


Acute pancreatitis is acute inflammation of the pancreas (and, sometimes, adjacent tissues). The most common triggers are gallstones and alcohol intake. The severity of acute pancreatitis is classified as mild, moderately severe, or severe based on the presence of local complications and transient or persistent organ failure. Diagnosis is based on clinical presentation, serum amylase and lipase levels, and imaging studies. Treatment is supportive with IV fluids, analgesics, and nutritional support. Although overall mortality of acute pancreatitis is low, morbidity and mortality are significant in severe cases.
(See also Overview of Pancreatitis.)
Acute pancreatitis is a common disorder and a major health care concern.
Etiology of Acute Pancreatitis
Most cases of acute pancreatitis cases are due to gallstones (40 to 70%) and alcohol consumption (25 to 35%) (1).
The remaining cases result from myriad causes (see table Some Causes of Acute Pancreatitis).
Some Causes of Acute Pancreatitis
Cause | Examples |
|---|---|
Medications | ACE inhibitors, asparaginase, azathioprine, 2´,3´-dideoxyinosine, furosemide, GLP-1 receptor agonists,6-mercaptopurine, pentamidine,sulfa medications, valproate |
Infectious | Coxsackievirus B, cytomegalovirus, mumps, hepatitis A, hepatitis E |
Inherited | Multiple known gene mutations, including a small percentage of patients with cystic fibrosis |
Mechanical/structural | Gallstones, endoscopic retrograde cholangiopancreatography (ERCP), trauma, pancreatic cancer or periampullary cancer, choledochal cyst, sphincter of Oddi stenosis, pancreas divisum |
Metabolic | Hypertriglyceridemia, hypercalcemia (including hyperparathyroidism), estrogen use associated with high lipid levels |
Toxins | Alcohol, methanol |
Other | Cigarette smoking, pregnancy, postrenal transplant, ischemia caused by hypotension or atheroembolism, tropical pancreatitis |
Gallstones
Gallstones are the most common etiology of acute pancreatitis.
The precise mechanism of gallstone pancreatitis is unknown but likely involves increased pressure in the pancreatic duct caused by obstruction at the ampulla secondary to a stone or edema caused by the passage of a stone. Ductal hypertension results in aberrant activation of digestive enzymes from acinar cells. The toxic effects of bile acid itself on acinar cells might also be a mechanism.
Gallstone pancreatitis is rare in pregnancy and occurs most commonly in the third trimester.
Alcohol
Alcohol intake is the second most common etiology of acute pancreatitis. The risk of developing pancreatitis increases with increasing doses of alcohol (≥ 4 to 7 drinks/day in men and ≥ 3 drinks/day in women); risk was once thought to increase proportionally to duration of alcohol consumption, but acute pancreatitis attacks may occur in susceptible patients after short periods of high alcohol intake. Low or moderate levels of alcohol consumption are associated with progression from acute to chronic pancreatitis. However, < 10% of patients with chronic alcohol consumption develop acute pancreatitis, suggesting additional triggers or cofactors are needed to precipitate pancreatitis.
Pancreatic acinar cells metabolize alcohol into toxic metabolites via both oxidative and nonoxidative pathways and exhibit effects that predispose the cells to autodigestive injury and predispose the pancreas to necrosis, inflammation, and cell death. These effects include increased enzyme content, destabilization of lysosomal and zymogen granules, sustained increase in calcium overload, and activation of pancreatic stellate cells. Another theory proposes that alcohol increases the propensity of formation of protein plugs within pancreatic ducts by altering the level of lithogenic proteins and increasing the viscosity of pancreatic secretions, causing obstruction, and, eventually, acinar atrophy.
Other causes
A number of genetic mutations predisposing to pancreatitis have been identified. An autosomal dominant mutation of the cationic trypsinogen gene causes pancreatitis in 80% of carriers; an obvious familial pattern is present. Other mutations have lesser penetrance and are not readily apparent clinically except through genetic testing. The gene that causes cystic fibrosis increases the risk of recurrent acute pancreatitis as well as chronic pancreatitis.
Acute pancreatitis is a complication that develops after endoscopic retrograde cholangiopancreatography (ERCP) in about 5 to 8% of patients and may be as high as 16.5% based on an inpatient data base (2). Most events are of mild-to-moderate severity (3, 4).
Etiology references
1. Tenner S, Baillie J, DeWitt J, et al: American College of Gastroenterology guideline: Management of acute pancreatitis. Am J Gastroenterol 108(9):1400-1415; 1416, 2013. doi: 10.1038/ajg.2013.218
2. Kröner PT, Bilal M, Samuel R, et al: Use of ERCP in the United States over the past decade. Endosc Int Open 8(6):E761-E769, 2020. doi: 10.1055/a-1134-4873
3. Andriulli A, Loperfido S, Napolitano G, et al: Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol 102(8):1781-1788, 2007. doi: 10.1111/j.1572-0241.2007.01279.x
4. Kochar B, Akshintala VS, Afghani E, et al: Incidence, severity, and mortality of post-ERCP pancreatitis: a systematic review by using randomized, controlled trials. Gastrointest Endosc 81(1):143-149.e9, 2015. doi: 10.1016/j.gie.2014.06.045
Pathogenesis of Acute Pancreatitis
Regardless of the etiology, an early event in the pathogenesis of acute pancreatitis is intra-acinar activation of pancreatic enzymes (including trypsin, phospholipase A2, and elastase), leading to the autodigestive injury of the gland itself. The enzymes can damage tissue and activate the complement system and the inflammatory cascade, producing cytokines and causing inflammation and edema. This process causes necrosis in a few cases. Acute pancreatitis increases the risk of infection by compromising the gut barrier, leading to bacterial translocation from the gut lumen to the circulation.
Activated enzymes and cytokines that enter the peritoneal cavity cause a chemical burn and third spacing of fluid; those that enter the systemic circulation cause a systemic inflammatory response that can result in acute respiratory distress syndrome and acute kidney injury. The systemic effects are mainly the result of increased capillary permeability and decreased vascular tone, which result from the released cytokines and chemokines. Phospholipase A2 is thought to injure alveolar membranes of the lungs.
Classification of Acute Pancreatitis
The 2012 Revised Atlanta Classification (1) categorizes acute pancreatitis by type and severity.
Types of pancreatitis
Types of acute pancreatitis include
Interstitial edematous pancreatitis
Necrotizing pancreatitis
Interstitial edematous pancreatitis is defined by the presence of an enlarged pancreas on imaging. Peripancreatic stranding may be seen and is a sign of inflammation. Most patients develop this type of pancreatitis. The majority of cases are self-limited.
Necrotizing pancreatitis is defined by the presence of pancreatic and/or peripancreatic necrosis. It is best seen on contrast-enhanced cross-sectional imaging. Necrotizing pancreatitis occurs in about 5 to 10% of patients with acute pancreatitis and is associated with a prolonged and more severe disease course.
Severity of pancreatitis
Severity of acute pancreatitis can be classified as
Mild
Moderately severe
Severe
In mild acute pancreatitis, inflammation is confined to the pancreas and its close vicinity. Patients do not have organ failure or systemic or local complications. Mortality is rare.
In moderately severe acute pancreatitis, patients have local or systemic complications but no organ failure, or only transient organ failure (resolves within 48 hours).
In severe acute pancreatitis, there is persistent single or multiorgan failure (> 48 hours).
Classification reference
1. Banks PA, Bollen TL, Dervenis C, et al: Classification of acute pancreatitis 2012: Revision of the Atlanta classification and definitions by international consensus. Gut 62:102–111, 2013. doi: 10.1136/gutjnl-2012-302779
Complications of Acute Pancreatitis
Complications of acute pancreatitis can be categorized as (1)
Local: Pancreatic and peripancreatic fluid collections, splenic vein thrombosis, pseudoaneurysm formation, and gastric outlet dysfunction
Systemic: Shock, organ failure
Pancreatic and peripancreatic collections of enzyme-rich pancreatic fluid can occur early in the disease course. The collections contain only fluid or only fluid and necrotic material. Most of these collections resolve spontaneously, but if they do not resolve after about 4 weeks, they develop a fibrous capsule that can be seen on cross-sectional imaging. Such encapsulated collections are termed pancreatic pseudocysts or walled-off necrosis according to their contents; a pseudocyst contains only fluid, and walled-off necrosis contains both fluid and solid necrotic material. About one third of pseudocysts resolve spontaneously. In about one third of patients with pancreatic necrosis the fluid becomes infected by gut bacteria, which leads to very high morbidity and mortality.
Systemic complications include acute single or multiple organ failure (eg, cardiovascular and/or respiratory failure, acute kidney injury) and shock. Risk is increased in patients with underlying comorbidities and/or a persistent systemic inflammatory response syndrome (SIRS).
SIRS, in the appropriate clinical setting, is defined as the presence of two or more of the following (1):
Temperature > 38.3° C or < 36.0° C
Heart rate > 90/minute
Respiratory rate > 20/minute or PACO2 < 32 mmHg
White blood cell count > 12,000/mcL (12 × 109/L), < 4,000/mcL (4 × 109/L) or with > 10% bands
Organ failure is defined using the modified Marshall scoring system (see table Modified Marshall Organ Failure Score) (2), which is based on laboratory and vital sign indicators of respiratory, renal, and cardiovascular impairment.
Modified Marshall Organ Failure Score
Organ System | Score 0* | Score 1 | Score 2 | Score 3 | Score 4 |
Cardiovascular (systolic blood pressure)† | > 90 mm Hg | < 90 mm Hg (fluid responsive) | < 90 mm Hg (not fluid responsive) | < 90 mm Hg (pH < 7.3) | < 90 mm Hg (pH < 7.2) |
Renal (serum creatinine)‡ | < 1.4 mg/dL (≤ 134 micromol/L) | 1.4–1.8 mg/dL (134–169 micromol/L) | 1.9–3.6 mg/dL (170–310 micromol/L) | 3.6–4.9 mg/dL (311–439 micromol/L) | > 4.9 mg/dL (> 439 micromol/L) |
Respiratory (PaO2/FiO2)§ | > 400 mm Hg | 301–400 mm Hg | 201–300 mm Hg | 101–200 mm Hg | ≤ 101 mm Hg |
* A score of 2 or more in any organ system indicates organ failure. | |||||
† Off inotropic support. | |||||
‡ A score for patients with preexisting chronic kidney disease depends on the extent of further deterioration of baseline renal function. No formal correction exists for a baseline serum creatinine ≥ 1.5 mg/dL (≥ 134 micromol/L). | |||||
§ PaO2 in mm Hg; FiO2 is fractional inspired O2 in decimal fraction (eg, 0.5, rather than 50%). For nonventilated patients, the FiO2 can be estimated from the following: Supplemental oxygen: FiO2 (decimal fraction)
| |||||
Data from Banks PA, Bollen TL, Dervenis C, et al: Classification of acute pancreatitis 2012: Revision of the Atlanta classification and definitions by international consensus. Gut 62:102–111, 2013. doi: 10.1136/gutjnl-2012-302779 | |||||
Mortality in the early phase (within 1 week) of acute pancreatitis usually results from multiorgan failure, whereas mortality in the late phase (> 1 week) usually results from a combination of factors, including multiorgan failure, infection of pancreatic necrosis, and complications of surgical and endoscopic interventions.
Complications references
1. Bone RC, Balk RA, Cerra FB, et al: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101(6):1644-1655, 1992. doi: 10.1378/chest.101.6.1644
2. Banks PA, Bollen TL, Dervenis C, et al: Classification of acute pancreatitis 2012: Revision of the Atlanta classification and definitions by international consensus. Gut 62:102–111, 2013. doi: 10.1136/gutjnl-2012-302779
Symptoms and Signs of Acute Pancreatitis
An acute pancreatitis attack causes steady, boring upper abdominal pain, typically severe enough to require parenteral opioids. The pain radiates through to the back in about 50% of patients. Pain usually develops suddenly in gallstone pancreatitis; in alcoholic pancreatitis, pain develops over a few days. The pain usually persists for several days. Sitting up and leaning forward may reduce pain, but coughing, vigorous movement, and deep breathing may accentuate it. Nausea and vomiting are common.
The patient tends to appear acutely ill and sweaty. Pulse rate is usually elevated (eg, 100 to 140 beats/minute). Respiration is shallow and rapid. Blood pressure may be transiently high or low, with significant postural hypotension. Temperature may be normal or even subnormal at first but may increase to 37.7 to 38.3° C within a few hours. Sensorium may be blunted to the point of obtundation. Scleral icterus is occasionally present because of obstruction of the bile duct by a gallstone or inflammation and swelling of the pancreatic head. The lungs may have limited diaphragmatic excursion and evidence of atelectasis.
Patients may have an ileus, resulting in decreased bowel sounds and abdominal distention. Marked abdominal tenderness occurs, most often in the upper abdomen. Rarely, severe peritoneal irritation results in a rigid and boardlike abdomen. Pancreatic duct disruption may cause ascites (pancreatic ascites). The Grey Turner sign (ecchymoses of the flanks) and the Cullen sign (ecchymoses of the umbilical region) indicate extravasation of hemorrhagic exudate, occur in < 1% of cases, and portend a poor prognosis.
Infection in the pancreas or in an adjacent fluid collection should be suspected if the patient has a generally toxic appearance with fever and an elevated white blood cell count or if deterioration follows an initial period of stabilization. Patients with severe disease can develop multiorgan failure (cardiovascular, renal, and respiratory).
Diagnosis of Acute Pancreatitis
Serum markers (amylase, lipase)
Imaging studies
Pancreatitis is suspected whenever severe unexplained abdominal pain occurs, especially in a patient with significant alcohol consumption or known gallstones.
The diagnosis of acute pancreatitis is established by the presence of at least 2 of the following:
Abdominal pain consistent with the disease
Serum amylase and/or lipase > 3 times the upper limit of normal (normal range of amylase and lipase levels can differ depending on the assay used)
Characteristic findings on contrast-enhanced cross-sectional imaging studies
The differential diagnosis of the symptoms of acute pancreatitis includes
Perforated gastric or duodenal ulcer
Mesenteric infarction
Biliary colic
Inferior wall myocardial infarction
Hematoma of the abdominal muscles or spleen
To exclude other causes of abdominal pain and to diagnose metabolic complications of acute pancreatitis, a broad range of tests is usually done at initial evaluation. These include laboratory and imaging tests.
Laboratory tests
Serum amylase and lipase concentrations increase on the first day of acute pancreatitis and typically return to normal in 3 to 7 days. Lipase is more specific for pancreatitis, but both enzymes may be increased in renal failure and various abdominal conditions (eg, perforated ulcer, mesenteric vascular occlusion, intestinal obstruction). Other causes of increased serum amylase include salivary gland dysfunction, macroamylasemia, and tumors that secrete amylase. Fractionation of total serum amylase into pancreatic type (p-type) isoamylase and salivary-type (s-type) isoamylase increases the accuracy of serum amylase.
Both amylase and lipase levels may remain normal if destruction of acinar tissue during previous episodes precludes release of sufficient amounts of enzymes. The normal range of amylase and lipase levels can differ depending on the assay used. The serum of patients with hypertriglyceridemia may contain a circulating inhibitor that must be diluted before an elevation in serum amylase can be detected.
Serum amylase levels may be chronically elevated in macroamylasemia where amylase is bound to a serum immunoglobulin to form a complex that is filtered slowly from the blood by the kidneys. Amylase:creatinine clearance ratio does not have sufficient sensitivity or specificity to diagnose pancreatitis. It is generally used to diagnose macroamylasemia when no pancreatitis exists.
A urine dipstick test for trypsinogen-2 has sensitivity and specificity of > 90% for acute pancreatitis.

The white blood cell count usually increases to 12,000 to 20,000/mcL (12 to 20 × 109/L). Third-space fluid losses may increase the hematocrit to as high as 50 to 55% and elevate the blood urea nitrogen (BUN), indicating severe inflammation. Persistent elevation in BUN despite resuscitation is an indicator of increased morbidity and mortality.
Hyperglycemia and hypocalcemia may occur. Patients may have abnormal liver function test results, including elevated serum bilirubin, due to a retained stone in the bile duct or to compression of the bile duct by pancreatic edema. Patients with shock may have an elevated anion gap metabolic acidosis or other electrolyte abnormalities. Hypomagnesemia needs to be excluded in patients with hypocalcemia.
Imaging studies
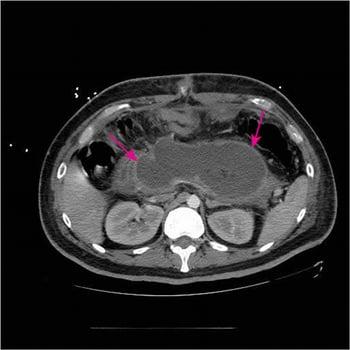
CT with IV contrast is the imaging study of choice to establish the diagnosis of acute pancreatitis and to assess for local complications. It is done early in the disease course if the diagnosis of acute pancreatitis is uncertain or to exclude other causes for the patient's symptoms. Also, once pancreatitis has been diagnosed, CT is done later in the disease course to identify the complications of acute pancreatitis such as necrosis, fluid collection, or pseudocysts, particularly if abdominal symptoms persist. Necrotic pancreatic tissue does not enhance after IV contrast is given. Generally, MRI outperforms CT for detecting choledocholithiasis and pancreatic necrosis and should be done in patients in whom other tests for choledocholithiasis were indeterminate and in patients who are considered likely to need a pancreatic drainage procedure.

Abdominal ultrasonography should be done if gallstone pancreatitis is suspected (and another cause is not obvious) to detect gallstones or dilation of the common bile duct, which indicates biliary tract obstruction. Edema of the pancreas may be visible, but overlying gas frequently obscures the pancreas.
If done, plain x-rays of the abdomen may disclose calcifications within pancreatic ducts (evidence of prior inflammation and hence chronic pancreatitis), calcified gallstones, localized ileus of a segment of small intestine in the left upper quadrant or the center of the abdomen (a “sentinel loop”), or the colon cutoff sign (absence of air in left colonic flexure or descending colon) in more severe disease. However, the value of routine abdominal x-rays is controversial.
Chest x-ray should be done and may reveal atelectasis or a pleural effusion (usually left-sided or bilateral but rarely confined to the right pleural space), which are signs of severe disease.
The role of endoscopic ultrasonography is limited in acute pancreatitis. Endoscopic ultrasonography has a comparable sensitivity to magnetic resonance cholangiopancreatography (MRCP) for detecting common bile duct stones, but MRCP has the advantage of being noninvasive. MRCP is done if liver tests, particularly direct bilirubin and alanine aminotransferase (ALT), are elevated from their baseline and abdominal ultrasonography does not exclude gallstones in the common bile duct as the etiology for gallstone acute pancreatitis.
Endoscopic retrograde cholangiopancreatography (ERCP) to relieve bile duct obstruction should be done expeditiously in patients with gallstone pancreatitis who have increasing serum bilirubin and signs of cholangitis.
Treatment of Acute Pancreatitis
Supportive measures
For severe acute pancreatitis and complications, antibiotics and therapeutic interventions as needed
Treatment of acute pancreatitis is typically supportive. Patients who develop complications may require specific additional treatment. (See also the American College of Gastroenterology's [ACG] 2013 guidelines for the management of acute pancreatitis.)
The basic treatment of acute pancreatitis includes
Early goal-directed fluid resuscitation
Analgesia
Nutritional support
The ACG's 2013 guidelines recommend that early, aggressive fluid resuscitation, defined as 250 to 500 mL/hour of isotonic crystalloid solution (ideally lactated Ringer's solution), be provided to all patients during the first 12 to 24 hours unless contraindicated by cardiovascular, renal, or other related comorbid factors. Adequacy of fluid replacement can be assessed by reduction in hematocrit and blood urea nitrogen levels over the first 24 hours, particularly if they were high at the onset. Other parameters include improvement in vital signs and maintenance of adequate urine output. The ACG guidelines also recommend that fluid requirements be reassessed at frequent intervals in the first 6 hours of admission and for the next 24 to 48 hours. Patients undergoing volume resuscitation should have pulse oximetry monitored continuously, receive supplemental oxygen as needed, and have their fluid intake and output strictly monitored. However, these recommendations are likely to change because overaggressive fluid resuscitation has been shown to increase adverse outcomes. A trial suggests moderate fluid resuscitation as the preferred resuscitation protocol (1.5 mL/kg/hour of lactated Ringer’s solution and, for patients with hypovolemia, 10 mL/kg boluses) (1).
Pain relief requires use of parenteral opioids such as hydromorphone or fentanyl, which should be given in adequate doses. Because morphine can theoretically increase pressure in the sphincter of Oddi, hydromorphone is usually preferred to morphine. Antiemetic drugs should be given to relieve nausea and vomiting.
Early enteral nutrition is recommended because it is associated with lower morbidity compared to delayed or no nutrition. Patients with mild pancreatitis can begin an oral low-residue, low-fat, soft diet as soon as it can be tolerated. If oral nutrition cannot be initiated early in the disease course, enteral feeding is preferred over total parenteral nutrition because parenteral nutrition is associated with increased risk of infectious complications and organ failure.
Severe acute pancreatitis and complications
Treatment of severe acute pancreatitis and complications includes
Intensive care unit (ICU) care
Enteral nutrition preferred over parenteral nutrition
Antibiotics for extrapancreatic infections and infected necrosis
Necrosectomy (removal of necrotic tissue) for infected necrosis
Endoscopic retrograde cholangiopancreatography (ERCP) for acute pancreatitis and concurrent acute cholangitis
Drainage of pseudocysts
The management of patients with severe acute pancreatitis and its complications should be individualized using a multidisciplinary approach including therapeutic endoscopists, interventional radiologists, and a surgeon. Patients with severe acute pancreatitis should be monitored closely in the first 24 to 48 hours in an ICU. Patients with worsening condition or widespread local complications requiring intervention should be transferred to centers of excellence focusing on pancreatic disease (if available).
Patients with severe acute pancreatitis may need artificial nutritional support, although the optimal starting time and duration of nutritional support are still unclear. The ACG's 2013 guidelines recommend using enteral nutrition and giving parenteral nutrition only if the enteral route is not available, not tolerated, or not meeting caloric requirements. The enteral route is preferred because it
Helps maintain the intestinal mucosal barrier
Prevents the intestinal atrophy that can occur with prolonged bowel rest (and helps prevent translocation of bacteria that can seed pancreatic necrosis)
Avoids the risk of infection of a central IV catheter
Is less expensive
A nasojejunal feeding tube placed beyond the ligament of Treitz may help avoid stimulating the gastric phase of the digestive process; placement requires radiologic or endoscopic guidance. If a nasojejunal feeding tube cannot be placed, nasogastric feeding should be initiated. In both cases, patients should be placed in the upright position to decrease risk of aspiration. The ACG guidelines note that nasogastric and nasojejunal feeding appear comparable in their efficacy and safety.
According to the ACG's 2013 guidelines and the American Gastroenterological Association's 2018 guideline on initial management of acute pancreatitis, prophylactic antibiotics are not recommended in patients with acute pancreatitis, regardless of the type or disease severity. However, antibiotics should be started if patients develop an extrapancreatic infection (eg, cholangitis, pneumonia, bloodstream infection, urinary tract infection) or infected pancreatic necrosis.
Infection (pancreatic or extrapancreatic) should be suspected in patients who have signs of deterioration (eg, fever, hypotension, tachycardia, altered mental status, increasing white blood cell count) or who fail to improve after 7 to 10 days of hospitalization. Most infections in pancreatic necrosis are caused by single bacterial species from the gut. The most common organisms are gram-negative bacteria; gram-positive bacteria and fungi are rare. In patients with infected necrosis, antibiotics known to penetrate pancreatic necrosis, such as carbapenems, fluoroquinolones, and metronidazole, are recommended.
For necrosectomy (removal of infected tissue), a minimally invasive approach is preferred over an open surgical approach and should be attempted initially. The ACG's 2013 guidelines recommend that drainage of infected necrosis (radiologic, endoscopic, or surgical approach) should be delayed, preferably for > 4 weeks in patients who are stable, to allow liquefication of the contents and the development of a fibrous capsule around the necrosis (walled-off necrosis).
More than 80% of patients with gallstone pancreatitis pass the stone spontaneously and do not require endoscopic retrograde cholangiopancreatography (ERCP). Patients with acute pancreatitis and concurrent acute cholangitis should undergo early ERCP. Patients with mild gallstone pancreatitis who spontaneously improve should undergo cholecystectomy before discharge to prevent recurrent attacks.
A pseudocyst that is expanding rapidly, infected, bleeding, or likely to rupture requires drainage. Whether drainage is percutaneous, surgical, or endoscopic ultrasound–guided cystogastrostomy depends on location of the pseudocyst and institutional expertise.
Treatment reference
1. de-Madaria E, Buxbaum JL, Maisonneuve P, et al: Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis. N Engl J Med 387(11):989-1000, 2022. doi: 10.1056/NEJMoa2202884
Prognosis for Acute Pancreatitis
The severity of acute pancreatitis is determined by the presence of organ failure, local and systemic complications, or a combination. Using patient-related risk factors to assess severity early in the course of disease can help identify patients at increased risk of developing organ dysfunction and other complications. These patients can then be given maximal supportive therapy at presentation to improve outcomes and decrease morbidity and mortality.
For initial risk assessment, patient-related risk factors that predict a severe course include the following:
Age ≥ 60 years
Comorbid health problems
Obesity with body mass index > 30
Long-term, heavy alcohol consumption
Presence of systemic inflammatory response syndrome (SIRS)
Laboratory markers of hypovolemia (eg, elevated BUN, elevated hematocrit)
Presence of pleural effusions and/or infiltrates on admission chest x-ray
Altered mental status
Severity scoring systems require multiple measurements and may delay appropriate management. Some of these can be done at admission to assist in triage of patients, whereas others are not accurate until 48 to 72 hours after presentation.
Ranson criteria (1): This scoring system is cumbersome and requires data from a 48-hour period to compute but has good negative predictive value.
The APACHE II score: This system is complex and cumbersome to use but has good negative predictive value.
Systemic inflammatory response syndrome score: This is inexpensive, readily available, and can be applied at the bedside.
Bedside index of severity in acute pancreatitis (BISAP) score: This score is simple and calculated during the first 24 hours.
Harmless acute pancreatitis score: This simple score is calculated within 30 minutes of admission.
Organ failure–based scores: These scores do not directly measure the severity of acute pancreatitis.
CT severity index (Balthazar score): This score is based on the degree of necrosis, inflammation, and the presence of fluid collections on CT.
The long-term risks after acute pancreatitis include the risks of recurrent attacks and development of chronic pancreatitis. Risk factors include the severity and amount of pancreatic necrosis in the initial episode of acute pancreatitis as well as the etiology; long-term, heavy alcohol consumption and cigarette smoking increase the risk of developing chronic pancreatitis.
Prognosis reference
1. Ranson JH, Rifkind KM, Roses DF, et al: Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet 139(1):69-81, 1974. PMID: 4834279
Key Points
There are many causes of acute pancreatitis, but the most common are gallstones and alcohol intake.
Inflammation is confined to the pancreas in mild cases, but, with increasing severity, a severe systemic inflammatory response may develop, resulting in shock and/or organ failure.
Once pancreatitis is diagnosed, assess risk using clinical criteria and scoring systems to triage appropriate patients to more intensive care and aggressive therapy and to help estimate prognosis.
Treatment includes IV fluid resuscitation, pain control, and nutritional support.
Complications, including pseudocyst and infected pancreatic necrosis, need to be identified and treated appropriately (eg, drainage of pseudocyst, necrosectomy).
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American College of Gastroenterology: Guidelines for the management of acute pancreatitis (2013)
American Gastroenterological Association: Guidelines on the initial management of acute pancreatitis (2018)







