


Ankylosing spondylitis is the prototypical spondyloarthropathy and a systemic disorder characterized by inflammation of the axial skeleton, large peripheral joints, and digits; nocturnal back pain; morning back stiffness; accentuated kyphosis; constitutional symptoms; aortitis; cardiac conduction abnormalities; and anterior uveitis. Diagnosis requires showing sacroiliitis on imaging or spine inflammation using MRI. Treatment is with nonsteroidal anti-inflammatory drugs (NSAIDs) and/or tumor necrosis factor inhibitors or interleukin-17 (IL-17) inhibitors and physical measures that maintain joint flexibility.
Ankylosing spondylitis is 3 times more frequent in men than in women and begins most often between ages 20 and 40. It is 10 to 20 times more common among first-degree relatives of patients with ankylosing spondylitis than in the general population. The human leukocyte antigen B27 (HLA-B27) allele is present in 90% of White patients with ankylosing spondylitis (1), but it is also present in up to 10% of the general population depending on ethnicity. The risk of ankylosing spondylitis in first-degree relatives with the HLA-B27 allele is approximately 20%. Increased prevalence of HLA-B27 in White people or HLA-B7 in Black people supports a genetic predisposition. However, the concordance rate in identical twins is only approximately 50%, suggesting that environmental factors contribute.
Reference
1. Khan MA, Braun WE, Kushner I, et al: HLA B27 in Ankylosing Spondylitis: Differences in Frequency and Relative Risk in American Blacks and Caucasians. J Rheumatol. 2023;50(1):39-43.
Classification of Ankylosing Spondylitis
Most patients have predominantly axial involvement (called axial ankylosing spondylitis). Some have predominately peripheral involvement. Among those with axial involvement, some have no evidence of sacroiliitis on radiographs. Thus, some experts have classified ankylosing spondylitis as follows:
Axial ankylosing spondylitis: Has predominantly axial involvement and findings typical of bilateral sacroiliitis on imaging
Nonradiographic ankylosing spondylitis: Clinically similar to axial ankylosing spondylitis but without findings typical of sacroiliitis on imaging
Peripheral ankylosing spondylitis: Ankylosing spondylitis with predominantly peripheral joint involvement
Symptoms and Signs of Ankylosing Spondylitis
The most frequent manifestation of ankylosing spondylitis is inflammatory back pain, but disease can begin in peripheral joints, especially in children and women, and rarely with acute iridocyclitis (iritis, anterior uveitis). Other early symptoms and signs are diminished chest expansion from diffuse costovertebral involvement, and occasionally fatigue, anorexia, weight loss, and anemia.


ST. BARTHOLOMEW'S HOSPITAL, LONDON/SCIENCE PHOTO LIBRARY
Back pain—often nocturnal and of varying intensity—eventually becomes recurrent. Morning stiffness, typically relieved by activity, and paraspinal muscle spasm develop. A flexed or bent-over posture eases back pain and paraspinal muscle spasm; thus, kyphosis is common in untreated patients. Severe hip and shoulder arthritis can eventually develop. In late stages, untreated patients may develop accentuated kyphosis, loss of lumbar lordosis, and fixed bent-forward posturing, with compromised pulmonary function and an inability to lie flat. There may be peripheral potentially deforming joint involvement, sometimes involving isolated digit diffuse swelling (dactylitis). Achilles and patellar tendinitis can occur.
Systemic manifestations of ankylosing spondylitis occur in approximately 25% of patients (1). Recurrent, acute anterior uveitis is common; less commonly it becomes protracted and severe enough to impair vision. Neurologic signs occasionally result from compression radiculitis or sciatica, vertebral fracture or subluxation, or cauda equina syndrome. Cardiovascular manifestations include aortic insufficiency, aortitis, angina, pericarditis, and cardiac conduction abnormalities (which may be asymptomatic). Dyspnea, cough, or hemoptysis can rarely result from nontuberculous fibrosis or cavitation of an upper lobe of the lung; cavitary lesions can become secondarily infected with Aspergillus. Nonspecific colitis has been noted in 30% of patients with ankylosing spondylitis. Subcutaneous nodules, like those in patients with rheumatoid arthritis, do not develop in patients with ankylosing spondylitis.
Symptoms and signs reference
1. Stolwijk C, van Tubergen A, Castillo-Ortiz JD, Boonen A: Prevalence of extra-articular manifestations in patients with ankylosing spondylitis: a systematic review and meta-analysis. Ann Rheum Dis 74(1):65-73, 2015. doi:10.1136/annrheumdis-2013-203582
Diagnosis of Ankylosing Spondylitis
Lumbosacral spine and sacroiliac joint radiography
Blood tests (erythrocyte sedimentation rate, C-reactive protein, human leukocyte antigen B27 [HLA-B27], and complete blood count) or explicit clinical criteria (Assessment of SpondyloArthritis international Society criteria)
Pelvic/spine MRI in select patients
Ankylosing spondylitis should be suspected in patients, particularly young men, with nocturnal back pain plus prolonged morning stiffness and kyphosis, diminished chest expansion, Achilles or patellar tendinitis, or unexplained anterior uveitis. A first-degree relative with ankylosing spondylitis should raise suspicion.

ST. BARTHOLOMEW'S HOSPITAL, LONDON/SCIENCE PHOTO LIBRARY
Patients should generally be tested with erythrocyte sedimentation rate, C-reactive protein, and complete blood count. Rheumatoid factor (RF), anti-anticyclic citrullinated peptide [CCP] antibodies, and antinuclear antibodies are needed only if peripheral arthritis suggests other diagnoses. The HLA-B27 allele is present in 90% of White patients with ankylosing spondylitis, but it is also present in up to 10% of the general population depending on ethnicity (1). No laboratory test is diagnostic, but results can increase suspicion for the disorder or rule out other disorders that can simulate ankylosing spondylitis. If, after these tests, ankylosing spondylitis is still suspected, patients should undergo radiography or MRI of the lumbosacral spine and sacroiliac joints; demonstration of sacroiliitis on radiograph strongly supports the diagnosis.
Some patients should undergo pelvic MRI to look for sacroiliitis that is not seen on radiographs. In these patients, MRI shows osteitis or early erosions.


DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Although there are several existing diagnostic criteria for patients with suspected ankylosing spondylitis, the Assessment of SpondyloArthritis international Society (ASAS) criteria (2, 3, 4) are most often applied. They are useful in diagnosing patients earlier in the disease process, particularly those without spondyloarthritis on imaging. The ASAS criteria for axial spondyloarthritis are applied to patients who have had back pain for > 3 months and who are < 45 years of age at onset.
Diagnosis can be done using ASAS imaging or clinical criteria. To fulfill the imaging criteria, patients must have radiographic or MRI evidence of sacroiliitis plus at least 1 spondyloarthritis feature. To fulfill the clinical criteria, patients must have HLA-B27 plus at least 2 separate spondyloarthritis features. ASAS spondyloarthritis features include the following:
Dactylitis
Enthesitis of the heel
Family history of spondyloarthritis
History of inflammatory back pain
Arthritis
Presence of HLA-B27
Elevated C-reactive protein
Good response to nonsteroidal anti-inflammatory drugs
Historical features that distinguish inflammatory back pain from noninflammatory back pain include onset at ≤ 40 years, gradual onset, morning stiffness, improvement with activity, and duration of symptoms ≥ 3 months before seeking medical attention.
Erythrocyte sedimentation rate and other acute-phase reactants (eg, C-reactive protein) are inconsistently elevated in patients with active ankylosing spondylitis. Tests for RF and antinuclear antibodies are negative. The HLA-B27 genetic marker is minimally helpful because positive and negative predictive values are low.
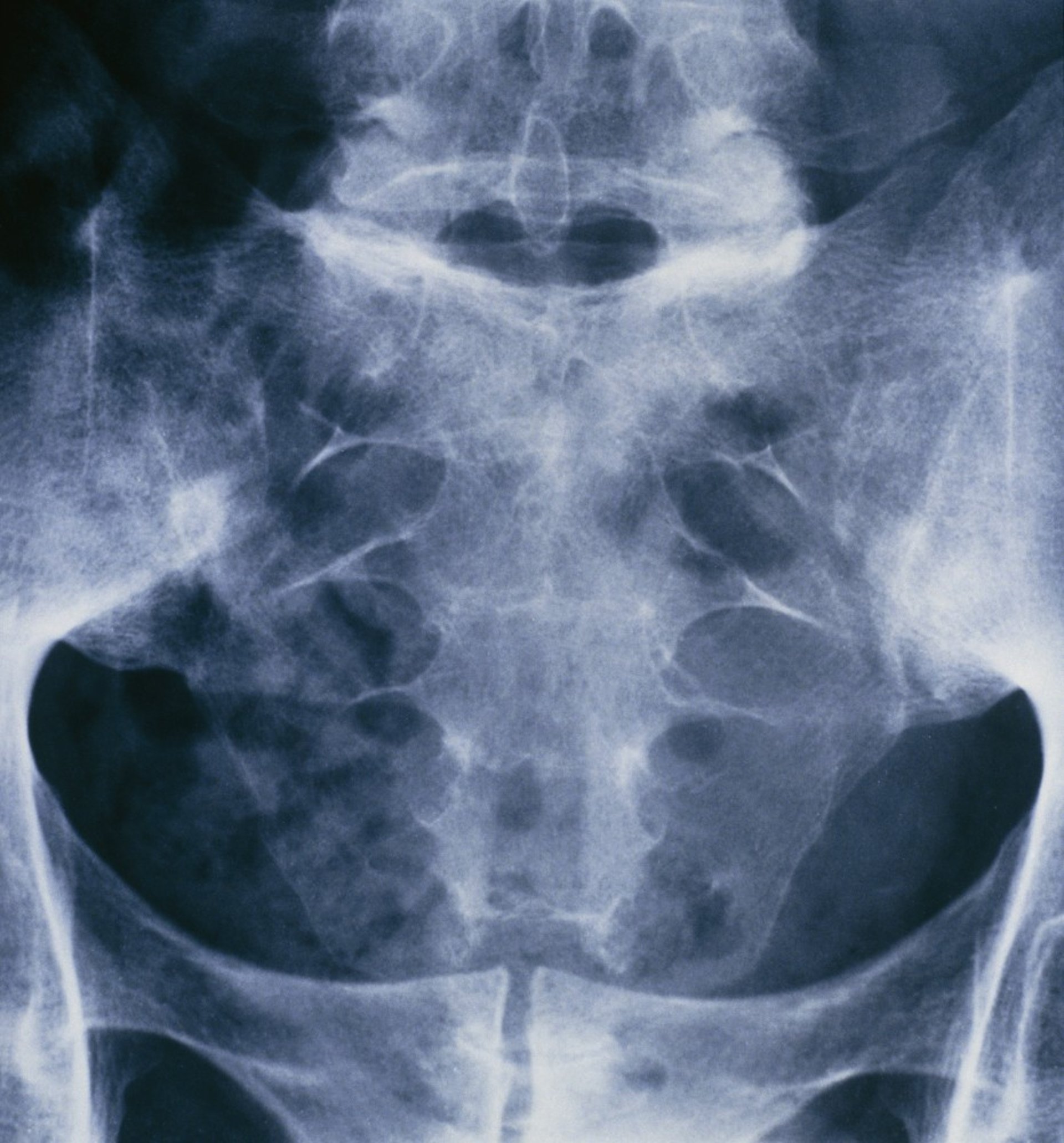
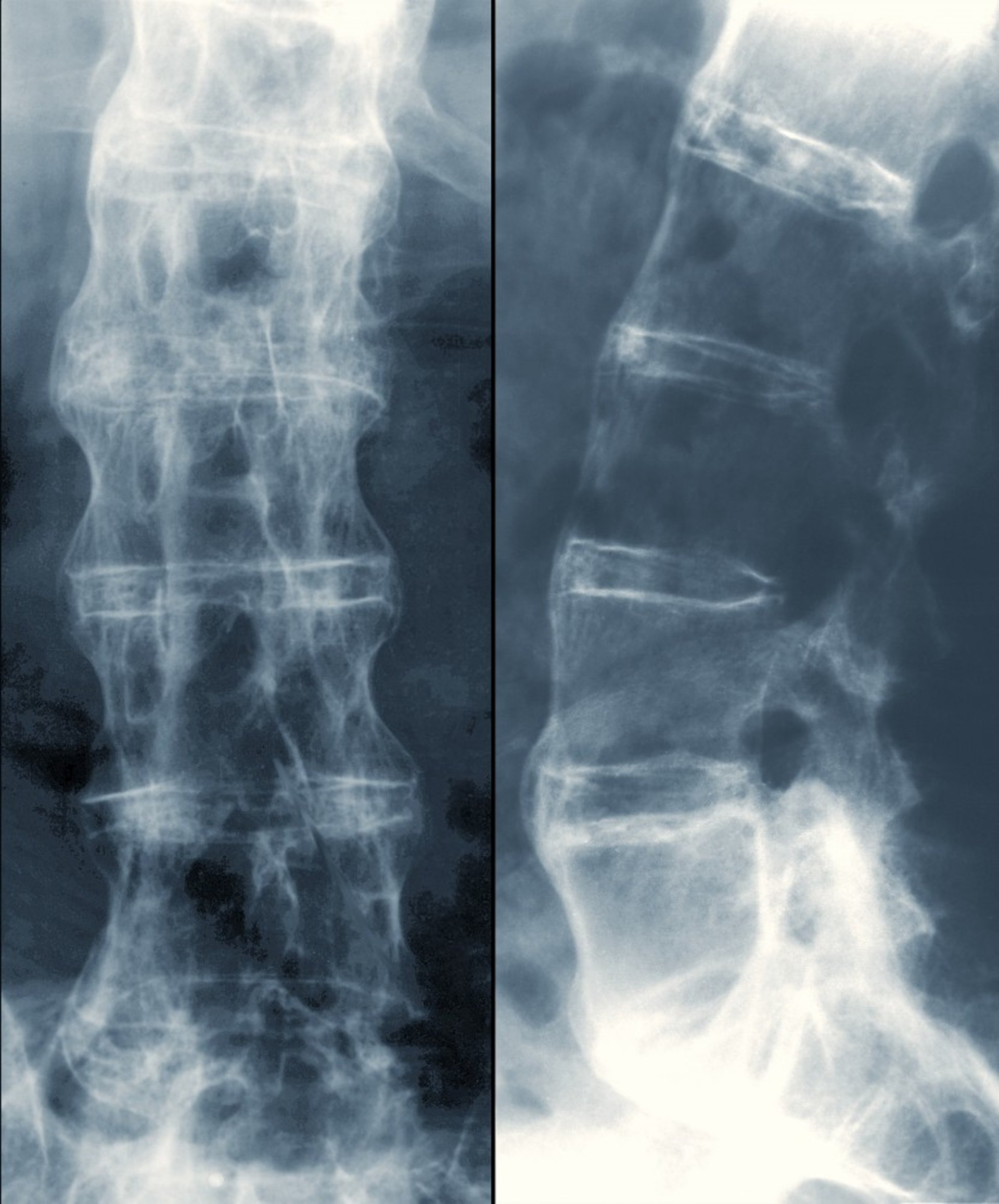
The earliest abnormalities on radiographs are pseudo-widening caused by subchondral erosions, followed by sclerosis or later narrowing and eventually fusion in the sacroiliac joints. Changes are symmetric. Early changes in the spine are upper lumbar vertebral squaring with sclerosis at the corners (shiny corner sign), spotty ligamentous calcification, and 1 or 2 evolving syndesmophytes. Late changes result in a “bamboo spine” appearance, resulting from prominent syndesmophytes, diffuse paraspinal ligamentous calcification, and osteoporosis; these changes develop in some patients on average over 10 years.

ZEPHYR/SCIENCE PHOTO LIBRARY


By permission of the publisher. From Asim Khan M: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
Changes typical of ankylosing spondylitis may not become visible on radiographs for years. MRI shows changes earlier, but there is no consensus regarding its role in routine diagnosis given the lack of prospective, validated data in regard to its diagnostic utility. Pelvic MRI should be done if the index of suspicion of spondyloarthritis is high or if there is a need to rule out other causes of the patient's symptoms. MRI shows early inflammatory changes, bone marrow edema on T2-weighted images with fatty changes, and subtle structural abnormalities. Lastly, routine monitoring of radiographic changes with serial spine radiographs is not recommended.
Differential diagnosis of ankylosing spondylitis
Mechanical back pain: A herniated intervertebral disk can cause back pain and radiculopathy similar to ankylosing spondylitis, but the pain is limited to the spine and nerve roots, usually causes more sudden symptoms, and causes no systemic manifestations or laboratory test abnormalities. If necessary, CT or MRI can differentiate it from ankylosing spondylitis. Involvement of a single sacroiliac joint suggests a different spondyloarthropathy or possibly infection. Tuberculous spondylitis can simulate ankylosing spondylitis (see tuberculosis of bones and joints).


Image provided by Roy Altman, MD.


Image courtesy of Kinanah Yaseen, MD.
Diffuse idiopathic skeletal hyperostosis (DISH): DISH occurs primarily in men > 50 years and may resemble ankylosing spondylitis clinically and on radiograph. Patients uncommonly have spinal pain, stiffness, and insidious loss of motion. Radiographic findings in DISH include large ossifications anterior to spinal ligaments (the calcification appears as if someone poured candle wax in front and on the right side of the vertebrae), bridging several vertebrae (usually 4 vertebral bodies) and usually starting at the lower thoracic spine, eventually affecting the cervical and lumbar spine. There is often subperiosteal bone growth along the pelvic brim and at insertion of tendons (such as the Achilles tendon insertion). However, the anterior spinal ligament is intact and frequently bulging, and sacroiliac and spinal apophyseal joints are not eroded. Additional differentiating features of DISH are stiffness that is usually not markedly accentuated in the morning and a normal erythrocyte sedimentation rate.
Osteitis condensans ilii: Generally, osteitis condensans ilii manifests as sclerotic triangles on the iliac side of lower third of the sacroiliac joint in young multiparous females without any bony erosions. This radiographic finding does not require treatment. In general, the HLA-B27 allele is not present in patients with osteitis condensans ilii.
Diagnosis references
1. Khan MA, Braun WE, Kushner I, et al: HLA B27 in Ankylosing Spondylitis: Differences in Frequency and Relative Risk in American Blacks and Caucasians. J Rheumatol. 2023;50(1):39-43.
2. Sieper J, Rudwaleit M, Baraliakos X, et al: The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis 68 Suppl 2:ii1-ii44, 2009. doi:10.1136/ard.2008.104018
3. Sepriano A, Landewé R, van der Heijde D, et al: Predictive validity of the ASAS classification criteria for axial and peripheral spondyloarthritis after follow-up in the ASAS cohort: A final analysis. Ann Rheum Dis 75(6):1034–1042, 2016. doi: 10.1136/annrheumdis-2015-208730
4. Sepriano A, Rubio R, Ramiro S, et al: Performance of the ASAS classification criteria for axial and peripheral spondyloarthritis: A systematic literature review and meta-analysis. Ann Rheum Dis 76(5):886–890, 2017. doi: 10.1136/annrheumdis-2016-210747
Treatment of Ankylosing Spondylitis
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Exercises and supportive measures
The goals of treatment are relieving pain, maintaining joint range of motion, and preventing end-organ damage. Because the condition may cause lung fibrosis, cigarette smoking is discouraged. (See also ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update.)
NSAIDs are first-line therapy for most patients. They reduce pain and suppress joint inflammation and muscle spasm, thereby increasing range of motion, which facilitates exercise and prevents contractures. Most NSAIDs work in ankylosing spondylitis, and tolerance and toxicity dictate drug choice. The daily dose of NSAIDs should be as low as possible, but maximum doses may be needed with active disease. Medication withdrawal should be attempted only slowly, after systemic and joint signs of active disease have been suppressed for several months.
Candida, diarrhea, herpes zoster, and worsening symptoms of inflammatory bowel disease.
Tapering of therapy rather than discontinuation can be considered in patients with sustained remission.
For proper posture and joint motion, daily exercise and other supportive measures (eg, postural training, therapeutic exercise) are vital to strengthen muscle groups that oppose the direction of potential deformities (ie, the extensor rather than flexor muscles). Reading while lying prone and pushing up on the elbows or pillows and thus extending the back may help keep the back flexible. Because chest wall motion can be restricted, which impairs lung function, cigarette smoking, which also impairs lung function, is strongly discouraged.
Intra-articular depot corticosteroids may be beneficial, particularly when 1 or 2 peripheral joints are more severely inflamed than others, thereby compromising exercise and rehabilitation. Imaging-guided corticosteroid injections (eg, with fluoroscopy or ultrasound) into the sacroiliac joints may occasionally help severe sacroiliitis.
If severe hip arthritis develops, total hip arthroplasty may lessen pain and improve flexibility dramatically; although there may be a small but increased incidence of postoperative heterotopic ossification after joint replacement.
Prognosis for Ankylosing Spondylitis
Ankylosing spondylitis is characterized by mild or moderate flares of active inflammation alternating with periods of little or no inflammation. Proper treatment in most patients results in minimal or no disability and in a full, productive life despite back stiffness. Occasionally, the course is severe and progressive, resulting in pronounced incapacitating deformities.
Poor prognostic factors include persistently high erythrocyte sedimentation rate and C-reactive protein, hip involvement, poor response to NSAIDs, presence of anterior uveitis, or heart or pulmonary disease.
Key Points
Ankylosing spondylitis is a systemic disorder that affects axial and peripheral joints and can cause constitutional symptoms, cardiac symptoms, and anterior uveitis (iritis).
Initial manifestation is usually inflammatory back pain and stiffness sometimes along with peripheral joint symptoms and/or anterior uveitis.
Diagnose based on the results of lumbosacral spine imaging, sacroiliac joint imaging, pelvic MRI, blood tests (erythrocyte sedimentation rate, C-reactive protein, and complete blood count), and/or explicit clinical criteria.
Use nonsteroidal anti-inflammatory drugs to help reduce symptom severity and improve function.
Use tumor necrosis factor (TNF) inhibitors, interleukin-17 (IL-17) inhibitors, or Janus kinase (JAK) inhibitors in patients who respond inadequately to NSAIDs.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.







