


Taenia solium infection (taeniasis) is an intestinal infection with adult tapeworms that follows ingestion of contaminated pork. Adult worms may cause mild gastrointestinal symptoms or passage of a motile segment in the stool. Cysticercosis is infection with larvae of T. solium, which develops after ingestion of ova excreted in human feces. Cysticercosis is usually asymptomatic unless larvae invade the central nervous system, resulting in neurocysticercosis, which can cause seizures and various other neurologic signs. Neurocysticercosis may be recognized on brain imaging studies. Fewer than half of patients with neurocysticercosis have adult T. solium
Presentation, diagnosis, and management of intestinal infection with the adult T. solium tapeworm are similar to those of T. saginata (beef tapeworm) infection.
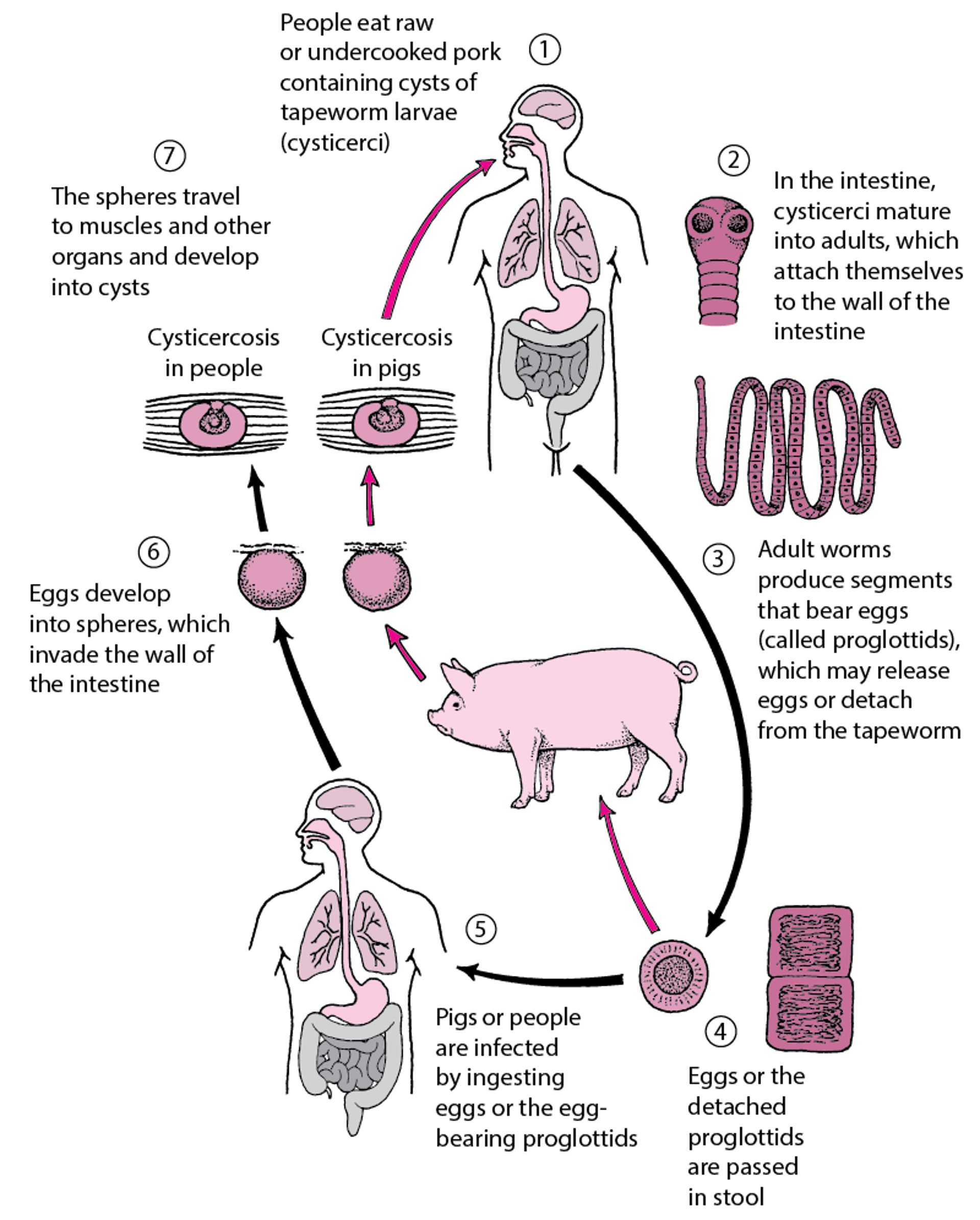
However, humans may also act as intermediate hosts for T. solium larvae if they ingest T. solium eggs from human excreta (see figure Taenia solium Life Cycle). Some experts postulate that if an adult tapeworm is present in the intestine, gravid proglottids (tapeworm segments) may be passed retrograde from the intestine to the stomach, where oncospheres (immature form of the parasite enclosed in an embryonic envelope) may hatch and migrate to subcutaneous tissue, muscle, viscera, and the central nervous system.
Adult tapeworms may reside in the small bowel for years. They reach 2 to 8 m in length and produce up to 1000 proglottids; each contains approximately 50,000 eggs.
Taenia solium Life Cycle
Humans may develop intestinal infection with adult worms after ingestion of contaminated pork or may develop cysticercosis after ingestion of eggs (making humans intermediate hosts).
|

Taeniasis and cysticercosis occur worldwide. Cysticercosis is prevalent, and neurocysticercosis is a major cause of seizure disorders in Latin America. Cysticercosis is rare in countries with low pork consumption. Infection in the United States or Canada is rare in those who have not traveled abroad, but infection may occur by ingesting ova from people who visited endemic countries and are harboring adult T. solium.
Rarely, Taenia species other than T. solium cause neurocysticercosis.
Symptoms and Signs
Intestinal infection
Humans infected with adult T. solium worms are asymptomatic or have mild gastrointestinal complaints. They may see proglottids in their stool.
Cysticercosis
Viable cysticerci (larval form) in most organs cause minimal or no tissue reaction, but dying cysts in the central nervous system, eye, or spinal cord can release antigens that elicit an intense tissue response. Thus, symptoms often do not appear for years after infection.
Infection in the brain (neurocysticercosis) may result in severe symptoms due to mass effect and inflammation induced by degeneration of cysticerci and release of antigens.
Depending on the location and number of cysticerci, patients with neurocysticercosis may present with seizures, signs of increased intracranial pressure, hydrocephalus, focal neurologic signs, altered mental status, or aseptic meningitis.
Cysticerci may also infect the spinal cord, muscles, subcutaneous tissues, and eyes.
Substantial secondary immunity develops after larval infection.
Diagnosis
Microscopic examination of stool for ova and proglottids
CT and/or MRI and serologic testing for patients with central nervous system symptoms
Intestinal infection with adult T. solium worms can usually be diagnosed by microscopic examination of stool samples and identification of ova and/or proglottids. However, the ova are indistinguishable from those of T. saginata and T. asiatica. T. solium eggs are present in ≤ 50% of stool samples from patients with cysticercosis.
Neurocysticercosis is usually diagnosed when CT or MRI is done to evaluate neurologic symptoms. Scans may show solid nodules, cysticerci, calcified cysts, ring-enhancing lesions, or hydrocephalus. The Centers' for Disease Control and Prevention immunoblot assay (using a serum or cerebrospinal fluid specimen) is highly specific and more sensitive than other enzyme immunoassays (particularly when > 2 central nervous system lesions are present; sensitivity is lower when only a single cyst is present). Note that antibody-based assays such as immunoblot do not distinguish between active and inactive infections.
Monoclonal antibody-based antigen detection assays are commercially available in Europe. Antigen detection assays appear to have higher sensitivity for subarachnoid and ventricular neurocysticercosis over parenchymal disease. The sensitivity of antigen detection is improved when cerebrospinal fluid rather than serum is used; however, false-negative results may be common with parenchymal disease (1).
Pearls & Pitfalls
|
Diagnosis reference
1. Pineda-Reyes R, White AC Jr.: Neurocysticercosis: an update on diagnosis, treatment, and prevention. Curr Opin Infect Dis 35(3):246-254, 2022. doi:10.1097/QCO.0000000000000831
Treatment
Treatment of intestinal infection
A stool sample should be repeated three months after therapy is completed to verify cure.
Antiparasitic drugs should be used with caution in patients who also have signs of neurocysticercosis (including previously asymptomatic or unrecognized disease) because killing of cysts in the brain may trigger an inflammatory response associated with seizures or other symptoms.
Treatment of neurocysticercosis
Treatment of neurocysticercosis is complicated. Detailed clinical practice guidelines on the Diagnosis and Treatment of Neurocysticercosis were issued by the Infectious Diseases Society of America and the American Society of Tropical Medicine and Hygiene in 2017.
The initial treatment goals for symptomatic neurocysticercosis are
To reduce inflammation associated with degenerating cysticerci documented by MRI
To prevent seizures if present or if risk is high
To relieve increased intracranial pressure if present
Conventional antiseizure drugs are given to patients who have seizures. These drugs can be used prophylactically in patients at high risk of seizures, particularly those who have multiple degenerating lesions with associated inflammation.
Neurosurgical intervention may be necessary for patients with increased intracranial pressure or intraventricular cysticerci.
Anthelmintic treatment of neurocysticercosis is complicated, and consultation with an expert is recommended. Initiation of antihelminthic therapy is not urgent, and it is critical that antihelminthic therapy be done after inflammation is controlled by corticosteroids. Choice of treatment depends on the location, number, viability, and size of cysticerci; stage of the disease; and clinical manifestations. Prior to anthelmintic treatment, an ophthalmologic examination should be done to exclude the presence of ocular cysticerci. Antihelminthic drugs should never be administered to patients with uncontrolled increased intracranial pressure.
Not all patients respond to treatment, and not all patients must be treated (cysts may already be dead and calcified, or the potential inflammatory response to treatment may be worse than the disease, as in cysticercal encephalitis when patients have a large number of cysts and widespread brain inflammation).
Either or
The presence of intraventricular cysticerci is also a relative contraindication for anthelminthic drugs because the resulting inflammatory response elicited by the dying cysts can cause obstructive hydrocephalus.
Surgery may be necessary for obstructive hydrocephalus (due to intraventricular cysticerci including those in the 4th ventricle) or spinal or ocular cysticercosis. Intraventricular cysticerci are removed endoscopically when possible. Ventricular shunts may be needed to reduce increased intracranial pressure.
Treatment references
1. Winthrop KL, Baddley JW: Pneumocystis and glucocorticoid use: to prophylax or not to prophylax (and when?); that is the question. Ann Rheum Dis 77(5):631-633, 2018. doi:10.1136/annrheumdis-2017-212588
2. Park JW, Curtis JR, Moon J, Song YW, Kim S, Lee EB: Prophylactic effect of trimethoprim-sulfamethoxazole for pneumocystis pneumonia in patients with rheumatic diseases exposed to prolonged high-dose glucocorticoids. Ann Rheum Dis 77(5):644-649, 2018. doi:10.1136/annrheumdis-2017-211796
Prevention
Intestinal T. solium infection can be prevented by cooking whole cuts of pork to ≥ 63° C (≥ 145° F) as measured with a food thermometer placed in the thickest part of the meat, then allowing the meat to rest for 3 minutes before carving or consuming. Ground pork should be cooked to ≥ 71° C (≥ 160° F). Ground pork does not require a rest period.
Identifying and treating carriers of adult T. solium is an important public health measure in preventing cysticercosis. In the United States, transmission has occurred when people who were infected in endemic areas had adult T. solium in their intestines, then contaminated food with their stool. It is very important that food handlers from endemic areas be taught and adhere to good handwashing practices.
When traveling to endemic areas with poor sanitation, people should be careful to avoid foods that might be contaminated by human feces and avoid raw and inadequately cooked pork.
Key Points
Ingestion of T. solium cysts may cause intestinal infection; ingestion of eggs may result in tissue cysts (cysticercosis), which are particularly problematic when in the brain.
Patients with neurocysticercosis may have seizures, signs of increased intracranial pressure, altered mental status, focal neurologic signs, or aseptic meningitis.
Diagnose intestinal infection with adult worms by identifying proglottids in stool and microscopic examination of stool samples for ova.
Diagnose neurocysticercosis by neuroimaging and serologic testing.
Consult an expert for neurocysticercosis; typically corticosteroids are given with antiseizure drugs to patients who have associated seizures or are thought to be at high risk of seizures.
Use of anthelmintics and/or surgery for neurocysticercosis depends on the location, number, and size of cysticerci; stage of the disease; and clinical manifestations.







