


Intussusception is telescoping of one portion of the intestine (intussusceptum) into an adjacent segment (intussuscipiens), causing intestinal obstruction and sometimes intestinal ischemia. Diagnosis is by ultrasonography. Treatment is with an air enema (for the most common type of intussusception, the ileocolic type) and sometimes surgery.
Intussusception generally occurs between 6 months and 3 years of age, with most cases occurring before age 1 and 70% occurring before age 2 (1). It is the most common cause of intestinal obstruction in this age group and occurs roughly equally in male and female children < 4 years of age. In children > 4 years of age, intussusception is much more common in males.
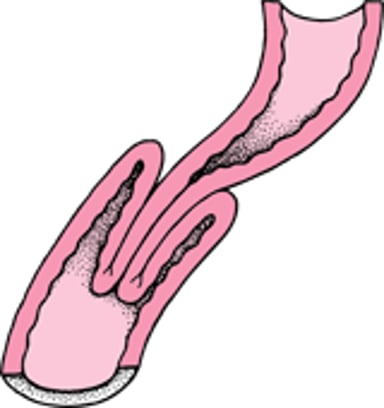
The telescoping segment obstructs the intestine and, if not treated, ultimately impairs blood flow to the intussuscepting segment (see figure Intussusception), causing ischemia, gangrene, and perforation.
Intussusception

Reference
1. Marsicovetere P, Ivatury SJ, White B, Holubar SD: Intestinal Intussusception: Etiology, Diagnosis, and Treatment. Clin Colon Rectal Surg 30(1):30-39, 2017. doi: 10.1055/s-0036-1593429
Etiology of Intussusception
Most cases are idiopathic. The most common type of intussusception is the ileocolic type.
In about 25% of children who have intussusception, typically very young and older children, a lead point (ie, a mass or other intestinal abnormality) triggers the telescoping. Examples include polyps, lymphoma, Meckel diverticulum, and immunoglobulin A–associated vasculitis (formerly called Henoch-Schönlein purpura) when purpura involve the bowel wall. Cystic fibrosis is also a risk factor.
Symptoms and Signs of Intussusception
The initial symptoms of intussusception are sudden onset of significant, colicky abdominal pain that recurs every 15 to 20 minutes, often with vomiting. The child appears relatively well between episodes.
Later, as intestinal ischemia develops, pain becomes steady, the child becomes lethargic, and mucosal hemorrhage causes heme-positive stool on rectal examination and sometimes spontaneous passage of a currant-jelly stool. The latter, however, is a late occurrence, and physicians should not wait for this symptom to occur to suspect intussusception. A palpable abdominal mass, described as sausage-shaped, is sometimes present. Perforation results in signs of peritonitis, with significant tenderness, guarding, and rigidity. Pallor, tachycardia, and diaphoresis indicate shock.
About 5 to 10% of children present without the colicky pain phase. Instead, they appear lethargic, as if drugged (atypical or apathetic presentation). In such cases, the diagnosis of intussusception is often missed until the currant-jelly stool appears or an abdominal mass is palpated.
Diagnosis of Intussusception
Ultrasonography
Suspicion of the diagnosis must be high, particularly in children with atypical presentation, and studies and intervention must be done urgently, because survival and likelihood of nonoperative reduction decrease significantly with time.
Approach depends on clinical findings. Ill children with signs of peritonitis require fluid resuscitation
Barium enema was once the preferred initial study because it revealed the classic coiled-spring appearance around the intussusceptum. In addition to being diagnostic, barium enema was also usually therapeutic; the pressure of the barium often reduced the telescoped segments. However, barium occasionally enters the peritoneum through a clinically unsuspected perforation and causes significant peritonitis. Currently, ultrasonography is the preferred means of diagnosis; it is easily done, relatively inexpensive, and safe; the characteristic finding is termed the target sign.
At times, an intussusception is seen incidentally on an imaging study, such as a CT scan. If children have no symptoms of intussusception, they can be closely followed, and intervention may be delayed or in some cases unnecessary.
Pearls & Pitfalls
|
Treatment of Intussusception
Air enema
Surgery if enema unsuccessful or if perforation present
If ileocolic intussusception is confirmed, an air enema is used for reduction, which lessens the likelihood and consequences of perforation. The intussusceptum can be successfully reduced in 75 to 95% of children. If the air enema is successful, children are observed overnight to rule out occult perforation. If reduction is unsuccessful or if the intestine has perforated, immediate surgery is required.
When reduction is achieved without surgery, the recurrence rate is 5 to 10%.
Key Points
Intussusception is telescoping of one segment of intestine into another, usually in children < 3 years of age.
The most common type of intussusception is ileocolic.
Children typically present with colicky abdominal pain and vomiting, followed by passage of currant-jelly stool.
Diagnosis is best made by ultrasonography.
Treatment is reduction by air enema and sometimes surgery.







