






 Myocardial Perfusion Markers")
Radionuclide imaging uses a special detector (gamma camera) to create an image following injection of radioactive material. This test is done to evaluate
Coronary artery disease (CAD)
Other cardiac disorders
Radionuclide imaging can expose patients to similar amounts of radiation than do comparable computed tomography (CT) studies. However, because the radioactive material is retained in the patient briefly, sophisticated radiation alarms (eg, in airports) may be triggered by the patient for several days after such testing
Single-Photon Emission Computed Tomography (SPECT)

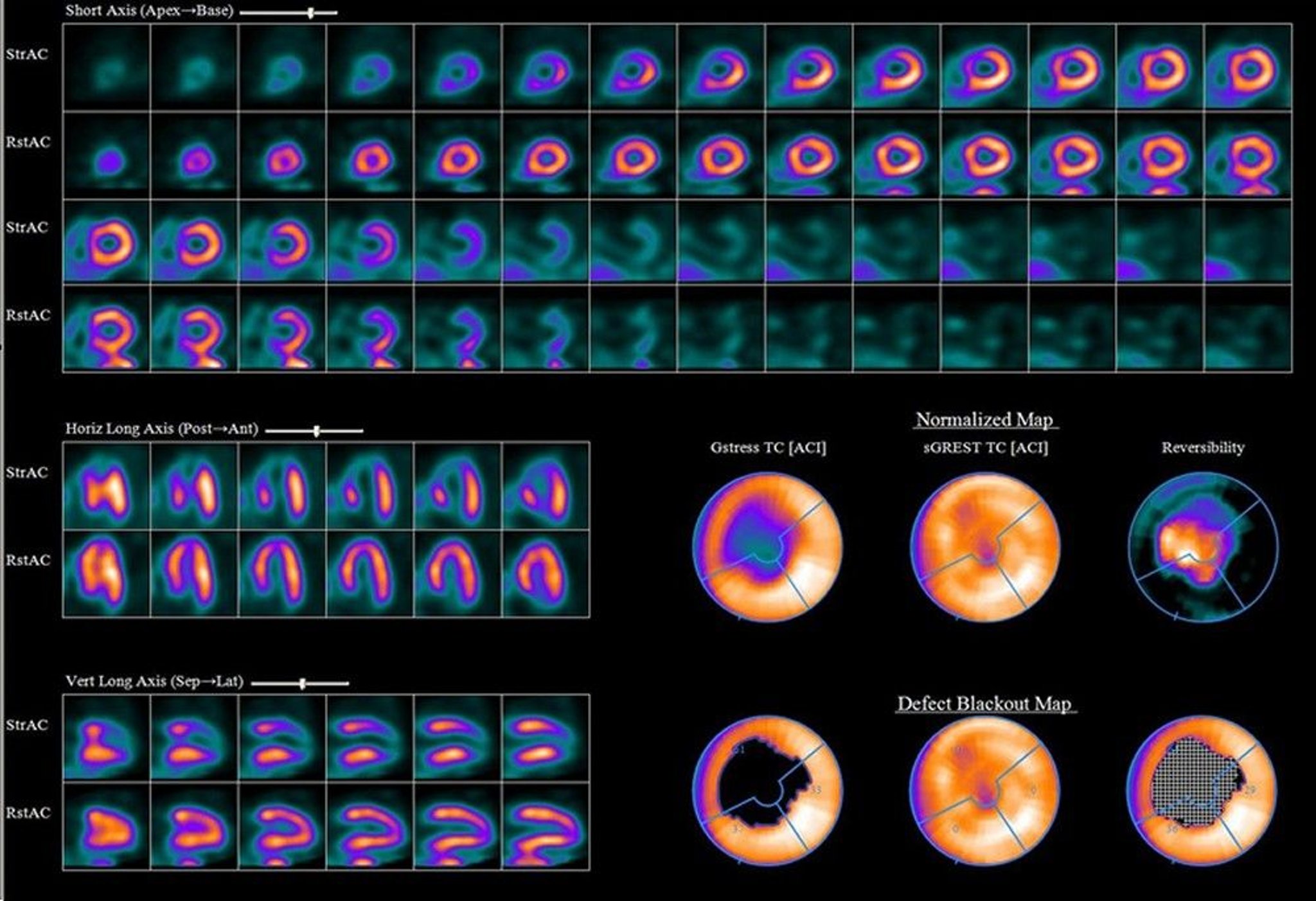
Image provided by James R. Corbett, MD.
Planar techniques, which produce a 2-dimensional image, are rarely used; SPECT, which uses a rotating camera system and tomographic reconstruction to produce a 3-dimensional image, is more common in the United States. With multihead SPECT systems, imaging can often be completed in ≤ 10 minutes. Visual comparison of stress and delayed images can be supplemented by quantitative displays. With SPECT, the following can be identified:
Inferior and posterior abnormalities
Small areas of infarction
Vessels responsible for infarction
The mass of infarcted and viable myocardium can be quantified, helping determine prognosis.
Myocardial Perfusion Imaging
In myocardial perfusion imaging, IV radionuclides are taken up by cardiac tissues in rough proportion to perfusion; thus, areas of decreased uptake represent areas of relative or absolute ischemia.
Attenuation of myocardial activity by overlying soft tissue may cause false-positive results. Attenuation by breast tissue in women is especially common. Attenuation by the diaphragm and abdominal contents may produce spurious inferior wall defects in both sexes but is more common among men. Attenuation is more likely with technetium-99m (99mTc) than with radioactive thallium 201 (Tl-201).
Indications
Myocardial perfusion imaging is used with stress testing to
Evaluate patients with chest pain of uncertain origin
Determine the functional significance of coronary artery stenosis seen on angiography
Determine the functional significance of collateral vessels seen on angiography
Evaluate the success of reperfusion interventions (eg, coronary artery bypass grafting [CABG], percutaneous intervention, thrombolysis)
Estimate prognosis after myocardial infarction

LIVING ART ENTERPRISES/SCIENCE PHOTO LIBRARY
After acute myocardial infarction, myocardial perfusion imaging can help estimate prognosis because it can show extent of the perfusion abnormality due to acute myocardial infarction, extent of scarring due to previous infarcts, and residual peri-infarct or other areas of reversible ischemia.
Protocols and imaging agents
Various protocols are used depending on the imaging agent, which include
Radioactive thallium-201 (Tl-201)
Technetium-99m (Tc-99m) markers (sestamibi, tetrofosmin, and teboroxime)
Iodine-123 (I-123)–labeled fatty acids
I-123 metaiodobenzylguanidine (MIBG)
Radioactive thallium-201 (Tl-201), which acts as a potassium analog, was the original tracer used in stress testing. It is injected at peak stress and imaged with SPECT, followed 4 hours later by injection of half the original dose during rest and by repeat SPECT. The goal of this protocol is to evaluate reversible perfusion defects that may warrant intervention. After stress testing, the perfusion imbalance between normal coronary arteries and those distal to a stenosis appears as a relative decrease in Tl-201 uptake in the areas perfused by the stenosed arteries. Sensitivity of stress testing with Tl-201 for coronary artery disease is similar whether imaging is done after exercise stress or pharmacologic stress. The use of Tl-201 has declined recently in favor of agents with improved image quality and lower radiation doses.
Several technetium-99m (Tc-99m) myocardial perfusion markers have been developed because the imaging characteristics of Tl-201 are not ideal for the gamma camera. Markers include sestamibi (commonly used), tetrofosmin, and teboroxime (see table Technetium-99m Myocardial Perfusion Markers). Protocols include 2-day stress-rest, 1-day rest-stress, and 1-day stress-rest. Some protocols use dual isotopes (Tl-201 and Tc-99m), although this approach is expensive. With either of these markers, sensitivity is about 90%, and specificity is about 71% to detect coronary artery disease.
For 2-day protocols, imaging at rest may be omitted if the initial stress test shows no evidence of abnormal perfusion. When higher doses of Tc-99m (> 30 millicurie) are used, first-transit function studies (with ventriculography) may be used with perfusion imaging.
Other radionuclides include iodine-123 (I-123)–labeled fatty acids, which produces cold spots where myocardium is ischemic; gallium citrate-67 (Ga-67), which accumulates in sites of active inflammation (eg, in acute inflammatory cardiomyopathy); and I-123 metaiodobenzylguanidine, a neurotransmitter analog taken up and stored in neurons of the sympathetic nervous system and used in research to evaluate heart failure, diabetes, pheochromocytoma, certain arrhythmias, and arrhythmogenic right ventricular dysplasia.
Technetium-99m (Tc-99) Myocardial Perfusion Markers
Marker | Characteristics |
|---|---|
Tc-99m sestamibi | Myocardial uptake is slower than that with thallium, but there is little myocardial washout, allowing timing flexibility; patients with acute symptoms can be injected with sestamibi immediately and imaged several hours later. Uptake depends more on blood flow than on viable myocardium; viable regions with low blood flow may be misclassified as scar. Studies may be done on a single or on separate days, with a low initial dose during stress followed by a much higher dose at rest. With electrocardiography (ECG)-gated imaging, ventricular wall motion, wall thickening, and ejection fraction can be estimated. |
Tc-99m tetrofosmin | Characteristics are similar to those of sestamibi. |
Tc-99m teboroxime | First-pass extraction from the myocardium is high, with rapid washout; half of peak myocardial activity is gone by 10 minutes. Because of its rapid dynamics, use with treadmill exercise is difficult. Studies suggest that stress-redistribution testing may be completed within 15 minutes of pharmacologic stress. Coronary artery disease may be detectable by analyzing myocardial washout of the tracer after injection at rest without the need for stress. |
Infarct Avid Imaging
Infarct avid imaging uses radiolabeled markers that accumulate in areas of damaged myocardium, such as Tc-99m pyrophosphate and antimyosin (indium-111 [In-111]–labeled antibodies to cardiac myosin). Images usually become positive 12 to 24 hours after acute myocardial infarction and remain positive for about 1 week; they may remain positive if myocardial necrosis continues post-myocardial infarction or if aneurysms develop. This technique is rarely used now because other diagnostic tests for myocardial infarction (eg, biomarkers) are more readily available and less expensive and because it provides no prognostic information other than infarct size.
Tc-99m pyrophosphate is now being used similarly to evaluate cardiac involvement in transthyretin amyloidosis (a type of amyloidosis in which sheets of misfolded transthyretin protein can accumulate in tissues, including the heart). Transthyretin amyloid deposits in the myocardium are particularly avid for Tc-99m pyrophosphate. Absent serum and urine manifestations of a light chain amyloidosis (which also can infiltrate the myocardium and result in a positive scan) or a recent infarct, a high ratio of uptake in the myocardium is specific for transthyretin cardiac amyloidosis and can eliminate the need for myocardial biopsy.
Radionuclide Ventriculography
Radionuclide ventriculography is used to evaluate ventricular function. It is useful for measuring resting and exercise ejection fraction in coronary artery disease, valvular heart disease, and congenital heart disease. Some clinicians prefer it for serial assessment of ventricular function in patients taking cardiotoxic cancer chemotherapy (eg, anthracyclines). However, radionuclide ventriculography has been largely replaced by echocardiography, which is less expensive, does not require radiation exposure, and theoretically can measure ejection fractions as accurately.
Tc-99m–labeled red blood cells are injected intravenously. Left ventricular (LV) and right ventricular (RV) function can be evaluated by
First-transit studies (a type of beat-to-beat evaluation)
Gated (electrocardiography [ECG]-synchronized) blood pool imaging done over several minutes (multiple-gated acquisition [MUGA])
Either study can be done during rest or after exercise. First-transit studies are rapid and relatively easy, but MUGA provides better images and is more widely used.
In first-transit studies, 8 to 10 cardiac cycles are imaged as the marker mixes with blood and passes through the central circulation. First-transit studies are ideal for assessing RV function and intracardiac shunts.
In MUGA, imaging is synchronized with the R wave of the ECG. Multiple images are taken of short, sequential portions of each cardiac cycle for 5 to 10 minutes. Computer analysis generates an average blood pool configuration for each portion of the cardiac cycle and synthesizes the configurations into a continuous cinematic loop resembling a beating heart.
MUGA can quantitate numerous indexes of ventricular function, including regional wall motion, ejection fraction (EF); ratio of stroke volume to end-diastolic volume, ejection and filling rates, LV volume, and indexes of relative volume overload (eg, LV:RV stroke volume ratios). EF is used most commonly.
MUGA during rest has virtually no risk. It is used for serially evaluating RV and LV function in various disorders (eg, valvular heart disorders); for monitoring patients taking potentially cardiotoxic drugs (eg, doxorubicin); and for assessing the effects of angioplasty, coronary artery bypass grafting (CABG), thrombolysis, and other procedures in patients with CAD or myocardial infarction. Arrhythmias are a relative contraindication because there may be few normal cardiac cycles.MUGA during rest has virtually no risk. It is used for serially evaluating RV and LV function in various disorders (eg, valvular heart disorders); for monitoring patients taking potentially cardiotoxic drugs (eg, doxorubicin); and for assessing the effects of angioplasty, coronary artery bypass grafting (CABG), thrombolysis, and other procedures in patients with CAD or myocardial infarction. Arrhythmias are a relative contraindication because there may be few normal cardiac cycles.
Left ventriculography
MUGA is useful for detecting left ventricular aneurysms; sensitivity and specificity are > 90% for typical anterior or anteroapical true aneurysms. Conventional gated blood pool imaging shows inferoposterior LV aneurysms less well than it shows anterior and lateral aneurysms; additional views are required. Gated SPECT imaging takes longer (about 20 to 25 minutes with a multihead camera) than a single planar gated view (5 to 10 minutes) but shows all portions of the ventricles.
Right ventriculography
MUGA is used to assess right ventricular function in patients who have a lung disorder or an inferior left ventricular infarct that may involve the RV. Normally, right ventricular ejection fraction (40 to 55% with most techniques) is lower than left ventricular ejection fraction. RVEF is low in many patients with pulmonary hypertension and in patients with RV infarction or cardiomyopathy affecting the RV. Idiopathic cardiomyopathy is usually characterized by biventricular dysfunction, unlike typical coronary artery disease, which usually causes more left ventricular than right ventricular dysfunction.
Valve assessment
MUGA can be used with rest-stress protocols to assess valvular disorders that result in left ventricular volume overload. In aortic regurgitation, a reduction in resting EF or no increase in EF with exercise is a sign of deteriorating cardiac function and may indicate a need for valvular repair. MUGA also can be used to calculate the regurgitant fraction in regurgitation of any valve. Normally, the stroke volume of the 2 ventricles is equal. However, in patients with left-sided valvular regurgitation, LV stroke volume exceeds that of the right ventricle by an amount proportional to the regurgitant fraction. Thus, if the RV is normal, the regurgitant fraction of the LV can be calculated from the LV:RV stroke volume ratio.
Shunt assessment
With MUGA and commercially available computer programs, size of a congenital shunt can be quantified by the stroke volume ratio or, during the first transit of the marker, by the ratio of abnormal early pulmonary recirculation of radioactivity to total pulmonary radioactivity.







