



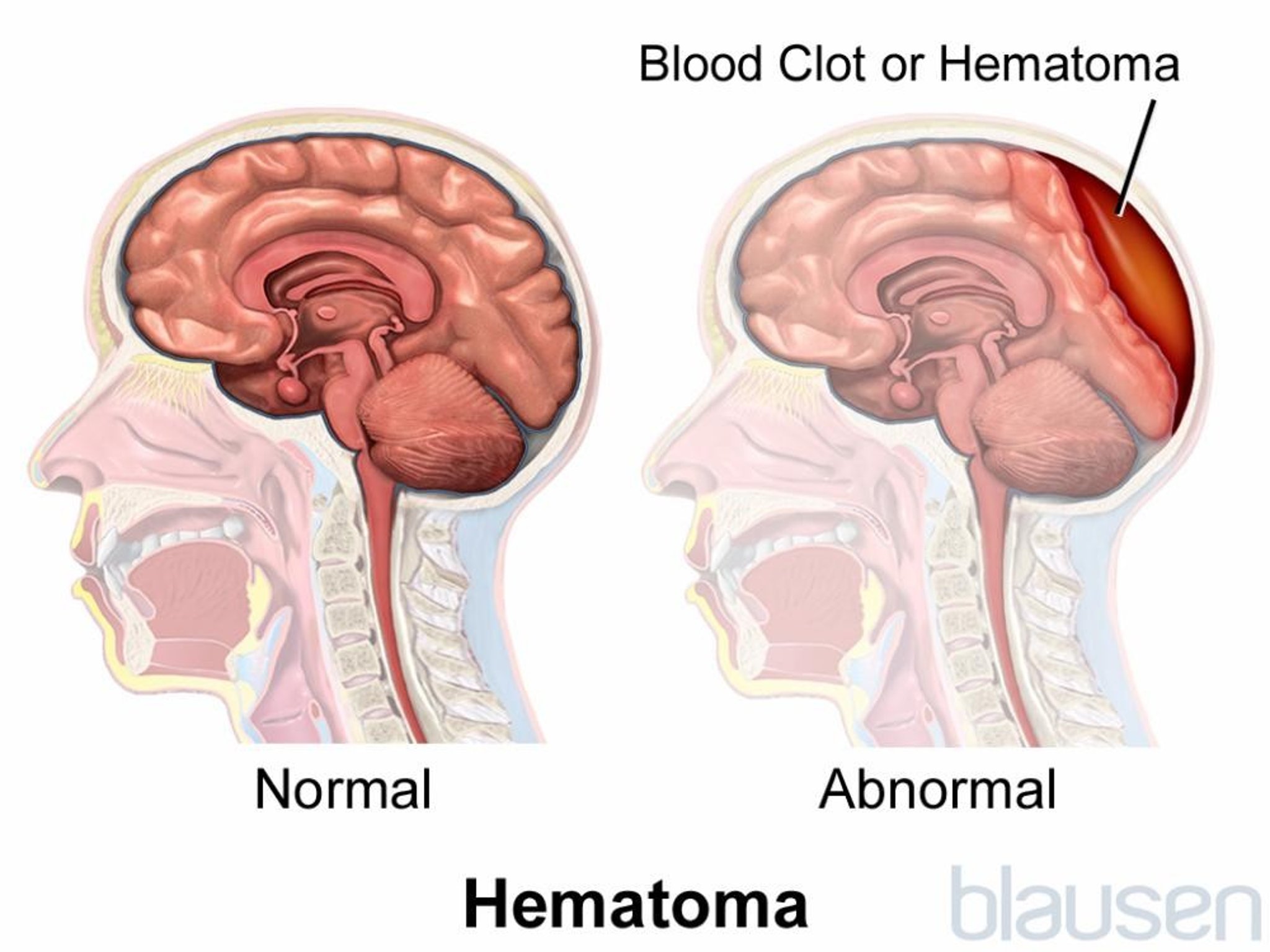
Intracranial hematomas are accumulations of blood inside the skull, either within the brain or between the brain and the skull.



Intracranial hematomas form when a head injury causes blood to accumulate within the brain or between the brain and the skull.
Symptoms may include a persistent headache, drowsiness, confusion, memory changes, paralysis on the opposite side of the body, speech or language impairment, and other symptoms depending on which area of the brain is damaged.
Computed tomography or magnetic resonance imaging is used to detect an intracranial hematoma.
Sometimes surgery is needed to drain blood from a hematoma.
Intracranial hematomas usually result from a head injury but sometimes result from spontaneous bleeding. There are several types of intracranial hematoma, including
Epidural hematomas, which form between the skull and the outer layer (dura mater) of tissue covering the brain (meninges)
Subdural hematomas, which form between the outer layer and the middle layer (arachnoid mater—see figure Viewing the Brain)
Intracerebral hematomas, which form within the brain
(See also Overview of Head Injuries.)
After injury, bleeding can also occur between the arachnoid mater and the inner layer (pia mater). (See Tissues Covering the Brain.) Bleeding in this area is called subarachnoid hemorrhage. However, because subarachnoid blood usually does not accumulate in 1 place, it is not considered a hematoma.

For people who are taking aspirin or anticoagulants (which increase the risk of bleeding), particularly older adults, the risk of developing a hematoma after even a minor head injury is increased. For people who are taking aspirin or anticoagulants (which increase the risk of bleeding), particularly older adults, the risk of developing a hematoma after even a minor head injury is increased.Intracerebral hematomas and subarachnoid hemorrhages can also result from strokes.
Most epidural and intracerebral hematomas and many subdural hematomas develop rapidly and cause symptoms within minutes. Large hematomas press on the brain and may cause swelling and herniation of the brain. Herniation may cause loss of consciousness, coma, paralysis on one or both sides of the body, breathing difficulties, slowing of the heart, and even death.
Some hematomas, particularly subdural hematomas, may develop slowly and cause gradual confusion and memory loss, especially in older adults. These symptoms are similar to those of dementia. People may not remember the head injury.
Diagnosis of intracranial hematomas is usually based on results of computed tomography (CT).
Treatment of intracranial hematomas depends on the type and size of the hematoma and how much pressure has built up in the brain.
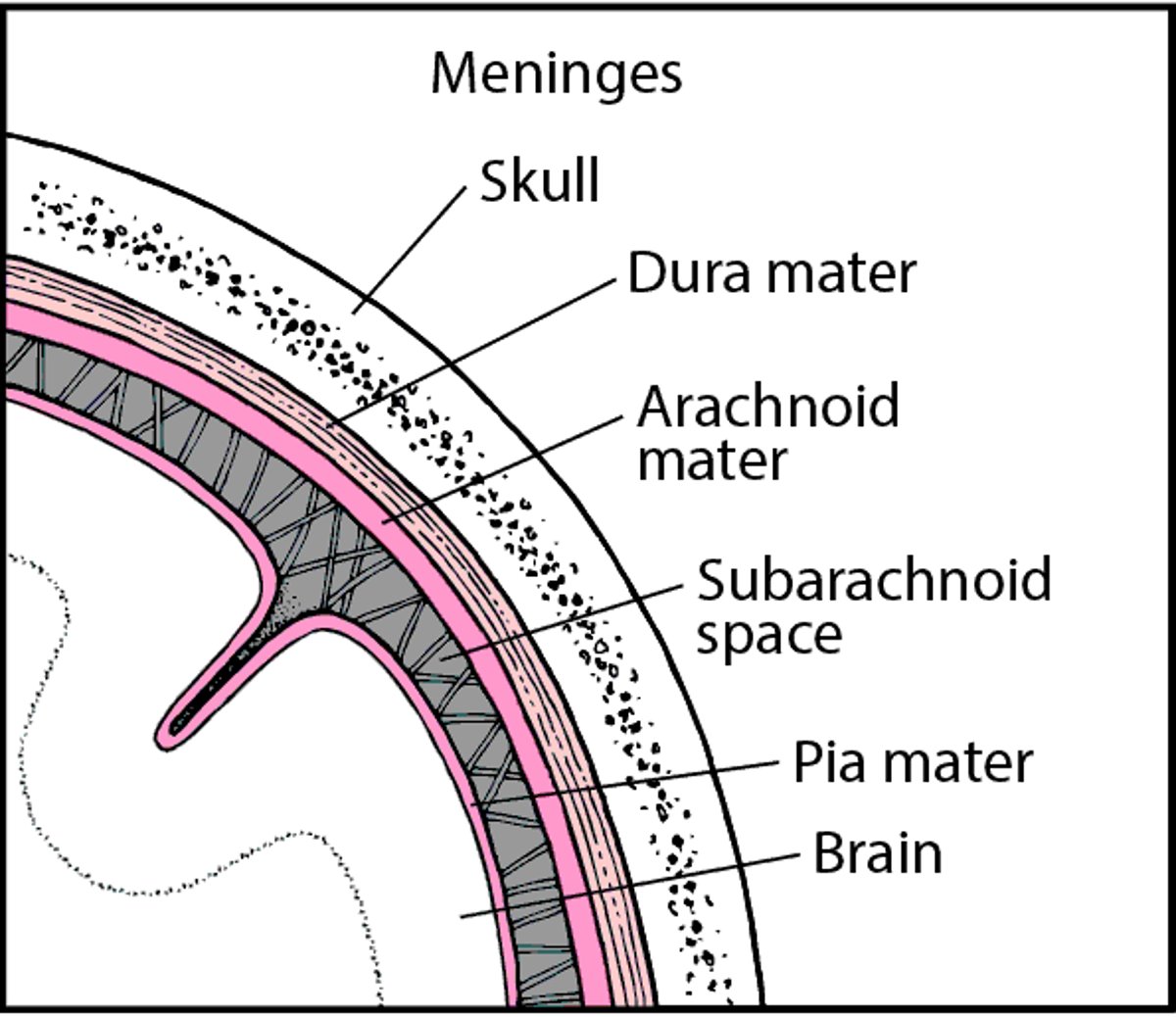
Tissues Covering the Brain
Within the skull, the brain is covered by 3 layers of tissue called the meninges:
Between the arachnoid membrane and pia mater is the subarachnoid space. This space contains cerebrospinal fluid, which flows through the meninges, fills the spaces within the brain, and helps cushion the brain and spinal cord. |

Epidural Hematomas
Epidural hematomas are caused by bleeding from an artery or a large vein (venous sinus) located between the skull and the outer layer of tissue covering the brain. Bleeding often occurs when a skull fracture tears the blood vessel.
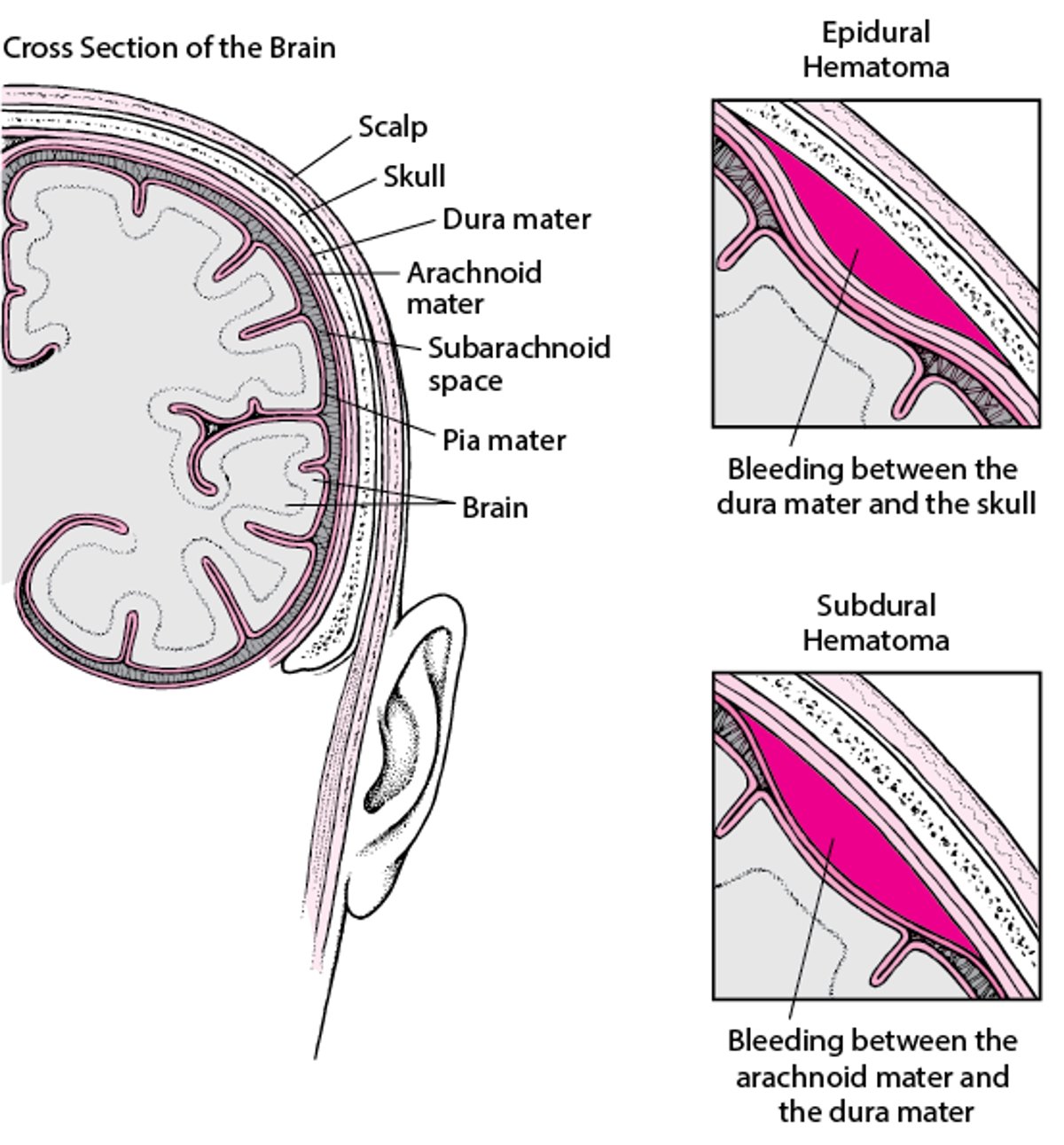
Pockets of Blood in the Brain
A head injury can cause bleeding in the brain. It can result in a pocket of blood between the skull and the outer layer of tissue covering the brain. This pocket of blood is called an epidural hematoma. Or a pocket of blood may form between the outer and middle layers of tissue. This pocket of blood is called a subdural hematoma. |

A severe headache may develop immediately or several hours after the injury. The headache sometimes disappears but returns several hours later, worse than before. Deterioration in consciousness, including increasing confusion, sleepiness, and a deep coma, can quickly follow. Some people lose consciousness after the injury, regain it, and have a period of unimpaired mental function (lucid interval) before consciousness deteriorates again. People may develop paralysis on the side of the body opposite the hematoma, speech or language impairment, or other symptoms, depending on the location of the brain damage.
Early diagnosis of epidural hematomas is crucial and is usually based on results of computed tomography (CT).
Doctors treat epidural hematomas as soon as they are diagnosed. Prompt treatment is necessary to prevent permanent damage. Usually, 1 or more holes are drilled in the skull to drain the excess blood. The surgeon also seeks the source of the bleeding and stops the bleeding.
Subdural Hematomas
Subdural hematomas are usually caused by bleeding from veins, including the bridging veins, located between the outer and middle layers of tissue covering the brain (meninges). Occasionally, subdural hematomas are caused by bleeding from arteries.
Subdural hematomas may be
Acute: Symptoms develop over minutes or a few hours after the injury.
Subacute: Symptoms develop over several hours or days.
Chronic: Symptoms develop gradually over weeks, months, or years.
Acute or subacute subdural hematomas may be caused by rapid bleeding after a severe head injury. Acute subdural hematomas are often caused by a head injury that occurs during a fall or motor vehicle crash. They may also develop in people who have bruising in the brain (contusions) or an epidural hematoma.
Acute subdural hematomas can cause swelling in the brain. The hematoma and swelling can result in increased pressure within the skull (intracranial pressure), which can make symptoms worse and increase the risk of dying.
Chronic subdural hematomas are more common among people with alcohol use disorder, older adults, and people who take medications that make blood less likely to clot (anticoagulants or antiplatelets). People with alcohol use disorder and older adults, who are relatively prone to falls as well as bleeding, may ignore or forget minor to moderately severe head injuries. These injuries can lead to small subdural hematomas that may become chronic.
By the time symptoms are noticeable, a chronic subdural hematoma may be very large. Chronic hematomas are less likely than acute hematomas to cause a rapid increase of pressure within the skull.
In older adults, the brain shrinks slightly, stretching the bridging veins and making them more likely to be torn if an injury, even a minor one, occurs. Also, bleeding tends to continue longer because the shrunken brain exerts less pressure on the bleeding vein, allowing more blood loss from it.
Blood that remains after a subdural hematoma is slowly reabsorbed. After the blood is resorbed from a hematoma, the brain may not re-expand as well in older adults as in younger people. As a result, a fluid-filled space (hygroma) may be left. The hygroma may refill with blood or enlarge because small vessels tear, causing repeated bleeding.
Did You Know...
|
Symptoms of Subdural Hematomas
Symptoms of a subdural hematoma may include a persistent headache, fluctuating drowsiness, confusion, memory changes, paralysis on the side of the body opposite the hematoma, and speech or language impairment. Other symptoms may occur depending on the location of the brain damage.
In infants, a subdural hematoma can cause the head to enlarge (as in hydrocephalus) because the skull is soft and pliable. Therefore, pressure within the skull increases less in infants than it does in older children and adults.
Diagnosis of Subdural Hematomas
Computed tomography or magnetic resonance imaging
Chronic subdural hematomas are more difficult to diagnose because of the length of time between the injury and the development of symptoms. An older adult with gradually developing symptoms, such as memory impairment and drowsiness, may be mistakenly thought to have dementia.
Computed tomography (CT) can detect acute, subacute, and many chronic subdural hematomas. Magnetic resonance imaging (MRI) is particularly accurate for diagnosis of chronic subdural hematomas.
Treatment of Subdural Hematomas
For small hematomas, often no treatment
For large hematomas, surgery to drain them
Often, small subdural hematomas in adults do not require treatment because the blood is absorbed on its own.
If a subdural hematoma is large and is causing symptoms such as persistent headache, fluctuating drowsiness, confusion, memory changes, and paralysis on the opposite side of the body, doctors usually drain it surgically, sometimes by drilling a small hole in the skull. However, sometimes a larger opening must be made in the skull—for example, when bleeding has occurred very recently or when the blood may be too thick to drain through a small hole. During surgery, a drain is usually inserted and left in place for several days because subdural hematomas can recur. The person is monitored closely for recurrences.
In infants, doctors usually drain the hematoma for cosmetic if for no other reasons.
About half of people who are treated for a large acute subdural hematoma survive. People who are treated for a chronic subdural hematoma usually improve or do not worsen.
Intracerebral Hematomas
Intracerebral hematomas are common after a severe head injury. They can be caused by bruising of the brain (a cerebral contusion). Exactly when 1 or more contusions become a hematoma is not well-defined.
People may develop drowsiness, confusion, paralysis on the side of the body opposite the hematoma, speech or language impairment, or other symptoms, depending on the location of the brain damage.
Fluid accumulation in the damaged brain (cerebral edema) is common. It increases pressure within the skull (intracranial pressure). When pressure within the skull is increased, the brain may get less blood and oxygen. If the pressure is high enough, the brain may be forced through a small natural opening in the relatively rigid sheets of tissue that separate the brain into compartments (brain herniation). Cerebral edema and its complications account for most deaths.
Computed tomography (CT) or magnetic resonance imaging (MRI) can detect intracerebral hematomas.
Surgery is usually avoided because of the following:
Intracerebral hematomas are caused by direct damage to the brain.
Usually, surgery does not restore brain function.
Hematomas are within the brain tissue. Thus, doctors must remove the overlying brain to get at the hematoma. Removing this tissue contributes to loss of brain function.







