



Vocal cord paralysis has numerous causes and can affect speaking, breathing, and swallowing. The left vocal cord is affected twice as often as the right, and females are affected more often than males (3:2). Diagnosis is based on direct visualization. An extensive assessment may be necessary to determine the cause. Several direct surgical approaches are available if treating the cause is not curative.
Topic Resources

Etiology of Vocal Cord Paralysis
Vocal cord paralysis may result from lesions or dysfunction at the level of the nucleus ambiguus, its supranuclear tracts, the main trunk of the vagus, or the recurrent laryngeal nerves. The left vocal cord is paralyzed more often than the right because the left recurrent nerve takes a longer course from the brain stem to the larynx, providing more opportunity for compression, traction, or surgical injuries.
Paralysis may be
Unilateral (most common)
Bilateral
Unilateral vocal cord paralysis is most common. About one third of unilateral paralyses are neoplastic in origin, one third are traumatic, and one third are idiopathic. Intracranial tumors, vascular insults, and demyelinating diseases cause nucleus ambiguus paralysis. Tumors at the base of the skull and trauma to the neck cause vagus paralysis. Recurrent laryngeal nerve paralysis is caused by neck or thoracic lesions (eg, aortic aneurysm; mitral stenosis; mediastinal tuberculous adenitis; tumors of the thyroid gland, esophagus, lung, or mediastinal structures), trauma, thyroidectomy, neurotoxins (eg, lead, arsenic, mercury), neurotoxic infections (eg, diphtheria), cervical spine injury or surgery, Lyme disease, and viral illness. Viral neuronitis probably accounts for most idiopathic cases.
Bilateral vocal cord paralysis is a life-threatening disorder caused by thyroid and cervical surgery, tracheal intubation, trauma, and neurodegenerative and neuromuscular diseases.
(See also Overview of Laryngeal Disorders.)
Symptoms and Signs of Vocal Cord Paralysis
Vocal cord paralysis results in loss of vocal cord abduction and adduction. Paralysis may affect phonation, respiration, and deglutition, and food and fluids may be aspirated into the trachea. The paralyzed cord generally lies 2 to 3 mm lateral to the midline.

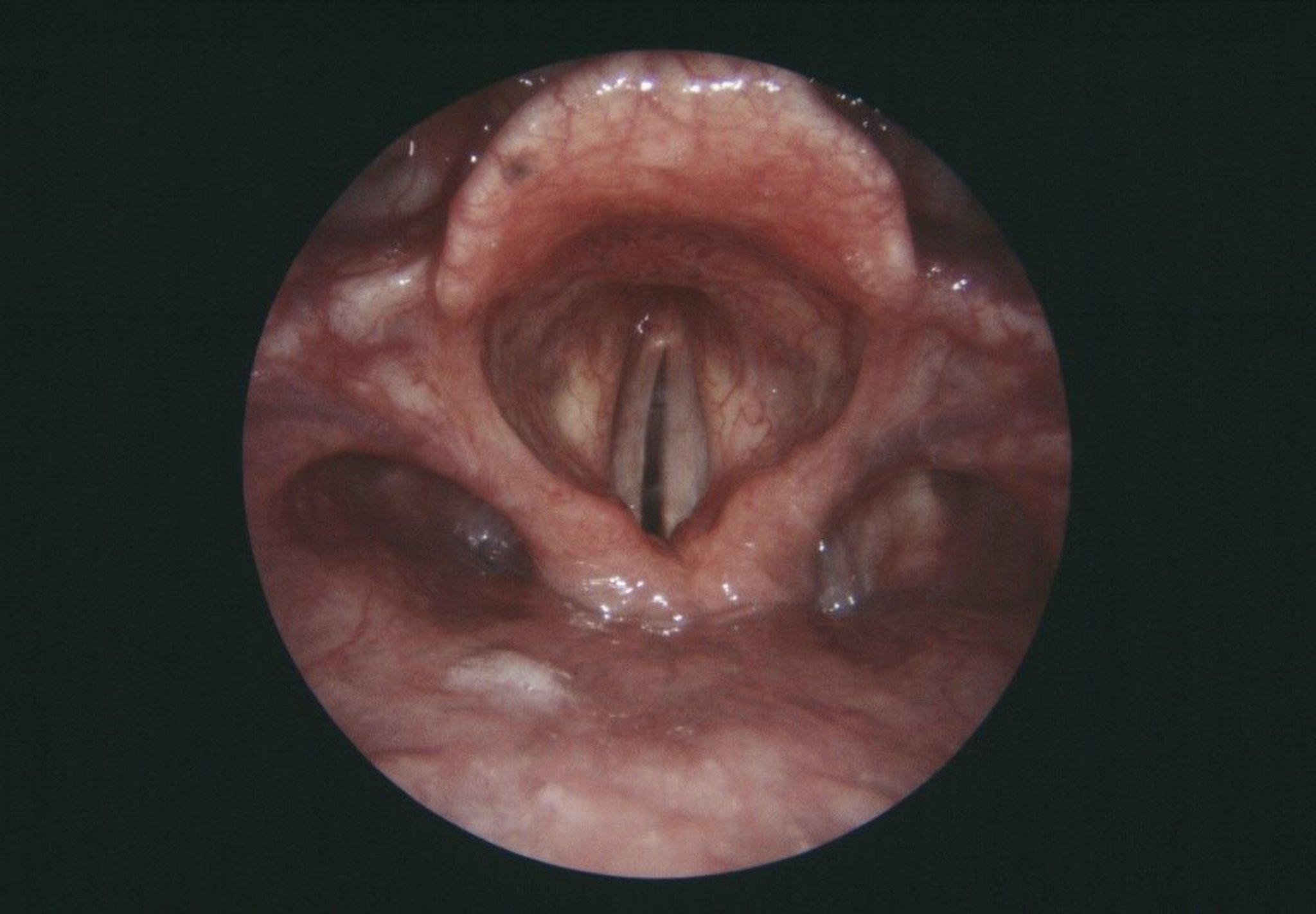
CNRI/SCIENCE PHOTO LIBRARY
In recurrent laryngeal nerve paralysis, the cord may move with phonation but not with inspiration.
In unilateral paralysis, the voice may be hoarse and breathy, but the airway is usually not obstructed because the normal cord abducts sufficiently.
In bilateral paralysis, both cords generally lie within 2 to 3 mm of the midline, and the voice is of good quality but of limited intensity and pitch modulation. The airway, however, is inadequate, resulting in stridor and dyspnea with moderate exertion as each cord is drawn to the midline glottis by an inspiratory Bernoulli effect. Aspiration is also a danger.
Diagnosis of Vocal Cord Paralysis
Laryngoscopy
Various tests for possible causes
Diagnosis of vocal cord paralysis is based on laryngoscopy. The cause must always be sought. Evaluation is guided by abnormalities identified on history and physical examination. During the history, the physician asks about all possible causes of peripheral neuropathy, including chronic heavy metal exposure (arsenic, lead, mercury), drug effects from phenytoin and vincristine, and history of connective tissue disorders, , mercury), drug effects from phenytoin and vincristine, and history of connective tissue disorders,Lyme disease, sarcoidosis, diabetes, and alcohol use disorder. Further evaluation may include enhanced CT or MRI of the head, neck, and chest; thyroid scan; barium swallow or bronchoscopy; and esophagoscopy.
Cricoarytenoid arthritis, which may cause fixation of the cricoarytenoid joint, must be differentiated from a neuromuscular etiology. Fixation is best documented by absence of passive mobility during rigid laryngoscopy under general anesthesia. Cricoarytenoid arthritis may complicate such conditions as rheumatoid arthritis, external blunt trauma, and prolonged endotracheal intubation.
Treatment of Vocal Cord Paralysis
For unilateral paralysis, surgical procedures to move cords closer together
For bilateral paralysis, surgical procedures and measures to maintain airway
In unilateral paralysis, treatment is directed at improving voice quality through augmentation, medialization, or reinnervation.
Augmentation involves injecting a paste of plasticized particles, collagen, micronized dermis, or autologous fat into the paralyzed cord, bringing the cords closer together to improve the voice and prevent aspiration.
Medialization is shifting the vocal cord toward the midline by inserting an adjustable spacer laterally to the affected cord. This can be done with a local anesthetic, allowing the position of the spacer to be “tuned” to the patient’s voice.
Reinnervation, which restores tone and positioning, but not motion, to the paralyzed vocal fold, is increasingly being used in pediatric and adult (< 55 years) patients with a nonrecoverable paralysis (1, 2).
In bilateral paralysis, an adequate airway must be reestablished. Tracheotomy may be needed permanently or temporarily during an upper respiratory infection. An arytenoidectomy with lateralization of the true vocal cord opens the glottis and improves the airway but may adversely affect voice quality. Posterior laser cordectomy opens the posterior glottis and may be preferred to endoscopic or open arytenoidectomy. Successful laser establishment of a posterior glottic airway usually obviates the need for long-term tracheotomy while preserving a serviceable voice quality. Selective reinnervation procedures are increasingly successful in select patients (3).
Treatment references
1. Espinosa MC, Ongkasuwan J: Recurrent laryngeal nerve reinnervation: is this the standard of care for pediatric unilateral vocal cord paralysis? Curr Opin Otolaryngol Head Neck Surg 26(6):431-436, 2018. doi:10.1097/MOO.0000000000000499
2. Anthony, B., Parker, N., Patel, R. et al: Surgical considerations for laryngeal reinnervation and future research directions. Curr Otorhinolaryngol Rep 8, 224–229, 2020. https://doi.org/10.1007/s40136-020-00294-7
3. Dunya, G., Orb, Q.T., Smith, M.E. et al: A review of treatment of bilateral vocal fold movement impairment. Curr Otorhinolaryngol Rep 9, 7–15, 2021. https://doi.org/10.1007/s40136-020-00320-8
Key Points
Vocal cord paralysis can be caused by a lesion or dysfunction anywhere in the neural pathway to the larynx (the nucleus ambiguus, its supranuclear tracts, the main trunk of the vagus, the recurrent laryngeal nerves).
Most paralyses are unilateral and affect mainly the voice, but bilateral paralysis can occur and obstruct the airway.
Paralysis is diagnosed by laryngoscopy, but identification of the cause typically requires imaging (eg, MRI) and other tests.
Patients with bilateral paralysis often require tracheal intubation/tracheotomy initially, before corrective surgical procedures are attempted.
Various surgical procedures are available to improve voice quality in unilateral paralysis or to improve airway patency in long-term bilateral paralysis.







