



Noncancerous (benign) ovarian growths include cysts (mainly functional cysts) and masses, including noncancerous tumors.
Topic Resources


Most noncancerous cysts and tumors do not cause any symptoms, but some cause pain or pressure in the pelvic area.
Doctors may detect growths during a pelvic examination, then use ultrasonography to confirm the diagnosis.
Some cysts disappear on their own.
Cysts or tumors may be removed through one or more small incisions or one large incision in the abdomen, and sometimes the affected ovary must also be removed.

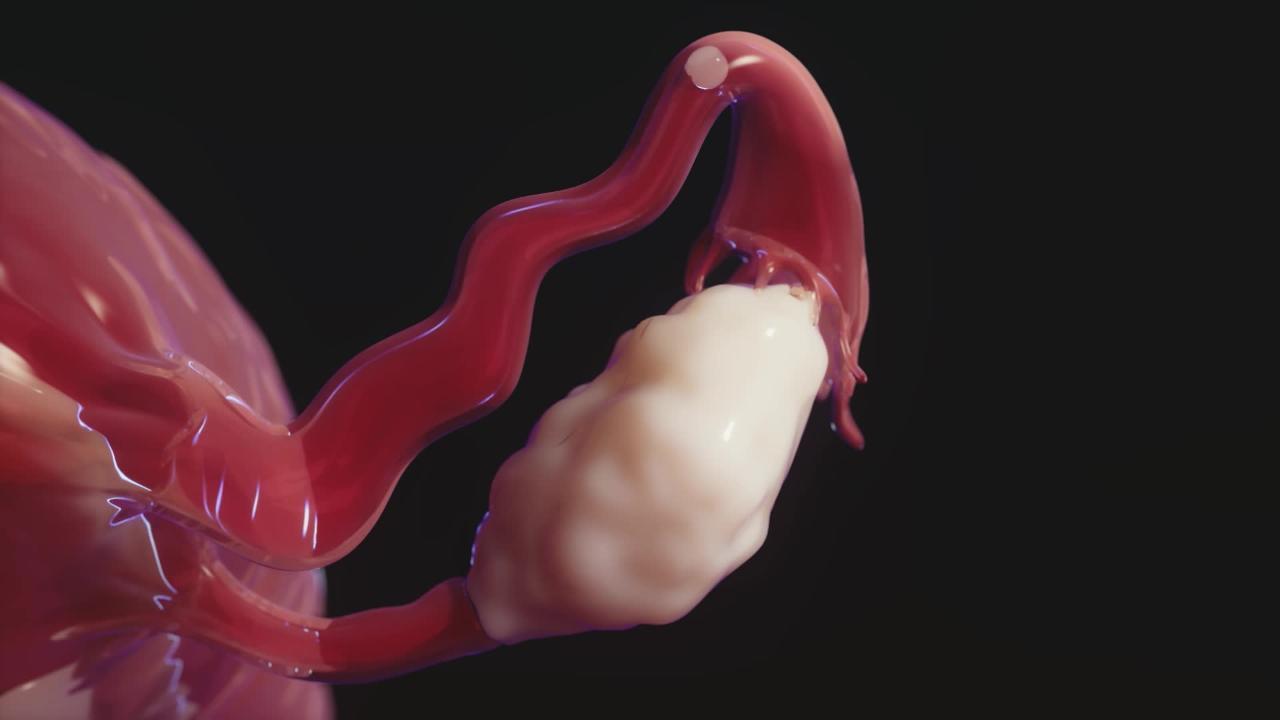
VERONIKA ZAKHAROVA/SCIENCE PHOTO LIBRARY
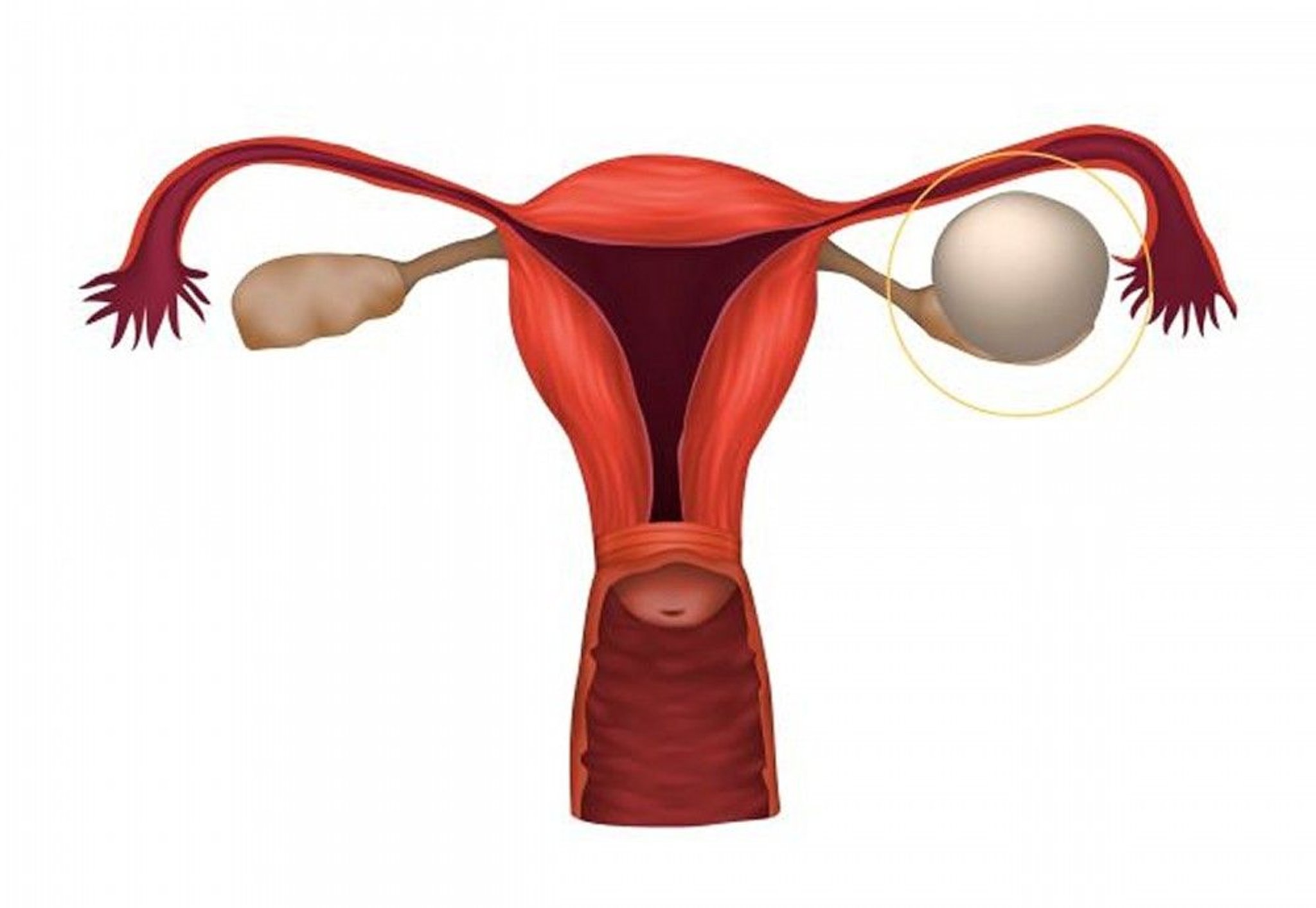
Ovarian cysts are fluid-filled sacs that form in or on an ovary. Such cysts are relatively common. Most are noncancerous (benign) and disappear on their own. Ovarian cancer is more likely to occur in women over 50.

Functional ovarian cysts
Functional cysts form from the fluid-filled cavities (follicles) in the ovaries. Each follicle contains one egg. Usually, during each menstrual cycle, one follicle releases one egg, and the follicle goes away after the egg is released. However, if an egg is not released, the follicle may continue to enlarge, forming a larger cyst.
About one third of premenopausal women develop a cyst. Functional cysts seldom develop after menopause.
There are two types of functional cysts:
Follicular cysts: These cysts form as the egg is developing in the follicle.
Corpus luteum cysts: These cysts develop from the structure that forms after the follicle ruptures and releases its egg. This structure is called the corpus luteum. Corpus luteum cysts may bleed, causing the ovary to bulge, or they may rupture. If the cyst ruptures, fluids escape into spaces in the abdomen (the abdominal cavity) and may cause severe pain.
Most functional cysts are less than about 2/3 inch (1.5 centimeters) in diameter. A few are 2 inches (5 centimeters) or more.
Functional cysts usually disappear on their own after a few days or weeks.
Benign ovarian tumors
Noncancerous (benign) ovarian tumors usually grow slowly and rarely become cancerous. The most common include the following:
Benign teratomas (dermoid cysts): These tumors usually develop from all three layers of tissue in the embryo (called germ cell layers). All organs form from these tissues. Thus, teratomas may contain tissues from other structures, such as nerves, glands, and skin.
Fibromas: These tumors are solid masses composed of connective tissue (the tissues that hold structures together). Fibromas are slow-growing and are usually less than 3 inches (about 7 centimeters) in diameter. They usually occur on only one side.
Cystadenomas: These fluid-filled cysts develop from the surface of the ovary and contain some tissue from glands in the ovaries.
Symptoms
Most functional cysts and noncancerous ovarian tumors do not cause any symptoms. But some cause intermittent dull or sharp pelvic pain. Sometimes they cause menstrual abnormalities. A few women feel pain deep in the abdomen during sexual activity.
Some cysts produce hormones that affect menstrual periods. As a result, periods may be irregular or heavier than normal. Spotting may occur between periods. In postmenopausal women, such cysts may cause vaginal bleeding.
If corpus luteum cysts bleed, they may cause pain or tenderness in the pelvic area.
Occasionally, sudden, severe abdominal pain occurs because a large cyst or mass causes the ovary to twist (a disorder called adnexal torsion).
Rarely, fluid accumulates in the abdomen (ascites) or around the lungs (pleural effusion) in women with fibromas or ovarian cancer. The combination of fibromas, ascites, and pleural effusion is called Meigs syndrome. Ascites may cause a feeling of pressure or heaviness in the abdomen.
Diagnosis
A pelvic examination
Ultrasonography
Sometimes blood tests
Doctors sometimes detect cysts or tumors during a routine pelvic examination. Sometimes doctors suspect them based on symptoms. Often, they are identified when an imaging test (such as ultrasonography) is done for another reason.
When the diagnosis needs to be confirmed, ultrasonography using an ultrasound device inserted into the vagina (transvaginal ultrasonography) is done.
A pregnancy test is done to rule out pregnancy, including pregnancy located outside the uterus (ectopic pregnancy).
If imaging suggests that the growth could be cancerous or if ascites is present, doctors remove the growth and examine it under a microscope. A laparoscope, inserted through a small incision just below the navel, may be used to examine the ovaries and to remove the growth.
If doctors suspect ovarian cancer, they do blood tests to check for substances called tumor markers, which may appear in the blood or may increase when some cancers are present. However, these tests are not reliable for diagnosis. They are most useful for monitoring how women with ovarian cancer respond to treatment
Treatment
For some cysts, regular monitoring with transvaginal ultrasonography
Sometimes surgery
Ovarian cysts
If ovarian cysts are less than about 2 inches (about 5 centimeters) in diameter, they usually disappear without treatment. Transvaginal ultrasonography is done periodically to determine whether they are disappearing.
If a cyst is larger than about 2 inches (5 centimeters) and does not disappear, it may need to be removed. If cancer cannot be ruled out, the ovary is removed. If the cyst is cancerous, the cysts and the affected ovary and fallopian tube are removed. For some large cysts if they have no characteristics of cancer, monitoring with transvaginal ultrasonography may be all that is needed.
Ovarian tumors
Benign tumors, such as fibromas and cystadenomas, require treatment.
If a tumor appears cancerous, surgery is done to evaluate the tumor and, if possible, to remove it. One of the following procedures is done:
Laparoscopy
Laparotomy
Laparoscopy requires one or more small incisions in the abdomen. It is done in a hospital and usually requires a general anesthetic. However, women may not have to stay overnight.
Laparotomy is similar but requires a larger incision and an overnight stay in the hospital.
Which procedure is used depends on how large the growth is and whether other organs are affected.
If technically feasible, doctors aim to preserve the ovaries by removing only the cyst (cystectomy).
Removal of the affected ovary (oophorectomy) is necessary for the following:
Fibromas or other solid tumors if the tumor cannot be removed by cystectomy
Cystadenomas
Cystic teratomas that are larger than 4 inches
Cysts that cannot be surgically separated from the ovary
Most cysts that occur in postmenopausal women and that are larger than about 2 inches







