


Sometimes clinicians s recommend screening tests as part of preventive care, which are tests that are done to look for disorders in people who have no symptoms. If women have symptoms related to the reproductive system (gynecologic symptoms), tests to identify the disorder causing them (diagnostic procedures) may need to be done.
Important screening tests for women include
Cervical cancer screening tests: Papanicolaou (Pap) test and/or a human papillomavirus (HPV) test to check for precancer or cancer of the cervix (the lower part of the uterus)
Mammography to check for breast cancer
Tests for sexually transmitted infections (such as chlamydia or gonorrhea) in at-risk women
Pregnancy Testing
Women who are of childbearing age and are trying to become pregnant, are concerned about an unintended pregnancy, or have gynecologic symptoms may ask to be tested for pregnancy or a clinician may recommend a pregnancy test. Clinicians take a sample of urine or sometimes blood from and test it to determine whether a woman is pregnant.
The accuracy of home urine pregnancy tests can vary depending upon the specific test kit, technique, and interpretation. Thus, any positive home pregnancy test should be confirmed by either a laboratory urine or blood test.
Other Laboratory Tests
Clinicians may do other blood tests to evaluate for gynecologic disorders or complications, including
Hormonal blood tests to evaluate fertility or test for causes of abnormal uterine bleeding (such as thyroid disorders, polycystic ovary syndrome, or menopause)
Red blood cell count to check for anemia in women with heavy uterine bleeding (potential causes include hormonal disorders, uterine fibroids, or uterine adenomyosis)
Platelet count or blood clotting tests for women with heavy bleeding and a possible blood clotting disorder
In additions, sometimes a urine sample is collected to test for urinary tract infection, sexually transmitted infections, or bladder or kidney abnormalities.
Testing for Gynecologic Infections
Testing for vaginitis
For women with abnormal vaginal discharge, clinicians may take a sample of the discharge to test for vaginitis, which can be caused by bacterial vaginosis, yeast infection, or trichomonas infection. Some test results are available immediately, and others take a few days.
Testing for sexually transmitted infections
Women at risk of sexually transmitted infections (STIs) should be screened for these diseases, even if they have no symptoms.
Women should be tested regularly for STIs, depending on risk. Testing should be done every year for gonorrhea and chlamydia in women who are
Sexually active and age 25 or younger
Sexually active and older than 25 if there is increased risk (such as a new or multiple sex partner, a woman or her partner have more than one sex partner or have had a previous STI)
Pregnancy
Testing at least once in a woman's lifetime for HIV and hepatitis C (or more often if the woman is at increased risk) is also recommended.
Pregnant women should be tested for HIV, hepatitis B, and syphilis.
Women at high risk, with symptoms, or who request testing should also be tested at any time for STIs. Testing for STIs is done with different types of tests, depending on the infection.
STIs that are tested for with vaginal, cervical, or urinary specimens are
For most of these STIs, the clinician uses a swab to obtain a small sample from the cervix. The sample is sent to a laboratory for analysis. Testing for gonorrhea and chlamydia can also be done using a urine specimen or a sample from inside the vagina (which can be collected by a clinician or by the woman herself).
STIs that are tested for with blood tests are:
STI testing is an important part of preventive care, because untreated STIs can cause serious complications (such as, infertility, severe diseases of the liver, nervous system, or immune system, or cancer).
Although HPV is an STI, HPV testing is usually done as part of cervical cancer screening, alone or combined with a Pap test, not as an STI test. HPV can cause genital warts and increases the risk of cervical cancer. Genital warts are diagnosed by clinicians during the pelvic examination, based on their appearance. Sometimes, if the diagnosis is uncertain, biopsy is required.
Cervical Cancer Testing
Screening for cervical cancer
Tests used to screen for cervical cancer include the following:
Papanicolaou (Pap) test: Cells from the cervix are examined under a microscope to determine whether any are cancerous or abnormal and may, without treatment, progress to cancer (precancerous cells).
Human papillomavirus (HPV) test: A sample from the cervix is tested to determine whether HPV is present. HPV can lead to cervical cancer.
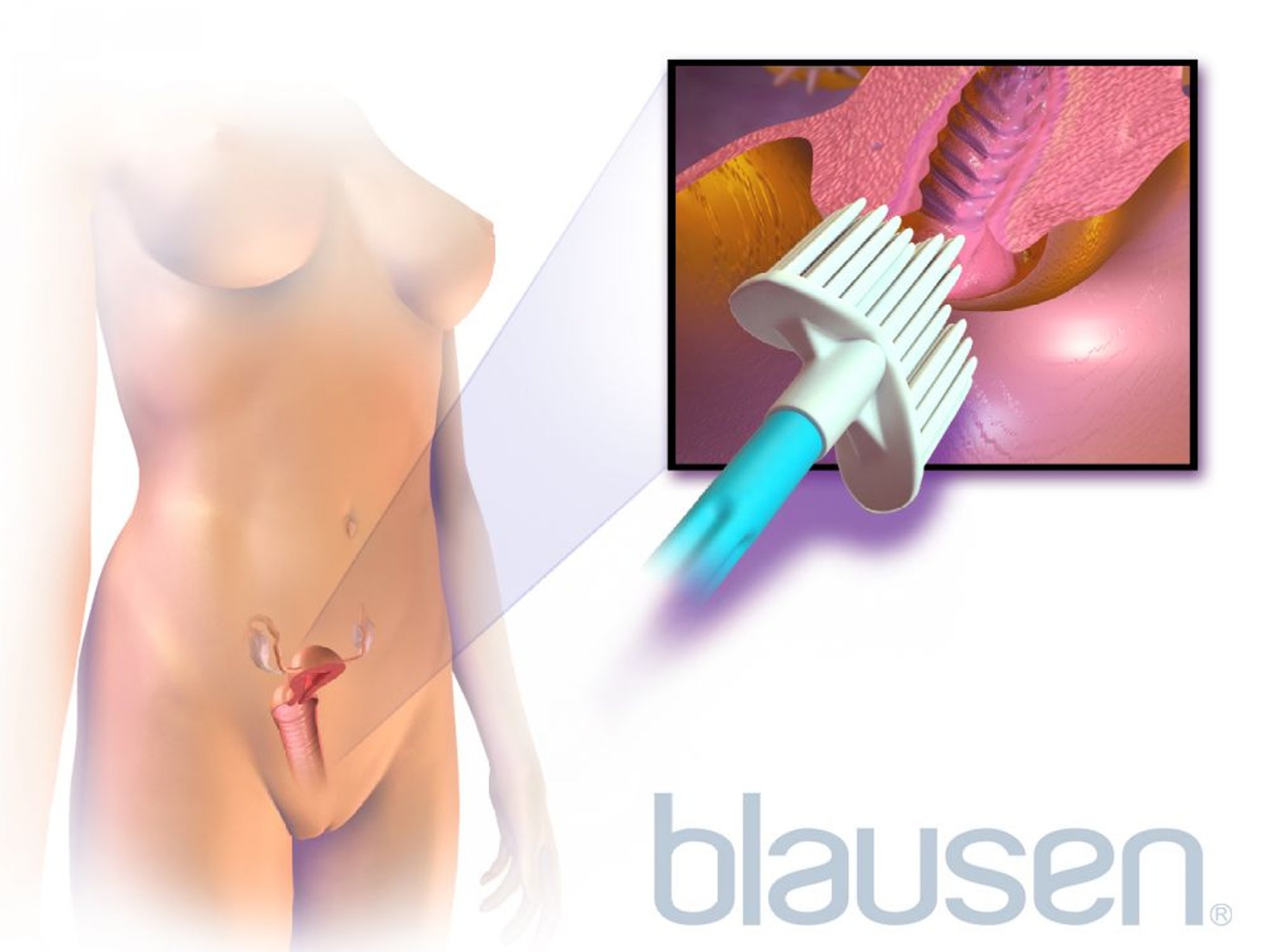
In both the Pap test and HPV test, clinicians collect a sample from the cervix. Clinicians collect the sample by inserting a speculum (a metal or plastic instrument) into the vagina to hold open the walls of the vagina. They then use a plastic brush to remove some cells from the surface of the cervix and from the passageway through the cervix (cervical canal). The samples are sent to a laboratory, where they are examined under a microscope to look for abnormal cells. Abnormal cells may indicate precancerous changes or, rarely, cervical cancer.

Usually, having a Pap test done feels scratchy or crampy, but it is not painful and takes only a few seconds.

Pap tests identify most cervical cancers, even very early-stage cancer. They can also detect precancerous changes in cervical cells. These changes, called cervical intraepithelial neoplasia (CIN), can be treated, thus helping prevent cancer from progressing and spreading.
Pap tests are most accurate if a woman does not douche or use vaginal creams or other products for at least 24 hours before the test.
Experts recommend that the first Pap test be done in most women after the age of 21 years.
How often testing is needed depends mainly on a woman’s age and the results of previous Pap tests:
Under age 21: Screening not needed
From age 21 to 29: Testing is usually done every 3 years using a Pap test alone (alternatively, average-risk patients 25 years and older may begin screening with primary HPV testing alone every 5 years)
From age 30 to 65: Testing is done every 3 years if only a Pap test is done, or every 5 years if an HPV test alone is done, or every 5 years if a Pap test and a test for HPV are done.
After age 65: Most women no longer need to be tested if they have had no abnormal test result in the last 10 years.
Women with a high risk of cervical cancer need to be tested more frequently. Such women include those who have an HIV infection, who have a weakened immune system (which may result from taking a medication or having a disorder that suppresses the immune system), or who have had abnormal Pap test results.
Pap tests in older women may be resumed or continued if a woman has a new sex partner or if she has several sex partners.
Women who have had their uterus completely removed (total hysterectomy) and have not had any abnormal Pap test results do not need to be screened for cervical cancer. However, if the hysterectomy is not total (that is, the cervix is left in place), screening is needed. (The cervix is the lower part of the uterus that opens into the vagina.)
Abnormal results of cervical cancer screening tests require further evaluation.
Cervical diagnostic and treatment procedures
Colposcopy
For colposcopy, a speculum is used to hold open the walls of the vagina and a binocular magnifying lens (similar to that of a microscope) is used to inspect the cervix for signs of cancer. Often, a sample of tissue is removed for examination under a microscope (biopsy).
Colposcopy is often done when
Cervical, vaginal, or vulvar lesions require evaluation.
Results of a Papanicolaou (Pap) test are abnormal, with or without positive HPV test.
A woman has completed treatment for cervical cancer.
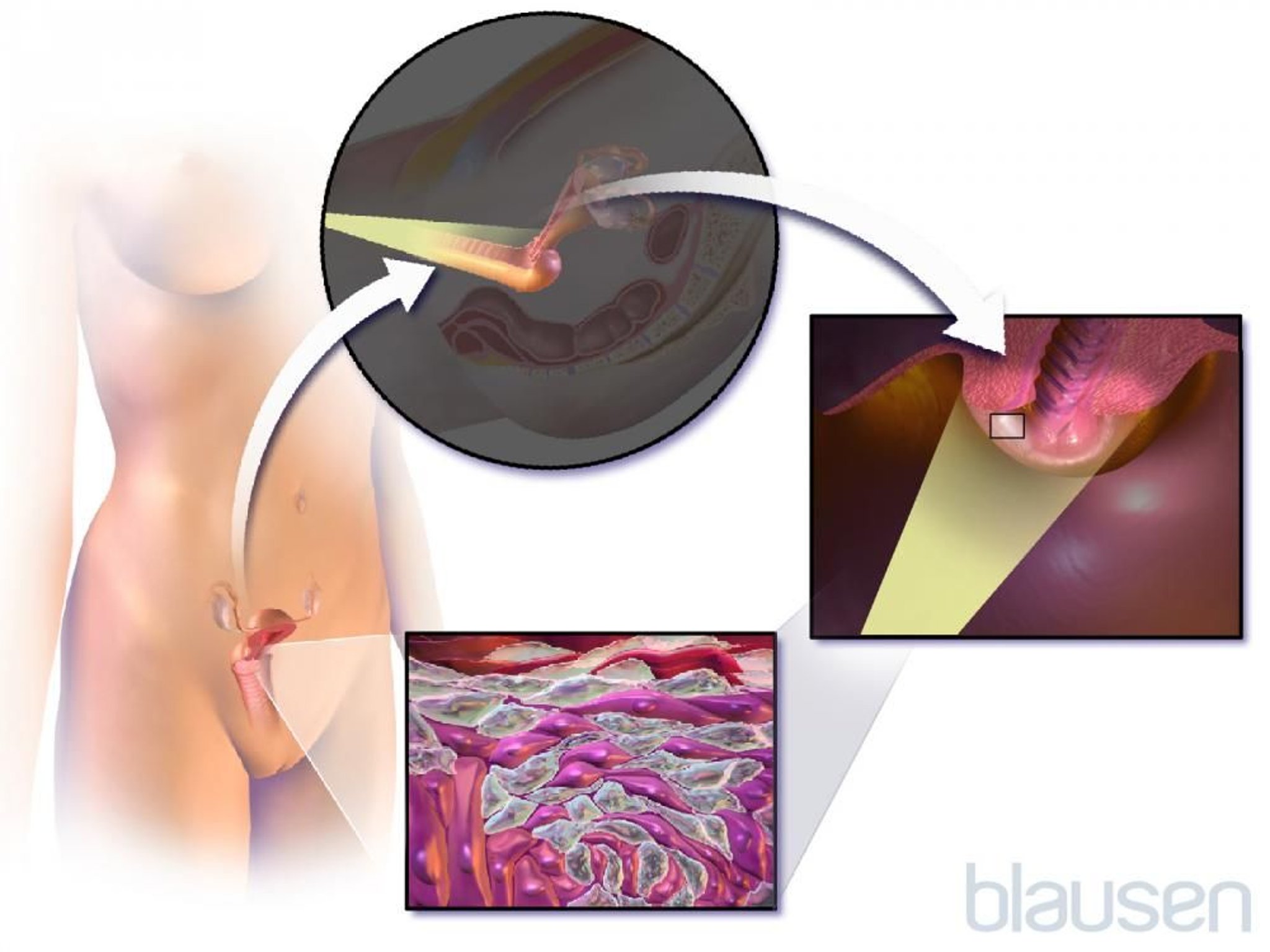
Women usually feel some discomfort when the speculum is inserted, but colposcopy alone (without biopsy) is painless and thus requires no anesthetic. The biopsy procedure is typically described as causing a crampy or sharp pinching sensation and also does not require an anesthetic. The procedure usually takes 10 to 15 minutes. Minimal spotting is common after the procedure.
Endocervical curettage
Endocervical curettage consists of inserting a small, sharp, scoop-shaped instrument (curet) into the passageway through the cervix (cervical canal) to obtain tissue. The curet is used to scrape a small amount of tissue from high inside the cervical canal. A cervical biopsy (to remove a smaller piece of tissue from the surface of the cervix) is typically done at the same time. The tissue samples are examined under a microscope by a pathologist.
Endocervical curettage is done when
Endometrial or cervical cancer is suspected or needs to be ruled out.
Usually, it is done during colposcopy and does not require an anesthetic.
Loop electrical excision procedure
In a loop electrical excision procedure (LEEP), a thin wire loop that conducts an electrical current is used to remove a piece of tissue. Typically, this piece of tissue is larger than that obtained in a biopsy of the cervix.
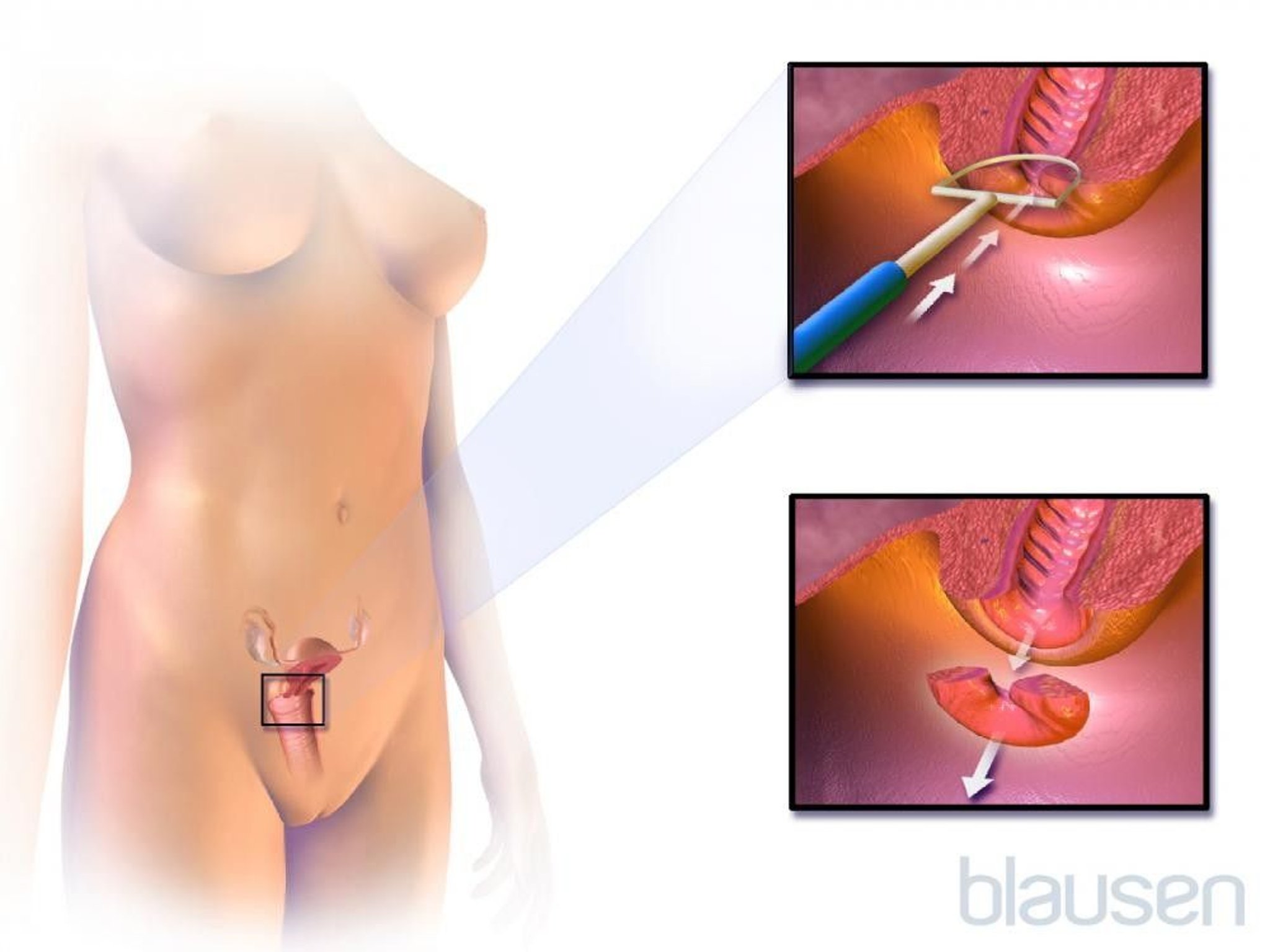
This procedure may be done after an abnormal Pap test result
To evaluate the abnormality more accurately
To remove the abnormal tissue (and thus treat early-stage cervical cancer)
Gynecologic Biopsies
A biopsy consists of removing a small sample of tissue for examination under a microscope. Biopsy of the vulva, vagina, cervix, or lining of the uterus can be done.
Cervix or vagina
A cervical biopsy is done when
A Pap test result showed a condition that could lead to cancer (precancerous condition) or cancer is suspected.
A clinician sees an abnormality during the pelvic examination.
A biopsy of the cervix or vagina is usually done during colposcopy. During colposcopy, clinicians can identify the area that looks most abnormal and take tissue samples from it.
Vulva
A biopsy of the vulva (the area around the opening of the vagina) is done when
A diagnosis cannot be made based on a woman’s symptoms and results of a physical examination.
Cancer of the vulva is suspected.
Biopsy of the vulva can usually be done in the doctor's office and requires use of a local anesthetic. If cancer or precancer caused by HPV is suspected, a colposcope is sometimes used to view the abnormal area and guide the biopsy.
Uterus
A biopsy of the lining of the uterus (endometrial biopsy) is usually done to
Determine the cause of abnormal vaginal bleeding
Check for cancer of the lining of the uterus (endometrial cancer) when this cancer is suspected
Also, infertility specialists use this procedure to determine whether ovulation is occurring normally and whether the uterus is ready for implantation of embryos as part of in vitro fertilization.
For an endometrial biopsy (endometrial aspiration), a speculum is used to hold open the walls of the vagina, and, after cleaning the cervix with antiseptic solution, a small plastic tube (3 mm wide) is inserted through the cervix into the uterus. The tube is used to suction tissue from the uterine lining.
Gynecologic Imaging Studies
Ultrasonography
Ultrasonography (sonography) uses ultrasound waves, produced at a frequency too high to be heard. The ultrasound waves are emitted by a handheld device that is placed on the abdomen (called abdominal ultrasonography) or inside the vagina (called transvaginal ultrasonography). The waves reflect off internal structures, and the pattern of this reflection can be displayed on a monitor.

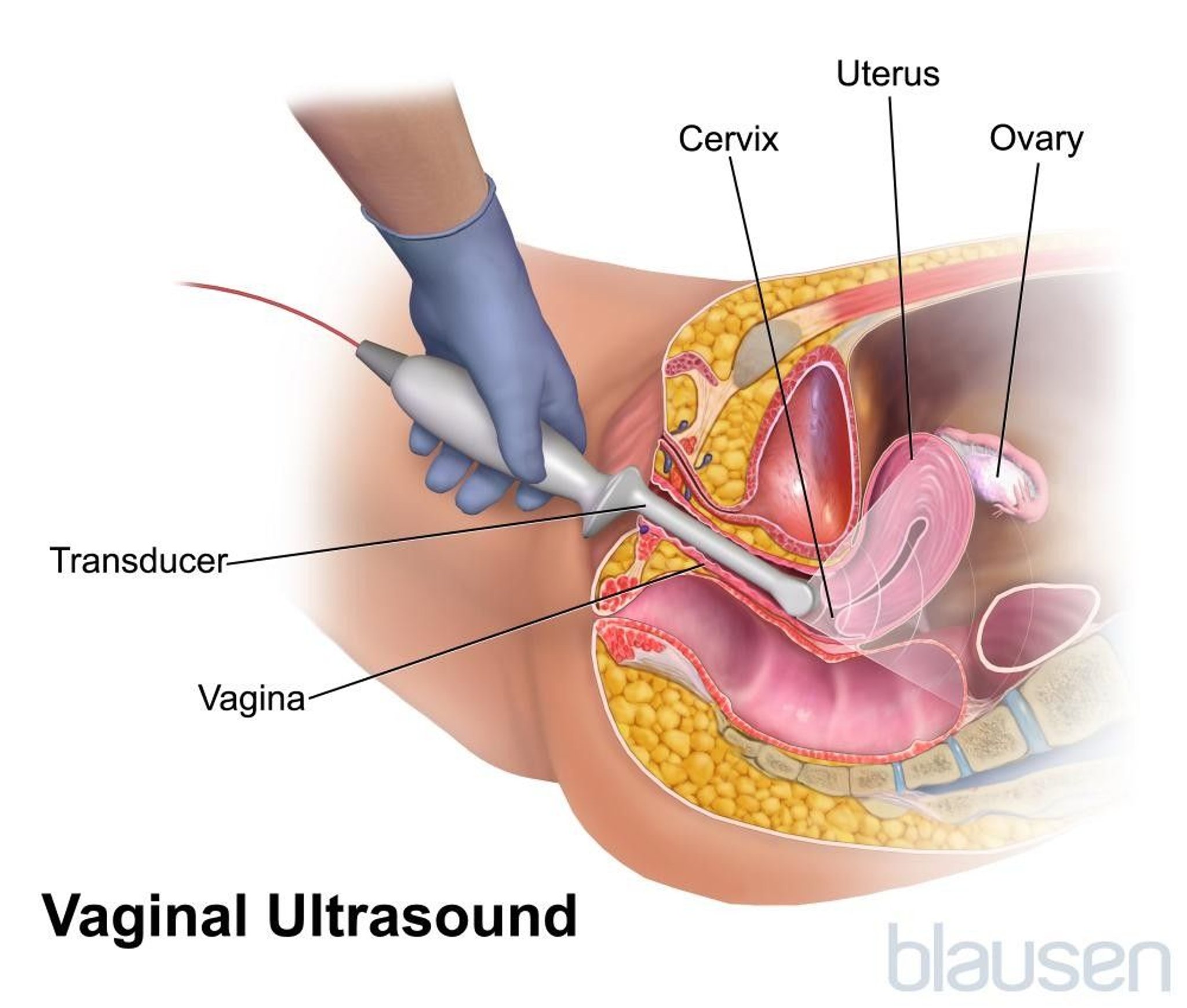
Transvaginal ultrasonography is mostly used to detect the following:
Tumors, cysts, and other abnormalities in the internal reproductive organs (ovaries, fallopian tubes, uterus, and vagina)
Transvaginal ultrasound can also be used to guide a doctor during certain procedures (dilation and curettage, placement of an intrauterine device).
Transabdominal and transvaginal ultrasonography may be done during pregnancy for the following reasons:
To evaluate the condition, size and growth, and anatomy of the fetus
To evaluate the location, condition, and blood flow of the placenta
To guide the placement of instruments during amniocentesis or chorionic villus sampling
Ultrasonography is painless and has no known risks for either mother or fetus.
Magnetic resonance imaging (MRI) or computed tomography (CT) scan
If evaluation with ultrasonography is not adequate, MRI (which is very good at detecting pelvic abnormalities but is expensive) may be used. CT is usually less desirable because it is somewhat less accurate for gynecologic disorders, involves significant radiation exposure, and often requires injection of a contrast agent. CT is mainly used for evaluation of gynecologic cancers that may have spread.
Saline sonography
For saline sonography (sonohysterography), fluid is placed in the uterus through a thin tube (catheter) that is inserted through the vagina and then the cervix. Then ultrasonography is done. The fluid fills and stretches (distends) the uterus so that abnormalities inside the uterus, such as polyps or fibroids, can be more easily detected.
Hysterosalpingography
For hysterosalpingography, x-rays are taken after a radiopaque contrast agent, which can be seen on x-rays, is injected through the cervix to outline the interior of the uterus and fallopian tubes.
Hysterosalpingography is often used to do the following:
To help determine the cause of infertility
To confirm that a sterilization procedure to block the tubes is successful
The procedure is done in a place where x-rays can be taken, such as a hospital or the radiology suite of a doctor's office.
Diagnostic Procedures
Occasionally, more extensive diagnostic procedures are needed.
Dilation and curettage
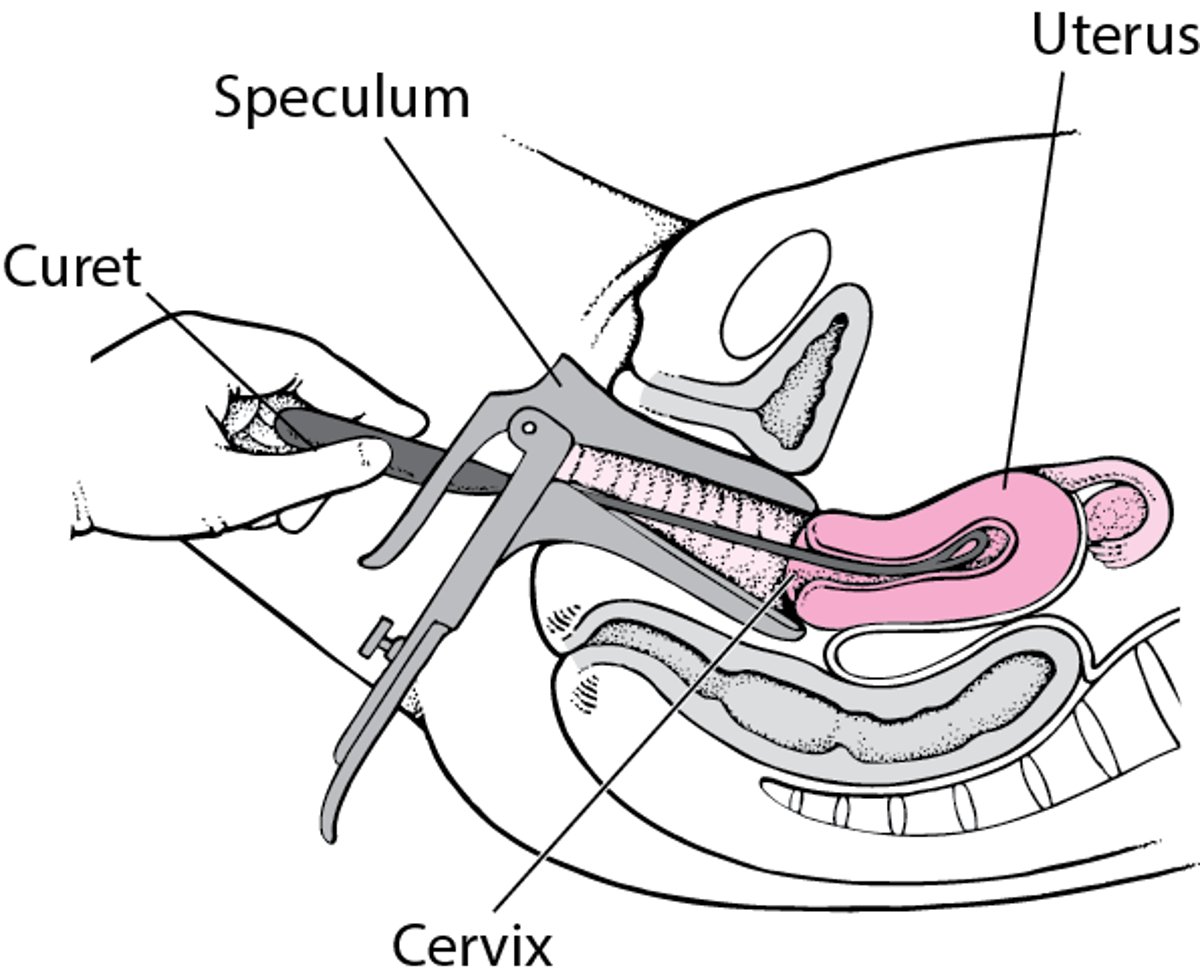
For dilation and curettage (D and C), conscious sedation or a general anesthetic is usually used. (With conscious sedation, people can respond to directions but do not feel pain.) Then, a speculum is used to spread the walls of the vagina, and the cervix is widened (dilated) using thin rods of increasing size. Sometimes a medication is used to help dilate the cervix. Then a small, sharp, scoop-shaped instrument (curet) can be inserted to remove tissue from the lining of the uterus. Sometimes a plastic tube attached to a suction machine (suction curet) or other instruments are used, if tissue needs to be removed for a miscarriage or other pregnancy-related issue.
D and C
After the speculum is in place, tapered curved metal rod (dilators—not shown) are used to stretch open the cervix so that the curet can be inserted into the uterus. The curet is used to remove tissue from the lining of the uterus. |

D and C may be used to treat women who have abnormal uterine bleeding or an incomplete (partial) miscarriageor other retained products of conception after a pregnancy. It is often done during the same procedure as hysteroscopy so that the doctor can see the inside of the uterine cavity.
D and C is often done in a hospital operating room. However, most women do not have to stay overnight in the hospital.
Hysteroscopy
To view the interior of the uterus, doctors can insert a thin viewing tube (hysteroscope) through the vagina and cervix into the uterus. The tube is 4 or 5 mm (about 1/4 inch) in diameter and contains cables that transmit light. Instruments used for a biopsy, electrocautery (heat), or surgery may be threaded through the tube. The site of abnormal bleeding or other abnormalities can usually be seen and can be sampled for a biopsy, sealed off using heat, or removed.
Hysteroscopy may be used for evaluation or treatment of the passageway through the cervix (called the endocervix or cervical canal) or the uterine cavity to do the following:
Diagnose abnormalities inside the uterus, such as polyps, fibroids, endometrial hyperplasia (overgrowth of the lining of the uterus), uterine cancer, scar tissue, or other abnormalities.
To treat abnormalities inside the uterine cavity, such removal of a polyp, fibroid, misplaced intrauterine device, or other abnormality or endometrial ablation (a procedure to treat heavy uterine bleeding by applying heat or other types of energy to thin the lining of the uterus).
Hysteroscopy for diagnosis (and some types of treatment) is sometimes done in a doctor's office. More frequently, it is done in a hospital with a general anesthetic.
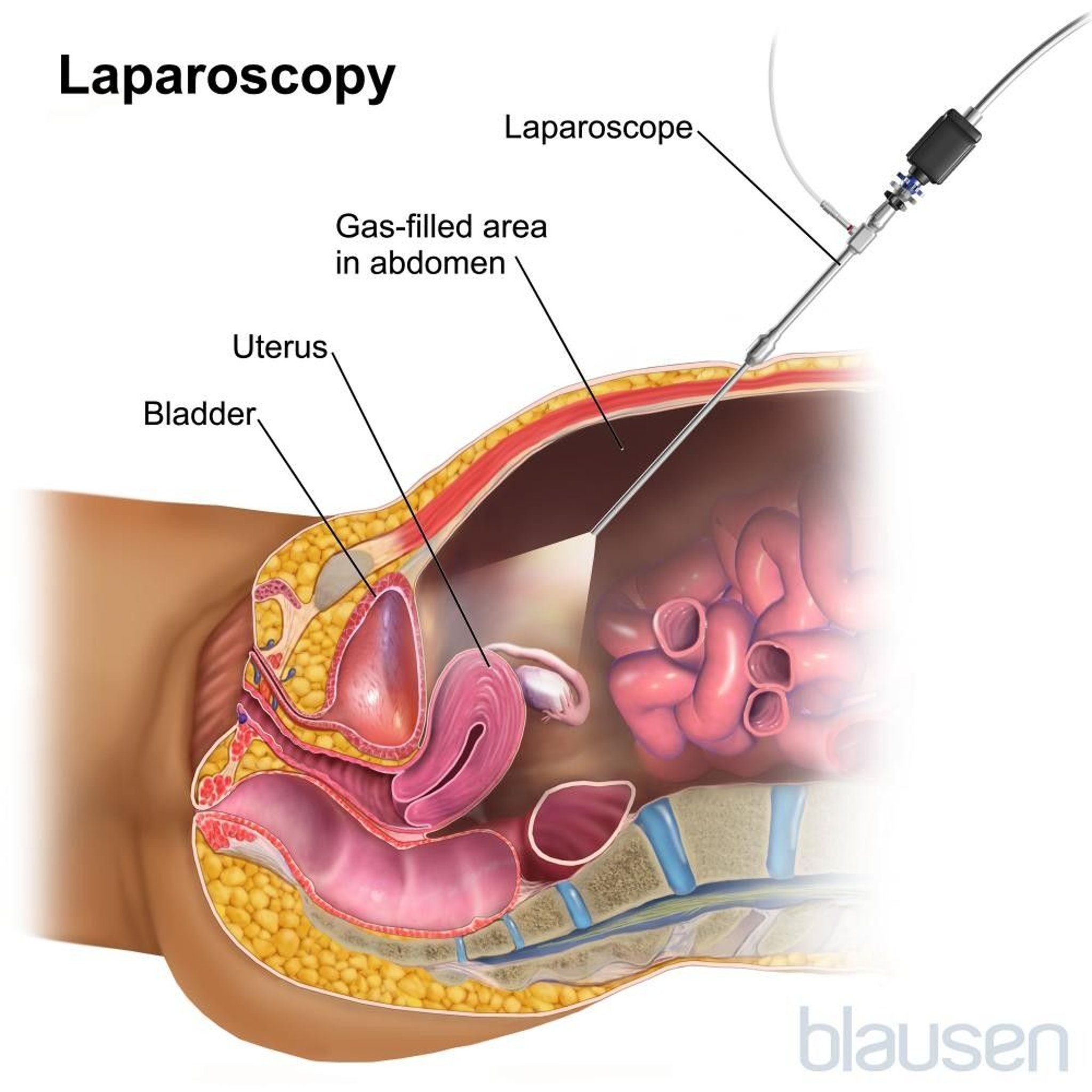
Laparoscopy
To directly examine the uterus, fallopian tubes, or ovaries, doctors use a viewing tube called a laparoscope. The laparoscope is attached to a thin cable containing flexible plastic or glass rods that transmit light.
The laparoscope is inserted into the abdominal cavity through a small incision just below the navel. A probe is inserted through the vagina and into the uterus. The probe enables doctors to manipulate the organs for better viewing. Carbon dioxide is pumped through the laparoscope to inflate the abdomen, so that organs in the abdomen and pelvis can be seen clearly.

Often, laparoscopy is used to do the following:
To determine the cause of pelvic pain, infertility, and other gynecologic disorders
To do surgical procedures, such as biopsies, tubal sterilization, removal of an ovarian cyst, removal of the ovaries and fallopian tubes, removal of an ectopic pregnancy in a fallopian tube, hysterectomy, or pelvic organ prolapse surgery.
Laparoscopy can detect structural abnormalities too small to be detected by imaging, as well as abnormalities on the surfaces of organs, such as (endometrial tissue outside the uterus), inflammation, and scarring.
Additional incisions may be required if more extensive surgical procedures, such as removal of an ovarian cyst or the uterus (hysterectomy), are needed.
Laparoscopy is done in a hospital and requires an anesthetic, usually a general anesthetic. An overnight stay in the hospital is usually not required. Laparoscopy may cause abdominal pain, but normal activities can usually be resumed in 3 to 5 days, depending on the extent of the procedure that is done through the laparoscope.







