


Autoimmune metaplastic atrophic gastritis is an inherited autoimmune disease that attacks parietal cells, resulting in hypochlorhydria and decreased production of intrinsic factor. Consequences include atrophic gastritis, B12 malabsorption, and, frequently, pernicious anemia. Risk of gastric adenocarcinoma increases 3-fold. Diagnosis is by endoscopy. Treatment is with parenteral vitamin B12.
(See also Overview of Acid Secretion and Overview of Gastritis.)
Etiology of AMAG
Patients with autoimmune metaplastic atrophic gastritis (AMAG) have antibodies to parietal cells and their components (which include intrinsic factor and the proton pump H+,K+-ATPase). AMAG is inherited as an autosomal dominant trait.
Some patients also develop Hashimoto thyroiditis and 50% have thyroid antibodies; conversely, parietal cell antibodies are present in 30% of patients with thyroiditis.
In some patients, AMAG may be associated with chronic Helicobacter pylori infection, although the relationship is not clear. Gastrectomy and chronic acid suppression with proton pump inhibitors cause similar deficiencies of intrinsic factor secretion.
Complications of AMAG
Complications of AMAG include
Vitamin B12 deficiency
Gastric adenocarcinoma
Carcinoid tumor
The lack of intrinsic factor leads to vitamin B12 deficiency that can result in a megaloblastic anemia (pernicious anemia) or neurologic symptoms (subacute combined degeneration).
The areas of atrophic gastritis in the body and fundus may manifest as metaplasia. Patients with AMAG have a 3-fold increased relative risk of developing gastric adenocarcinoma.
Patients with gland atrophy and/or intestinal metaplasia distributed multifocally, including to the lesser curvature of the corpus and fundus, have a phenotype called multifocal atrophic gastritis. Multifocal involvement is considered "extensive", in contrast to "marked," which refers to severity at a specific site. Risk of gastric adenocarcinoma is higher among patients who have multifocal atrophic gastritis.
Hypochlorhydria leads to G-cell hyperplasia and elevated serum gastrin levels (often > 1000 pg/mL [> 481 pmol/L]). Elevated gastrin levels lead to enterochromaffin-like cell hyperplasia, which occasionally undergoes transformation to a carcinoid tumor.
Symptoms and Signs of AMAG
Manifestations of autoimmune metaplastic atrophic gastritis (AMAG) itself are few and nonspecific, although some patients have upper abdominal discomfort.
Symptoms and signs of B12 deficiency may be minimal at first because anemia develops slowly, but eventually fatigue and weakness occur. Neurologic manifestations occur independently of the anemia but typically begin with decreased position and vibratory sensation in the extremities, accompanied by mild to moderate weakness and hyporeflexia.
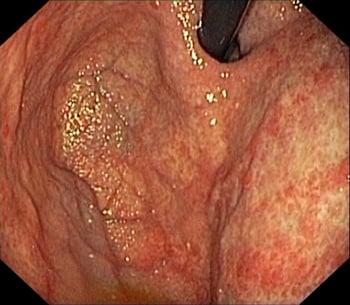
Diagnosis of AMAG
Endoscopic biopsy
There are no specific symptoms that point to this disorder. It is most often discovered when patients undergo endoscopy to evaluate upper abdominal discomfort or unexplained anemia. Endoscopic biopsy confirms the diagnosis. Serum B12 levels should be obtained. Parietal cell antibodies are usually present but are not measured routinely.

The American Gastroenterological Association's (AGA) 2020 guidelines on management of gastric intestinal metaplasia recommend testing for and treating H. pylori in patients with gastric intestinal metaplasia. The AGA guidelines also recommend against routine surveillance endoscopy in patients with autoimmune metaplastic atrophic gastritis and gastric intestinal metaplasia. Patients with atrophic gastritis and gastric intestinal metaplasia who have an increased risk of gastric cancer may elect to undergo surveillance, but they should be made aware of the low value of surveillance and the potential adverse effects of repeated upper endoscopies. Factors that increase the risk of gastric cancer include
Incomplete metaplasia
Extensive metaplasia
Family history of gastric cancer
Immigration from regions with high incidence of gastric cancer such as Korea, Japan, and South America
Routine short-interval (within 1 year) repeat endoscopy and biopsy is not recommended unless the baseline endoscopy was inadequate or showed high-risk histology or unless the patient is at increased risk of gastric cancer. Again, the decision to repeat the endoscopy within 1 year should be made after patients understand the low value of surveillance and the potential adverse effects of repeated upper endoscopies. Longer-interval (every 3 to 5 years) surveillance endoscopy among patients with incidentally detected gastric intestinal metaplasia may be reasonable if shared decision-making favors surveillance. There is no consensus on surveillance in patients with autoimmune gastritis without intestinal metaplasia. One guideline recommends endoscopic surveillance for gastric tumors every 3 to 5 years, but there is no evidence to suggest that this is cost effective (1).
The European Society of Gastrointestinal Endoscopy, European Helicobacter and Microbiota Study Group, European Society of Pathology, and Sociedade Portuguesa de Endoscopia Digestiva's 2019 update of the guidelines on management of epithelial precancerous conditions and lesions in the stomach emphasizes the use of high-definition endoscopy with chromoendoscopy in endoscopic evaluation of these patients. The guidelines recommend endoscopy every 3 years in patients with advanced atrophic gastritis or in patients with intestinal metaplasia. A small longitudinal study reported a 10% incidence of gastric tumors at 3 years in a cohort of patients with autoimmune and multifocal atrophic gastritis who underwent endoscopy at 3 years as recommended by the guidelines (2).
Diagnosis references
1. Lahner E, Zagari RM, Zullo A, et al: Chronic atrophic gastritis: Natural history, diagnosis and therapeutic management. A position paper by the Italian Society of Hospital Gastroenterologists and Digestive Endoscopists [AIGO], the Italian Society of Digestive Endoscopy [SIED], the Italian Society of Gastroenterology [SIGE], and the Italian Society of Internal Medicine [SIMI]. Dig Liver Dis 51(12):1621–1632, 2019. doi: 10.1016/j.dld.2019.09.016
2. Esposito G, Dilaghi E, Cazzato M, et al: Endoscopic surveillance at 3 years after diagnosis, according to European guidelines, seems safe in patients with atrophic gastritis in a low-risk region. Dig Liver Dis 53(4):467–473, 2021. doi: 10.1016/j.dld.2020.10.038
Treatment of AMAG
Parenteral vitamin B12
No treatment is needed other than parenteral replacement of vitamin B12.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Gastroenterological Association: Guidelines on management of gastric intestinal metaplasia (2020)
European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter Study Group (EHSG), European Society of Pathology (ESP), and the Sociedade Portuguesa de Endoscopia Digestiva (SPED): Guidelines for the management of precancerous conditions and lesions in the stomach (MAPS) (2019)







