



Bartholin gland cysts are the most common large vulvar cysts. They are mucus-filled and are located on either side of the vaginal opening. Symptoms of large cysts include vulvar pressure or pain, dyspareunia, and vulvar asymmetry. Bartholin gland cysts may form abscesses, which are painful. Diagnosis is by pelvic examination. Large cysts and abscesses require drainage and sometimes excision; abscesses require antibiotics.
Topic Resources


Bartholin glands are round, very small, nonpalpable, and located deep in the posterolateral vaginal orifice. Obstruction of the Bartholin duct causes the gland to enlarge with mucus, resulting in a cyst. Cause of obstruction is usually unknown. Rarely, the cysts result from a sexually transmitted infection (eg, gonorrhea).
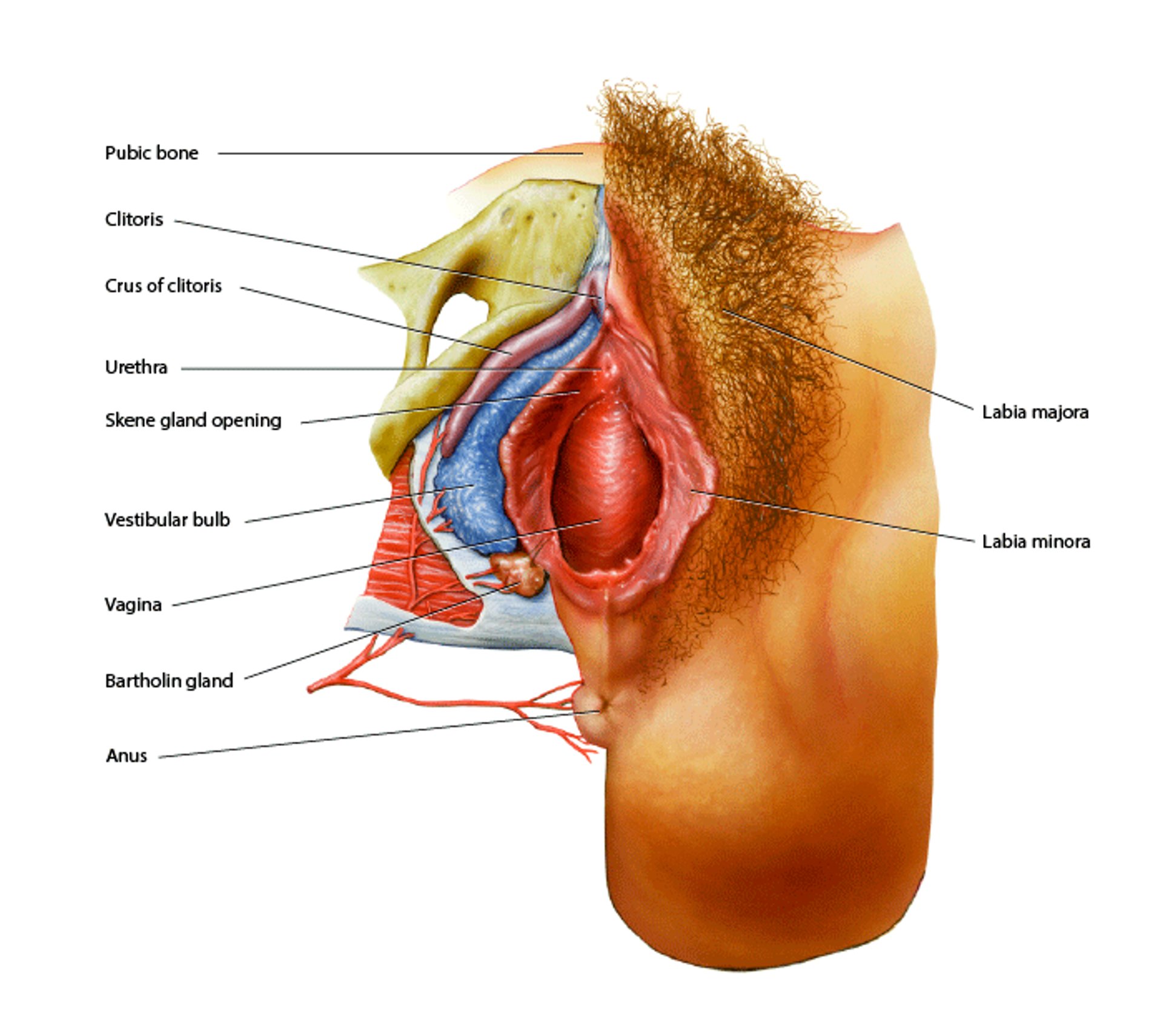
Vulvar Anatomy
At the center of this image is the vagina, a canal composed of smooth muscle. The small opening directly above it is the urethra, which is the opening from the bladder. Below the vagina is the anus. Above the urethra is the clitoris, a body of erectile tissue that is homologous to the penis. The vagina is surrounded by the labia minora, which are surrounded by the labia majora. The pubic bone is at top. The purple tissue is a continuation of the clitoris, the crus of clitoris. The bulb of the vestibule (blue) also consists of erectile tissue. Below the bulb is a Bartholin gland, which secretes mucus to lubricate the vagina. BO VEISLAND/SCIENCE PHOTO LIBRARY |

Bartholin gland cysts develop in about 2% of women, usually those in their 20s (1). With aging, cysts are less likely to develop.
A cyst may become infected, forming an abscess. Methicillin-resistant Staphylococcus aureus (MRSA) has become more common in such infections (and in other vulvar infections).
Rarely, vulvar cancers originates in Bartholin glands.
General reference
1. Berger MB, Betschart C, Khandwala N, et al: Incidental Bartholin gland cysts identified on pelvic magnetic resonance imaging. Obstet Gynecol 120 (4):798–802, 2012. doi: 10.1097/AOG.0b013e3182699259
Symptoms and Signs of Bartholin Gland Cyst or Abscess
Most Bartholin gland cysts are asymptomatic, but large cysts can be irritating, cause pressure or pain, and interfere with sexual intercourse or walking. Most cysts are nontender, unilateral, and palpable near the vaginal orifice. Cysts distend the affected labia majora, causing vulvar asymmetry.


By permission of the publisher. From Kaufman R, Brown D. In Atlas of Clinical Gynecology: Gynecologic Pathology. Edited by M Stenchever (series editor) and B Goff. Philadelphia, Current Medicine, 1998.
If an abscess develops, it causes severe vulvar pain and sometimes fever; abscesses are tender and typically erythematous. Cellulitis with localized erythema, and tenderness may develop. A vaginal discharge may be present. Sexually transmitted diseases may coexist.
Diagnosis of Bartholin Gland Cyst or Abscess
Clinical evaluation
Diagnosis of Bartholin gland cysts is usually by examination of the vulva. A sample of discharge from the cyst, if present, may be tested for sexually transmitted infections. Abscess fluid should be cultured.
In women > 40 years old, some experts recommend biopsy to exclude Bartholin gland carcinoma or other vulvar cancer.
Treatment of Bartholin Gland Cyst or Abscess
Sitz baths for mild symptoms
For abscesses, incision and drainage and usually placement of a catheter for drainage
Surgery for more severe symptoms and for all cysts in women > 40
In women < 40, asymptomatic cysts do not require treatment. Mild symptoms may resolve with sitz baths. Otherwise, symptomatic cysts may require a procedure to drain or remove the cyst.
For abscesses, a procedure is done to produce a permanent opening from the gland to the exterior because abscesses often recur after simple drainage. A small incision is made in the cyst and/or abscess, and then one of the following is done:
Catheter insertion: A small balloon-tipped catheter may be inserted, inflated, and left in the cyst for 4 to 6 weeks; this procedure stimulates fibrosis and produces a permanent opening.
Marsupialization: The everted edges of the cyst are sutured to the exterior.
Abscesses are sometimes treated with a procedure and an oral antibiotic regimen that covers MRSA (eg, trimethoprim 160 mg/sulfamethoxazole 800 mg once or twice a day OR trimethoprim 160 mg/sulfamethoxazole 800 mg once or twice a day PLUS amoxicillin-clavulanate 875 mg twice a day OR trimethoprim 160 mg/sulfamethoxazole 800 mg once or twice a day PLUS metronidazole 500 mg 3 times a day). Oral antibiotics should be used when Abscesses are sometimes treated with a procedure and an oral antibiotic regimen that covers MRSA (eg, trimethoprim 160 mg/sulfamethoxazole 800 mg once or twice a day OR trimethoprim 160 mg/sulfamethoxazole 800 mg once or twice a day PLUS amoxicillin-clavulanate 875 mg twice a day OR trimethoprim 160 mg/sulfamethoxazole 800 mg once or twice a day PLUS metronidazole 500 mg 3 times a day). Oral antibiotics should be used whencellulitis is also present; antibiotics should be chosen based on that region's antibiogram. Inpatient admission for IV antibiotics should be strongly considered if patients have poorly controlled diabetes mellitus or are immunocompromised.
Recurrent cysts or abscesses may require complete excision of the Bartholin gland.
In women > 40, newly developed cysts or abscesses should be surgically biopsied (to exclude vulvar cancer) or removed. Cysts that have been present for years and have not changed in appearance do not require biopsy or surgical removal unless symptoms are present.
Key Points
Bartholin gland cysts are vulvar cysts.
They result from ductal obstruction; the cause is usually unknown.
Cysts may become infected, sometimes with MRSA, and form an abscess.
For abscesses and for cysts that cause bothersome symptoms, treat with an incision and drainage procedure (eg, with catheter insertion, marsupialization, and/or excision).
In women > 40 years old, biopsy newly developed cysts to exclude vulvar cancer
Surgically remove a Bartholin gland if a patient has recurrent cysts or abscesses or if cancer is suspected.







