


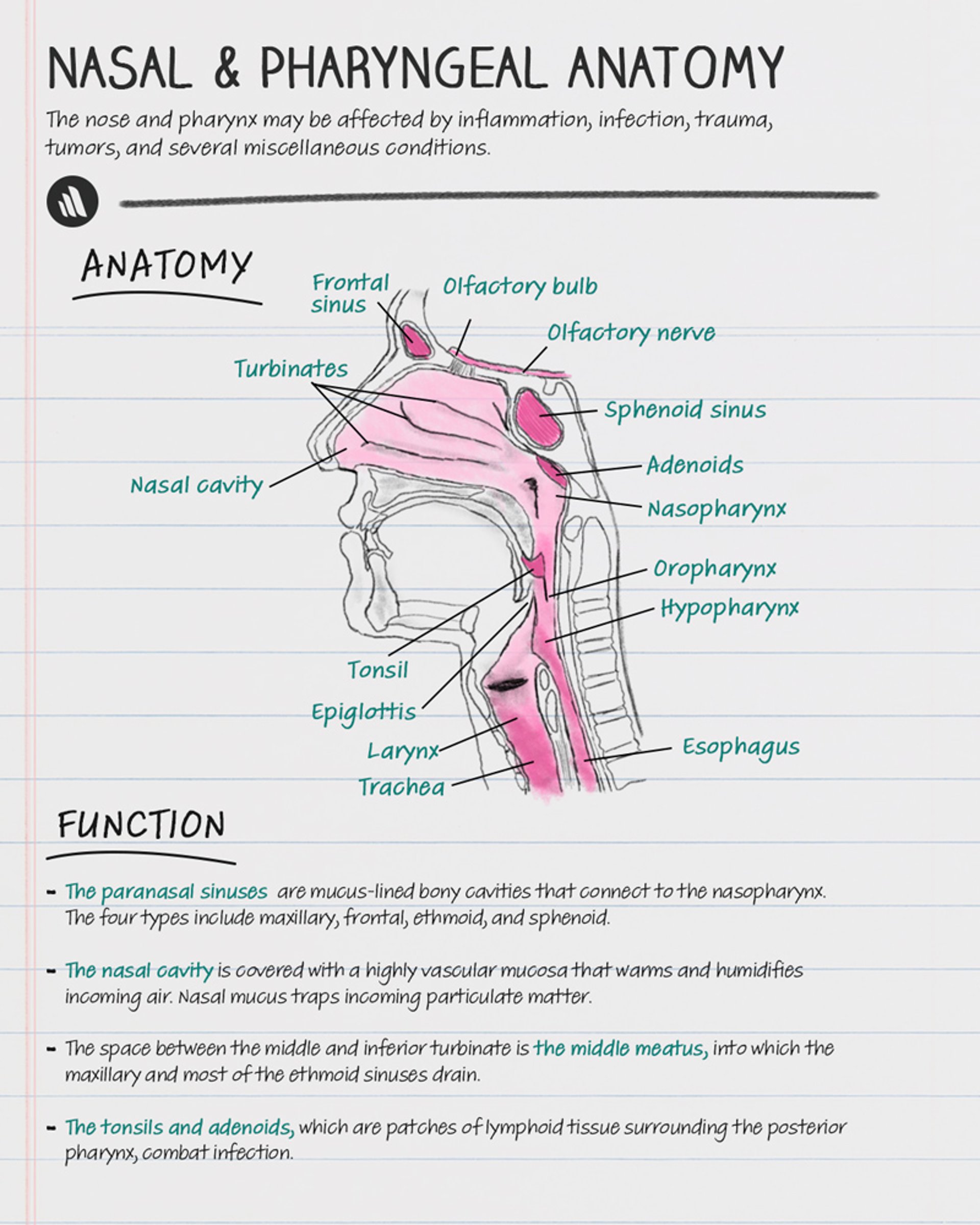
The nose and pharynx (consisting of the nasopharynx, oropharynx, and hypopharynx) may be affected by inflammation, infection, trauma, tumors, and several miscellaneous conditions.
Nasal and Pharyngeal Anatomy
Throat
The uvula hangs in the midline at the far end of the soft palate. It varies greatly in length. A long uvula and loose or excess velopharyngeal tissue may cause snoring and occasionally contribute to obstructive sleep apnea.
Tonsils and adenoids are patches of lymphoid tissue surrounding the posterior pharynx in an area termed Waldeyer’s ring. Their role is to combat infection.
The larynx is discussed in Laryngeal Disorders.

Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
Nose
Sinuses
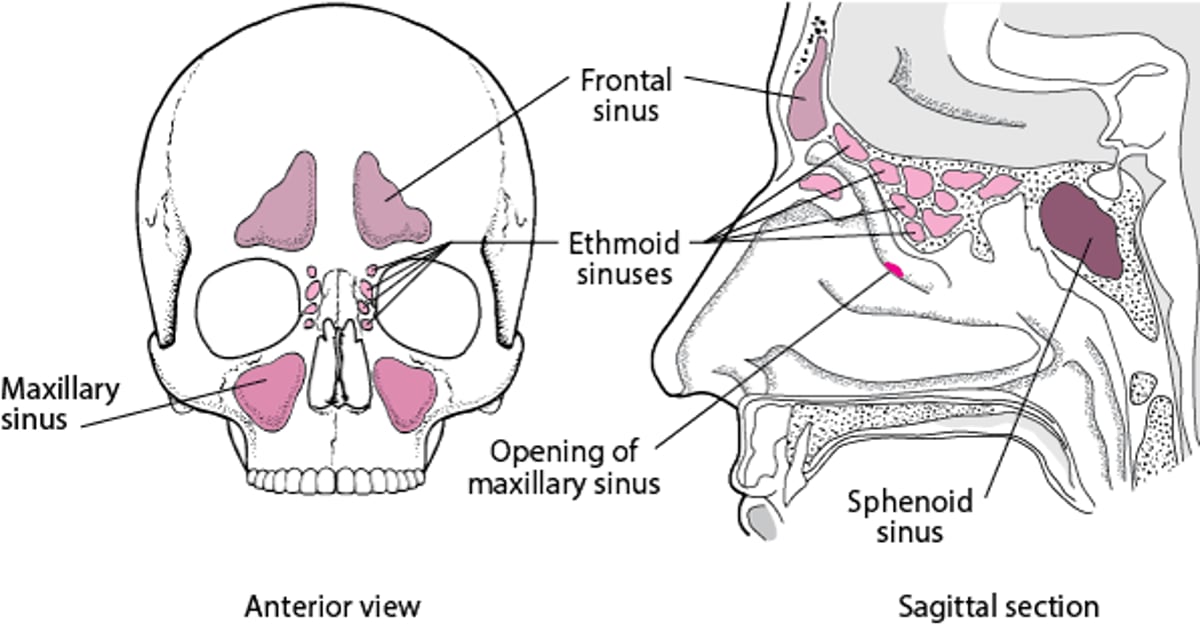
The paranasal sinuses are mucus-lined bony cavities that connect to the nasopharynx. There are four types:
Maxillary
Frontal
Ethmoid
Sphenoid
They are located in the facial and cranial bones (see figure Paranasal Sinuses). The physiologic role of the sinuses is unclear.
Paranasal sinuses

Evaluation of the Nose and Pharynx
Examination of the nose and pharynx is part of every general otorhinolaryngologic examination.
History
General information includes use of alcohol or tobacco (both major risk factors for head and neck cancer) and systemic symptoms, such as fever and weight loss.
Oropharyngeal symptoms include
Mouth and throat pain
Mouth and throat ulcers
Difficulty swallowing or speaking
Nasal and sinus symptoms include
Congestion (noting presence and duration)
Nasal discharge
Loss of smell and/or taste
Bleeding from the nose
Physical examination
Some otorhinolaryngologic physicians use a head-mounted light. However, because the light cannot be precisely aligned on the axis of vision, it is difficult to avoid shadowing in narrow areas (eg, nasal cavity). Illumination is better if the head-mounted mirror is convex; the physician looks through a hole in the center of the mirror, so the illumination is always on-axis. The head mirror reflects light from a source placed behind the patient and slightly to one side and requires practice to use effectively.
The nose is examined using a nasal speculum, which is held so that the two blades open in an anteroposterior (or slightly oblique) direction and do not press against the septum. The physician notes any crusting, discharge, septal deviation, or perforation; whether mucosa is erythematous, boggy, or swollen; and presence of polyps. The skin over the frontal and maxillary sinuses is examined for erythema and tenderness, suggesting sinus inflammation.
Alternatively, a mirror examination can be done. A topical pharyngeal anesthetic for the throat is required for this examination. The mirror should be warmed before use to avoid fogging. A small mirror is used for the nasopharynx. It is held just below the uvula, angling upward; the tongue is pushed down with a tongue blade. A larger mirror is used for the hypopharynx and larynx. The tongue is retracted by grasping it with a gauze pad, and the mirror is placed against the soft palate, angling downward.
Neck examination consists of inspection and palpation for masses. If masses are found, the physician notes whether they are tender; fluctuant, firm, or stony hard and whether they are movable or fixed. Masses caused by infection are tender and mobile; cancers tend to be nontender, hard, and fixed. Particular attention is paid to the cervical lymph nodes and thyroid and parotid glands.







