



Croup is acute inflammation of the upper and lower respiratory tracts most commonly caused by parainfluenza virus type 1 infection. It is characterized by a brassy, barking cough and inspiratory stridor. Diagnosis is usually obvious clinically but can be made by anteroposterior neck radiograph. Treatment is antipyretics, hydration, nebulized racemic epinephrine, and corticosteroids. Prognosis is excellent.. It is characterized by a brassy, barking cough and inspiratory stridor. Diagnosis is usually obvious clinically but can be made by anteroposterior neck radiograph. Treatment is antipyretics, hydration, nebulized racemic epinephrine, and corticosteroids. Prognosis is excellent.


")
")
Croup affects mainly children aged 6 months to 3 years.
Etiology of Croup
The most common pathogens are
Parainfluenza viruses, especially type 1
Less common causes are respiratory syncytial virus (RSV) and adenovirus followed by influenza viruses A and B, enterovirus, rhinovirus, measles virus, and Mycoplasma pneumoniae. Croup caused by influenza may be particularly severe and may occur in a broader age range of children.
Seasonal outbreaks are common. Cases caused by parainfluenza viruses tend to occur in the fall; those caused by RSV and influenza viruses tend to occur in the winter and spring. Spread is usually through the air or by contact with infected secretions.
Pathophysiology of Croup
The infection causes inflammation of the larynx, trachea, bronchi, bronchioles, and sometimes lung parenchyma. Obstruction caused by swelling and inflammatory exudates develops and becomes pronounced in the subglottic region. Obstruction increases the work of breathing; rarely, tiring results in hypercapnia. Atelectasis may occur concurrently if the bronchioles become obstructed.
Symptoms and Signs of Croup
Croup is usually preceded by upper respiratory infection symptoms. A barking, often spasmodic, cough and hoarseness then occur, commonly at night; inspiratory stridor may be present as well. The child may awaken at night with respiratory distress, tachypnea, and retractions. In severe cases, cyanosis with increasingly shallow respirations may develop as the child tires.

The obvious respiratory distress and harsh inspiratory stridor are the most dramatic physical findings. Auscultation reveals prolonged inspiration and stridor. Crackles also may be present, indicating lower airway involvement. Breath sounds may be diminished with atelectasis.
Fever is present in about half of children. The child’s condition may seem to improve in the morning but worsen again at night.
Recurrent episodes are often called spasmodic croup. Allergy or airway reactivity may play a role in spasmodic croup, but the clinical manifestations cannot be differentiated from those of viral croup. Also, spasmodic croup usually is initiated by a viral infection; however, fever is typically absent.
Diagnosis of Croup
Clinical presentation (eg, barking cough, inspiratory stridor)
Anteroposterior (AP) and lateral neck radiographs as needed
Diagnosis of croup is usually obvious by the barking nature of the cough.
Similar inspiratory stridor can result from epiglottitis, bacterial tracheitis, airway foreign body, diphtheria, and retropharyngeal abscess. Epiglottitis, retropharyngeal abscess, and bacterial tracheitis have a more rapid onset and cause a more toxic appearance, odynophagia, and fewer upper respiratory tract symptoms. A foreign body may cause respiratory distress and a typical croupy cough, but fever and a preceding upper respiratory infection are usually absent. Diphtheria is excluded by a history of adequate immunization and is confirmed by identification of the organism in cultures of scrapings from a typical grayish diphtheritic membrane.

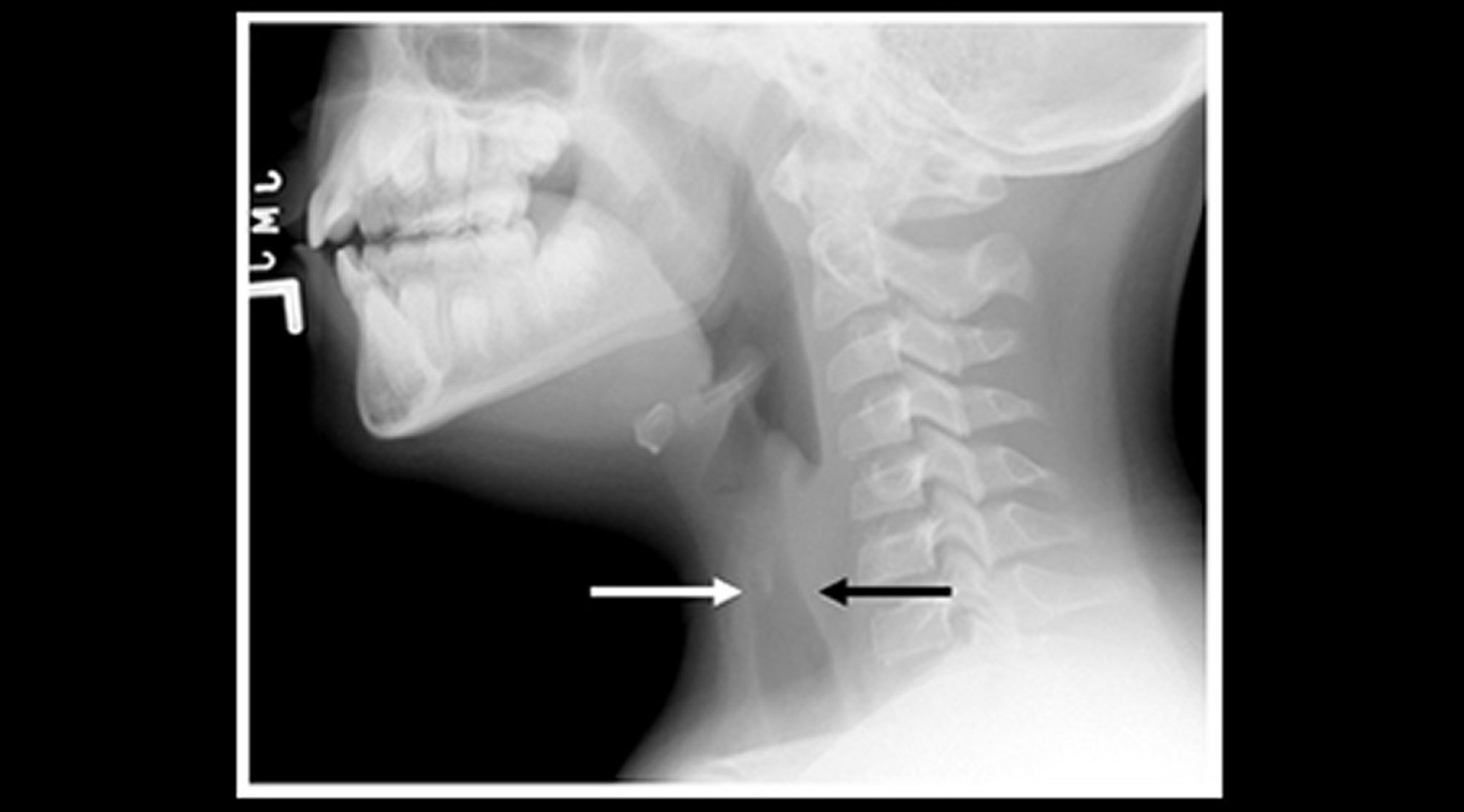
Image courtesy of John McBride, MD.
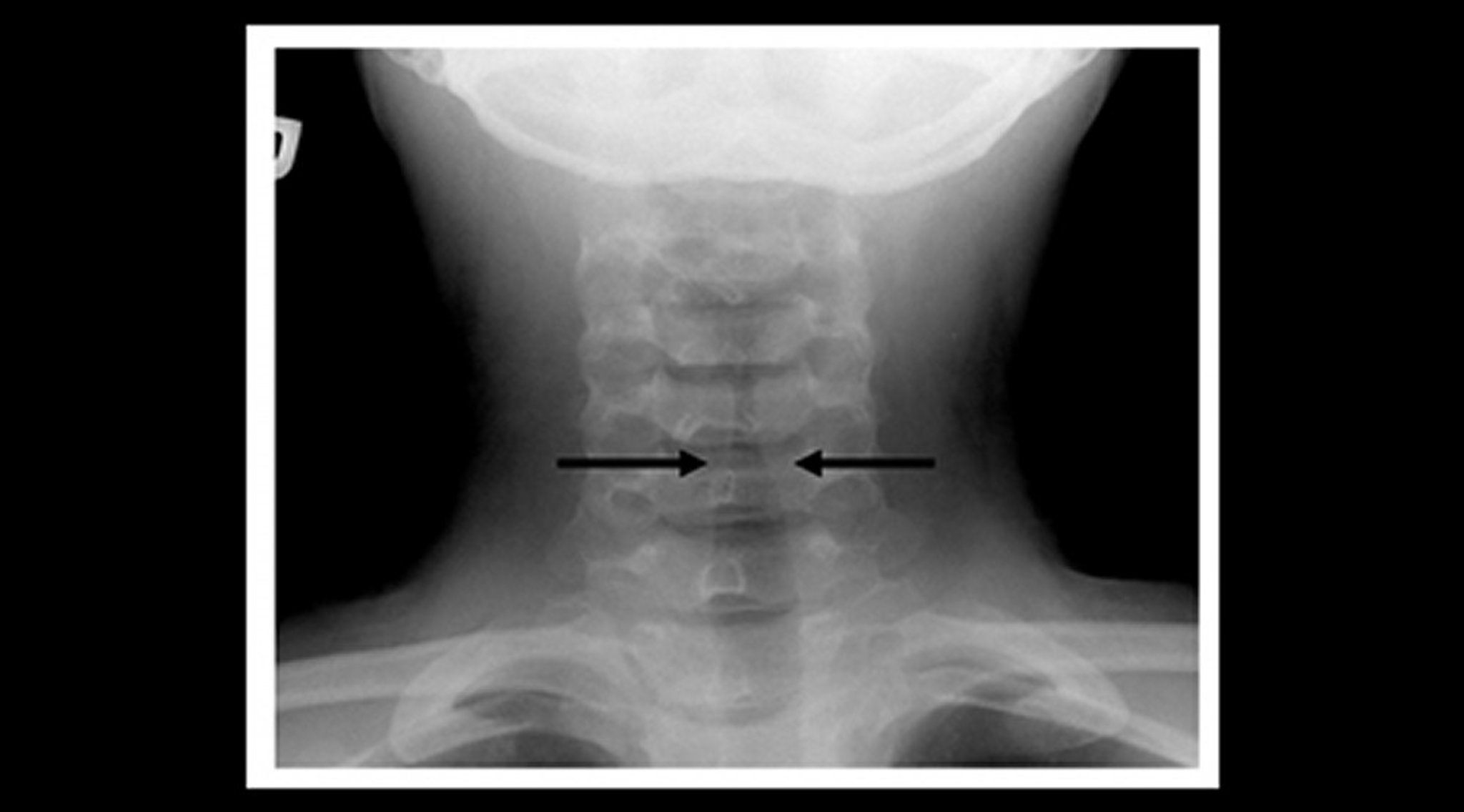
Image courtesy of John McBride, MD.
If the diagnosis is unclear, patients should have AP and lateral radiographs of the neck and chest; subepiglottic narrowing (steeple sign) seen on AP neck radiograph supports the diagnosis. Seriously ill patients, in whom epiglottitis is a concern, should be examined in the operating room by appropriate specialists able to establish an airway (see Treatment of Epiglottitis). Patients should have pulse oximetry, and those with respiratory distress may have arterial blood gas measurement.
Pearls & Pitfalls
|
Treatment of Croup
For outpatients, cool humidified air and possibly a single dose of a long-acting corticosteroid
For inpatients, humidified oxygen, racemic epinephrine, and corticosteroidsFor inpatients, humidified oxygen, racemic epinephrine, and corticosteroids
The illness usually lasts 3 to 4 days and resolves spontaneously. A mildly ill child may be cared for at home with hydration and antipyretics. Keeping the child comfortable is important because fatigue and crying can aggravate the condition. Humidification devices (eg, cold-steam vaporizers or humidifiers) may ameliorate upper airway drying and are frequently used at home by families but have not been shown to alter the course of the illness. The vast majority of children with croup recover completely.
High-dose dexamethasone 0.6 mg/kg IM or orally once (maximum dose 10 mg) may benefit children early in the first 24 hours of the disease. It can help prevent hospitalization or help a child who is hospitalized with moderate to severe croup; hospitalized children who do not respond quickly may require several doses. The viruses that most commonly cause croup do not usually predispose to secondary bacterial infection, and antibiotics are rarely indicated.High-dose dexamethasone 0.6 mg/kg IM or orally once (maximum dose 10 mg) may benefit children early in the first 24 hours of the disease. It can help prevent hospitalization or help a child who is hospitalized with moderate to severe croup; hospitalized children who do not respond quickly may require several doses. The viruses that most commonly cause croup do not usually predispose to secondary bacterial infection, and antibiotics are rarely indicated.
Hospitalization is typically indicated for
Increasing or persistent respiratory distress
Tachycardia
Fatigue
Cyanosis or hypoxemia
Dehydration
Pulse oximetry is helpful for assessing and monitoring severe cases. If oxygen saturation falls below 92%, humidified oxygen should be given and arterial blood gases should be measured to assess CO2 retention. A 30 to 40% inspired oxygen concentration is usually adequate. CO2 retention (PaCO2 > 45 mm Hg) generally indicates fatigue and the need for endotracheal intubation, as does inability to maintain oxygenation.
Nebulized racemic epinephrine offers symptomatic relief and relieves fatigue. However, the effects are transient; the course of the illness, the underlying viral infection, and the PaO2 are not altered by its use. Tachycardia and other adverse effects may occur. This medication is recommended mainly for patients with moderate to severe croup. Nebulized racemic epinephrine offers symptomatic relief and relieves fatigue. However, the effects are transient; the course of the illness, the underlying viral infection, and the PaO2 are not altered by its use. Tachycardia and other adverse effects may occur. This medication is recommended mainly for patients with moderate to severe croup.
Key Points
Croup is an acute, viral, respiratory tract infection affecting infants age 6 to 36 months and is typically caused by parainfluenza viruses (mainly type 1).
A barking, often spasmodic cough and sometimes inspiratory stridor (caused by subglottic edema) are the most prominent symptoms; symptoms are often worse at night.
Diagnosis is usually clinical, but an anteroposterior radiograph of the neck and chest showing classic subepiglottic narrowing (steeple sign) supports the diagnosis.
Give cool, humidified air or oxygen, and sometimes corticosteroids and nebulized racemic epinephrine.Give cool, humidified air or oxygen, and sometimes corticosteroids and nebulized racemic epinephrine.







