic cardiovascular disease (ASCVD) or have a more than 10% risk of developing it in the next 10 years.
Treatment for High Blood Pressure
Blood Pressure (mm Hg) | Low Risk of ASCVD* | High Risk of ASCVD* | Presence of ASCVD* |
|---|---|---|---|
Elevated blood pressure (120–129 systolic, less than 80 diastolic) | Lifestyle changes Re-examination in 3–6 months | Lifestyle changes Re-examination in 3–6 months | Lifestyle changes Re-examination in 3–6 months |
Stage 1 high blood pressure ( 130–139 systolic, 80–89 diastolic) | Lifestyle changes Re-examination in 3–6 months | Treatment with 1 blood pressure–lowering medication† Re-examination in 1 month | Treatment with 1 blood pressure–lowering medication† Re-examination in 1 month |
Stage 2 high blood pressure (systolic 140 or higher OR diastolic 90 or higher)‡ | Treatment with 2 blood pressure–lowering medications Re-examination in 1 month | Treatment with 2 blood pressure–lowering medications Re-examination in 1 month | Treatment with 2 blood pressure–lowering medications Re-examination in 1 month |
* ASCVD = atherosclerotic cardiovascular disease, including coronary artery disease, heart failure, or stroke. Low risk is considered less than 10%. High risk is 10% or more. | |||
† Lifestyle changes are recommended for all people receiving medication therapy. | |||
‡ For people with blood pressure readings of 140–159/90–100, doctors prescribe 2 medications (of different classes) for the initial treatment, and they re-examine the person frequently. | |||


IAN HOOTON/SCIENCE PHOTO LIBRARY
Doctors often recommend that people with high blood pressure monitor their own blood pressure at home. Self-monitoring probably helps motivate people to follow a doctor's recommendations regarding treatment.
Treatment goals
The goal for antihypertensive therapy is to decrease blood pressure to below 130/80 mm Hg in most people. However, if decreasing a person's blood pressure to less than 130/80 mm Hg causes symptoms, such as fainting, light headedness, memory loss, or dizziness, doctors may recommend a higher blood pressure goal but not higher than 140/90. For some people, for example, those at high risk of heart disease, a lower systolic goal may be appropriate.
Lifestyle changes
Lifestyle changes are important for all people with hypertension.
People who are overweight and have high blood pressure are advised to lose weight. Losing as few as 10 pounds (4.5 kilograms) can lower blood pressure. For people who have obesity, diabetes, or high cholesterol levels, changes in diet (to one that is rich in fruits, vegetables, and low-fat dairy products, with reduced saturated and total fat content) are important for reducing the risk of heart and blood vessel disease.
People who smoke should stop smoking.
Limiting the intake of alcohol and sodium (while maintaining an adequate intake of calcium, magnesium, and potassium) may make medication therapy for high blood pressure unnecessary. Alcohol intake should be no more than 2 drinks (a daily total of 24 ounces [about 1 liter] of beer, 8 ounces [about 240 milliliters] of wine, or 2 ounces [about 60 milliliters] of 100-proof whiskey or other liquor) in men and 1 drink in women. Daily sodium intake should ideally be reduced to less than 1500 milligrams, or less than 3.75 grams of sodium chloride (salt) intake.
Moderate aerobic exercise is helpful. Most people with hypertension do not have to restrict their physical activity as long as their blood pressure is controlled. Regular exercise helps reduce blood pressure and weight and improves the functioning of the heart and overall health (see Benefits of Exercise).
People should get adequate sleep. Getting a minimum of 6 hours of sleep per night may help people maintain control of their blood pressure.
Medications
(See also Medications for High Blood Pressure.)
Medications that are used in the treatment of high blood pressure are called antihypertensives. With the wide variety of antihypertensives available, high blood pressure can be controlled in almost anyone, but treatment has to be tailored to the individual. Treatment is most effective when the person and doctor communicate well and collaborate on the treatment program.
Different types of antihypertensives reduce blood pressure by different mechanisms, so many different treatment strategies are possible. For some people, doctors use a stepped approach to medication therapy: They start with one type of antihypertensive and add others as necessary. For other people, doctors find a sequential approach is preferable: They prescribe one antihypertensive, and if it is ineffective, they stop it and prescribe another type. For people with blood pressure at or above 140/90 mm Hg, usually 2 medications are started at the same time. In choosing an antihypertensive, doctors consider such factors as
The person's age, sex, and sometimes ethnicity
The severity of high blood pressure
The presence of other conditions, such as diabetes or high blood cholesterol levels
Potential side effects, which vary depending on the medication
The costs of the medications and of tests needed to check for certain side effects
Many people require 2 or more medications to reach their blood pressure goal.
Most people tolerate their prescribed antihypertensive medications without problems. But any antihypertensive medication can cause side effects. So if side effects develop, a person should tell the doctor, who can adjust the dose or substitute another medication. Usually, antihypertensive medication must be taken indefinitely to control blood pressure.
Treatment of secondary hypertension
The cause of the high blood pressure is treated if possible. Treating kidney disease can sometimes return blood pressure to normal or at least lower it, so that antihypertensive therapy is more effective. A narrowed artery to the kidney may be widened by inserting a balloon-tipped catheter and inflating the balloon (angioplasty). Or the narrowed part of the artery supplying the kidney can be bypassed. Often the high blood pressure resolves after such surgery. Tumors that cause high blood pressure, such as a pheochromocytoma, usually can be removed surgically.
Treatment of resistant hypertension
Resistant hypertension is blood pressure that is not controlled despite taking 3 medications of different classes adequate doses. Four drugs may be required for some patients.
Two interventional treatments for managing people with resistant hypertension are available in some countries outside the United States. However, these treatments are not available in the United States where they are considered experimental. In one (renal artery sympathetic nerve ablation), a radiofrequency catheter is inserted into the artery to each kidney to damage the sympathetic nerves.along the renal arteries. Another treatment (pacemaker therapy or baroreflex activation therapy) involves implanting an electrode in the neck, where it stimulates certain nerve endings that help regulate blood pressure. The longterm effects of these treatments are not known.
Treatment of hypertensive urgencies and emergencies
In hypertensive emergencies, blood pressure must be lowered rapidly. Hypertensive emergencies are treated in hospital intensive care units. Most medications used to rapidly lower blood pressure, such as fenoldopam, nitroprusside, nicardipine, or labetalol, are given intravenously.In hypertensive emergencies, blood pressure must be lowered rapidly. Hypertensive emergencies are treated in hospital intensive care units. Most medications used to rapidly lower blood pressure, such as fenoldopam, nitroprusside, nicardipine, or labetalol, are given intravenously.
Prognosis for High Blood Pressure
Untreated high blood pressure increases a person's risk of developing heart disease (such as heart failure, heart attack, or sudden cardiac death), kidney failure, or stroke at an early age. High blood pressure is the most important risk factor for stroke. It is also one of the 3 most important risk factors for heart attack that a person can modify (the other 2 are smoking and high cholesterol levels in the blood).
Treatment that lowers high blood pressure greatly decreases the risk of stroke and heart failure. Such treatment may also decrease the risk of a heart attack, although not as dramatically.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association: High blood pressure: Comprehensive resource to help people understand causes of high blood pressure and manage the lifestyle changes required for treatment







