


- Liver Structure and Function
- Evaluation of the Patient With a Liver Disorder
- The Asymptomatic Patient With Abnormal Liver Test Results
- Acute Liver Failure
- Ascites
- Inborn Metabolic Disorders Causing Hyperbilirubinemia
- Jaundice
- Metabolic Dysfunction–Associated Liver Disease (MASLD)
- Portal Hypertension
- Portosystemic Encephalopathy
- Postoperative Liver Dysfunction
- Spontaneous Bacterial Peritonitis (SBP)
- Systemic Abnormalities in Liver Disease
Portal hypertension is elevated pressure in the portal vein. It is caused most often by cirrhosis (in North America), schistosomiasis (in endemic areas), or hepatic vascular abnormalities. Consequences include esophageal varices and portosystemic encephalopathy. Diagnosis is based on clinical criteria, often in conjunction with imaging tests and endoscopy. Treatment involves prevention of gastrointestinal (GI) bleeding with endoscopy, drugs, or both and sometimes with portacaval shunting or liver transplantation.
Topic Resources



(See also Liver Structure and Function and Evaluation of the Patient With a Liver Disorder.)
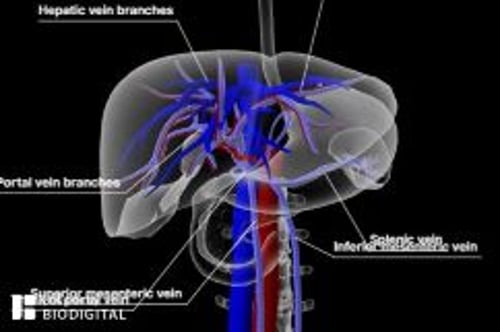
The portal vein, formed by the superior mesenteric and splenic veins, drains blood from the abdominal GI tract, spleen, and pancreas into the liver. Within reticuloendothelium-lined blood channels (sinusoids), blood from the terminal portal venules merges with hepatic arterial blood. Blood flows out of the sinusoids via the hepatic veins into the inferior vena cava.
Normal portal pressure is 5 to 10 mm Hg (7 to 14 cm H2O), which exceeds inferior vena caval pressure by 4 to 5 mm Hg (portal venous gradient). Higher values are defined as portal hypertension.
Etiology of Portal Hypertension
Portal hypertension results mainly from increased resistance to blood flow in the portal vein. A common cause of this resistance is disease within the liver; uncommon causes include blockage of the splenic or portal vein and impaired hepatic venous outflow (see table Most Common Causes of Portal Hypertension). Increased flow volume is a rare cause, although it often contributes to portal hypertension in cirrhosis and in hematologic disorders that cause massive splenomegaly.
Most Common Causes of Portal Hypertension
Mechanism or Location | Cause |
|---|---|
Prehepatic | |
Obstruction | Splenic or portal vein thrombosis |
Increased portal flow (rare) | Massive splenomegaly caused by a primary hematologic disorder |
Hepatic | |
Presinusoidal | Idiopathic portal hypertension Other periportal disorders (eg, primary biliary cholangitis, sarcoidosis, congenital hepatic fibrosis) |
Sinusoidal | Cirrhosis (all etiologies) |
Postsinusoidal | Hepatic sinusoidal obstruction syndrome (hepatic veno-occlusive disease) |
Posthepatic | |
Obstruction | Hepatic vein thrombosis (Budd-Chiari syndrome) Obstruction of the inferior vena cava |
Resistance to right heart filling | Constrictive pericarditis |
Pathophysiology of Portal Hypertension
In cirrhosis, tissue fibrosis and regeneration increase resistance in the sinusoids and terminal portal venules. However, other potentially reversible factors contribute; they include contractility of sinusoidal lining cells, production of vasoactive substances (eg, endothelins, nitric oxide), various systemic mediators of arteriolar resistance, and possibly swelling of hepatocytes.
Over time, portal hypertension creates portosystemic venous collaterals. They may slightly decrease portal vein pressure but can cause complications. Engorged serpentine submucosal vessels (varices) in the distal esophagus and sometimes in the gastric fundus can rupture, causing sudden, catastrophic gastrointestinal bleeding. Bleeding rarely occurs unless the portal pressure gradient is > 12 mm Hg. Gastric mucosal vascular congestion (portal hypertensive gastropathy) can cause acute or chronic bleeding independent of varices. Visible abdominal wall collaterals are common; veins radiating from the umbilicus (caput medusae) are much rarer and indicate extensive flow in the umbilical and periumbilical veins. Collaterals around the rectum can cause rectal varices that can bleed.
Portosystemic collaterals shunt blood away from the liver. Thus, less blood reaches the liver when portal flow increases (diminished hepatic reserve). In addition, toxic substances from the intestine are shunted directly to the systemic circulation, contributing to portosystemic encephalopathy. Venous congestion within visceral organs due to portal hypertension contributes to ascites via altered Starling forces. Splenomegaly and hypersplenism commonly occur as a result of increased splenic vein pressure. Thrombocytopenia, leukopenia, and, less commonly, hemolytic anemia may result.
Portal hypertension is often associated with a hyperdynamic circulation. Mechanisms are complex and seem to involve altered sympathetic tone, production of nitric oxide and other endogenous vasodilators, and enhanced activity of humoral factors (eg, glucagon).
Symptoms and Signs of Portal Hypertension
Portal hypertension is asymptomatic; symptoms and signs result from its complications. The most dangerous is acute variceal bleeding. Patients typically present with sudden painless upper gastrointestinal bleeding, often massive. Bleeding from portal hypertensive gastropathy is often subacute or chronic. Ascites, splenomegaly, or portosystemic encephalopathy may be present.
Diagnosis of Portal Hypertension
Usually clinical evaluation
Portal hypertension is assumed to be present when a patient with chronic liver disease has collateral circulation, splenomegaly, ascites, or portosystemic encephalopathy. Proof requires measurement of the hepatic venous pressure gradient, which approximates portal pressure, by a transjugular catheter; however, this procedure is invasive and usually not done. Imaging may help when cirrhosis is suspected. Ultrasonography or CT often reveals dilated intra-abdominal collaterals, and Doppler ultrasonography can determine portal vein patency and flow.
Esophagogastric varices and portal hypertensive gastropathy are best diagnosed by endoscopy, which may also identify predictors of esophagogastric variceal bleeding (eg, red markings on a varix).
Treatment of Portal Hypertension
Ongoing endoscopic therapy and surveillance
Nonselective beta-blockers with or without isosorbide mononitrateNonselective beta-blockers with or without isosorbide mononitrate
Sometimes portal vein shunting
When possible, the underlying disorder is treated.
In patients with esophagogastric varices that have bled, combined endoscopic and drug treatment decreases mortality and reduces risk of rebleeding better than either therapy used alone. A series of endoscopic banding sessions are done to obliterate residual varices, then periodic endoscopic surveillance is done to identify and treat recurrent varices. Long-term drug therapy usually involves nonselective beta-blockers; these drugs lower portal pressure primarily by diminishing portal flow, although the effects vary. Agents include propranolol (40 to 80 mg orally twice a day), nadolol (40 to 160 mg orally once a day), timolol (10 to 20 mg orally twice a day), and carvedilol (6.25 to 12.5 mg orally twice a day), with dosage titrated to decrease heart rate by about 25%. Adding isosorbide mononitrate 10 to 20 mg orally twice a day may further reduce portal pressure (In patients with esophagogastric varices that have bled, combined endoscopic and drug treatment decreases mortality and reduces risk of rebleeding better than either therapy used alone. A series of endoscopic banding sessions are done to obliterate residual varices, then periodic endoscopic surveillance is done to identify and treat recurrent varices. Long-term drug therapy usually involves nonselective beta-blockers; these drugs lower portal pressure primarily by diminishing portal flow, although the effects vary. Agents include propranolol (40 to 80 mg orally twice a day), nadolol (40 to 160 mg orally once a day), timolol (10 to 20 mg orally twice a day), and carvedilol (6.25 to 12.5 mg orally twice a day), with dosage titrated to decrease heart rate by about 25%. Adding isosorbide mononitrate 10 to 20 mg orally twice a day may further reduce portal pressure (1).
In patients with esophagogastric varices that have not yet bled (ie, for primary prophylaxis), outcomes are similar with beta blocker therapy or endoscopic therapy.
Patients who do not adequately respond to either treatment should be considered for transjugular intrahepatic portosystemic shunting (TIPS) or, less frequently, a surgical portacaval shunt. In TIPS, the shunt is created by placing a stent between the portal and hepatic venous circulation within the liver. (See also the American Association for the Study of Liver Diseases [AASLD] practice guideline The Role of Transjugular Intrahepatic Portosystemic Shunt [TIPS] in the Management of Portal Hypertension: Update 2009.) Although TIPS may result in fewer immediate deaths than surgical shunting, particularly during acute bleeding, maintenance of patency may require repeat procedures because the stent may become stenosed or occluded over time. Long-term benefits are unknown. Liver transplantation may be indicated for some patients.
For bleeding due to portal hypertensive gastropathy, beta blockers can be used to decrease portal pressure. A shunt should be considered if drugs are ineffective, but results may be less successful than for esophagogastric variceal bleeding.
Because it rarely causes clinical problems, hypersplenism requires no specific treatment, and splenectomy should be avoided.
Treatment reference
1. Albillos A, Zamora J, Martínez J, et al: Stratifying risk in the prevention of recurrent variceal hemorrhage: Results of an individual patient meta-analysis. Hepatology 66:1219-1231, 2017.
Prognosis for Portal Hypertension
Mortality during acute variceal hemorrhage may exceed 50%. Prognosis is predicted by the degree of hepatic reserve and the degree of bleeding. For survivors, the bleeding risk within the next 1 to 2 years is 50 to 75%. Ongoing endoscopic or drug therapy lowers the bleeding risk but decreases long-term mortality only marginally. For treatment of acute bleeding, Overview of Gastrointestinal Bleeding and Varices: Treatment.
Key Points
Portal hypertension is caused most often by cirrhosis (in Europe and North America), schistosomiasis (in endemic areas), or hepatic vascular abnormalities.
Complications can include acute variceal bleeding (with a high mortality rate), ascites, splenomegaly, and portosystemic encephalopathy.
Diagnose portal hypertension based on clinical findings.
To help prevent acute variceal bleeding, initiate periodic surveillance and endoscopic banding sessions.
To help prevent rebleeding, treat with nonselective beta-blockers with or without isosorbide mononitrate, transjugular intrahepatic portosystemic shunting (TIPS), or both. To help prevent rebleeding, treat with nonselective beta-blockers with or without isosorbide mononitrate, transjugular intrahepatic portosystemic shunting (TIPS), or both.







