


Rocky Mountain spotted fever (RMSF) is caused by Rickettsia rickettsii and transmitted by ixodid ticks. Symptoms are high fever, severe headache, and rash.
(See also Overview of Rickettsial and Related Infections.)
Rocky Mountain spotted fever is a rickettsial disease.
Epidemiology of RMSF
RMSF is limited to the Western Hemisphere. Initially recognized in the Rocky Mountain states, it occurs in practically all of the United States and throughout Central and South America. In humans, infection occurs mainly from March to September, when adult ticks are active and people are most likely to be in tick-infested areas. In southern states, sporadic cases occur throughout the year. The incidence is highest in children < 15 years and in people who frequent tick-infested areas for work or recreation. (See also Centers for Disease Control and Prevention: RMSF–epidemiology and statistics.)
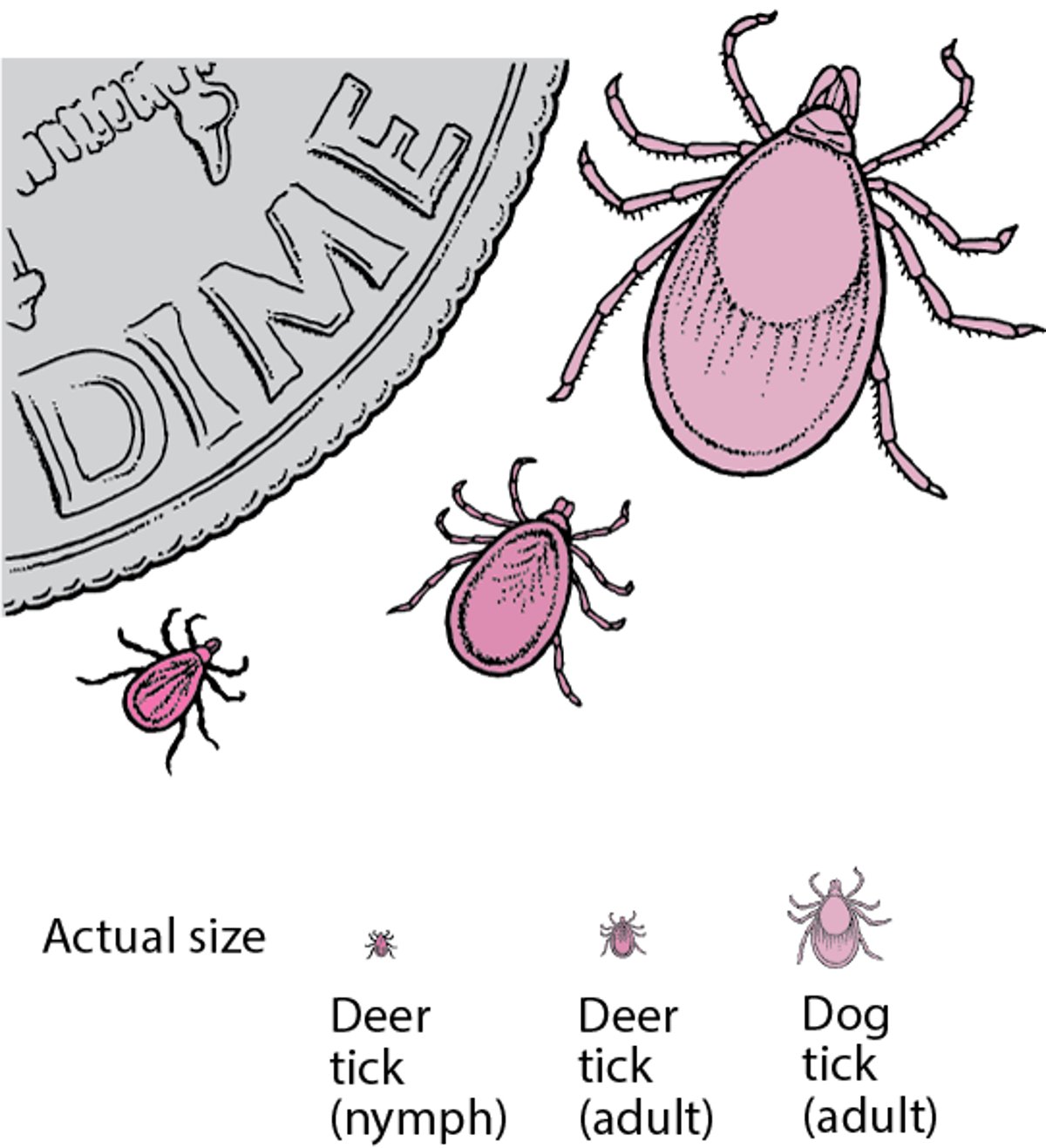
Hard-shelled ticks (family Ixodidae) harbor R. rickettsii, and infected females transmit the agent to their progeny. These ticks are the natural reservoirs. Dermacentor andersoni (wood tick) is the principal vector in the western United States. D. variabilis (dog tick) is the vector in the eastern and southern United States.


Image courtesy of Dr. Christopher Paddock via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Dr. Christopher Paddock via the Public Health Image Library of the Centers for Disease Control and Prevention.
RMSF is probably not transmitted directly from person to person.
Pathophysiology of RMSF
Small blood vessels are the sites of the characteristic pathologic lesions of Rocky Mountain spotted fever. Rickettsiae propagate within damaged endothelial cells, and vessels may become blocked by thrombi, producing vasculitis in the skin, subcutaneous tissues, central nervous system, lungs, heart, kidneys, liver, and spleen. Disseminated intravascular coagulation rarely occurs (1).
Pathophysiology reference
1. Walker DH: Rickettsiae and rickettsial infections: the current state of knowledge. Clin Infect Dis 15;45 Suppl 1:S39-44, 2007. doi: 10.1086/518145
Symptoms and Signs of RMSF
The incubation period for Rocky Mountain spotted fever averages 7 days but varies from 3 to 12 days; the shorter the incubation period, the more severe the infection.
Onset is abrupt, with severe headache, chills, prostration, and muscular pains. Fever reaches 39.5 to 40° C within several days and remains high (for 15 to 20 days in severe cases), although morning remissions may occur.
Between the first and sixth day of fever, most patients with RMSF develop a rash on the wrists, ankles, palms, soles, and forearms that rapidly extends to the neck, face, axillae, buttocks, and trunk. Initially macular and pink, it becomes maculopapular and darker. In about 4 days, the lesions become petechial and may coalesce to form large hemorrhagic areas that later ulcerate.

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Neurologic symptoms include headache, restlessness, insomnia, delirium, and coma, all indicative of encephalitis.
Hypotension develops in severe cases. Hepatomegaly may be present, but jaundice is infrequent. Nausea and vomiting are common. Localized pneumonitis may occur. Untreated patients may develop pneumonia, tissue necrosis, and circulatory failure, sometimes with brain and heart damage. Cardiac arrest with sudden death occasionally occurs in fulminant cases.
Diagnosis of RMSF
History and physical examination
Biopsy of rash with fluorescent antibody staining to detect organisms
Acute and convalescent serologic testing (serologic testing not useful acutely)
Polymerase chain reaction (PCR)
Clinicians should suspect Rocky Mountain spotted fever in any seriously ill patient who lives in or near a wooded area anywhere in the Western Hemisphere and has unexplained fever, headache, and prostration, with or without a history of tick contact. A history of tick bite is elicited in about 60% of patients (see CDC: RMSF).
Testing is usually required to confirm RMSF but because of the limitations of currently available tests, clinicians typically must make treatment decisions before receiving results of confirmatory testing.
If patients have a rash, a skin biopsy should be taken from the rash site. PCR or immunohistochemical staining, which can provide fairly rapid results, is used. However, a negative test result does not justify withholding treatment when clinical manifestations suggest RMSF.
Culture of R. rickettsii is available only at specialized laboratories.
Pearls & Pitfalls
|
Serologic tests are not useful for acute diagnosis because they usually become positive only during convalescence. Indirect immunofluorescence assay using 2 paired samples is usually done.
For details, see Diagnosis of Rickettsial and Related Infections.
Treatment of RMSF
Starting antibiotics early significantly reduces mortality and prevents most complications of Rocky Mountain spotted fever . If patients who have been in an endemic area have a tick bite but no clinical symptoms or signs, antibiotics should not be given immediately.
If fever, headache, and malaise occur with or without a rash, antibiotics should be started promptly.
Centers for Disease Control and Prevention (CDC) has found that short courses of doxycycline (5 to 10 days) can be used in children without causing tooth staining or weakening of tooth enamel. Use of antibiotics other than doxycycline
chloramphenicol is not available in the United States, and its use can cause grey baby syndrome and adverse hematologic effects, which requires monitoring of blood indices.
Regarding pregnant patients, the CDC advises1). Thus, pregnant women should be counseled on the potential risks versus benefits when making a decision about antibiotic treatment of RMSF.
Severely ill patients with RMSF may have a marked increase in capillary permeability in later stages; thus, IV fluids should be given cautiously to maintain blood pressure while avoiding worsening pulmonary and cerebral edema.
Treatment reference
1. Todd SR, Dahlgren FS, Traeger MS, et alJ Pediatr 166(5):1246-51, 2015. doi: 10.1016/j.jpeds.2015.02.015
Prevention of RMSF
No effective vaccine is available to prevent Rocky Mountain spotted fever. Measures can be taken to prevent tick bites. (See also Centers for Disease Control and Prevention: Preventing tick bites.)
Deer ticks

Preventing tick access to skin includes
Staying on paths and trails
Tucking trousers into boots or socks
Wearing long-sleeved shirts
Engorged ticks should be removed with care and not crushed between the fingers because crushing the tick may result in disease transmission. The tick’s body should not be grasped or squeezed. Gradual traction on the head with a small forceps dislodges the tick. The point of attachment should be swabbed with alcohol. Petroleum jelly, lit matches, and other irritants are not effective ways to remove ticks and should not be used.
No practical means are available to rid entire areas of ticks, but tick populations may be reduced in endemic areas by controlling small-animal populations.
Key Points
Despite its name, Rocky Mountain spotted fever (RMSF) occurs in practically all of the United States and throughout Central and South America.
Small-vessel vasculitis can cause serious illness affecting the central nervous system, lungs, heart, kidneys, liver, and spleen; untreated mortality is about 20%.
Symptoms (severe headache, chills, prostration, muscle pain) begin abruptly, followed by fever and usually a rash.
Neurologic symptoms (headache, restlessness, insomnia, delirium, coma) may develop, indicating encephalitis.
Suspect RMSF in any seriously ill patient who lives in or near a wooded area anywhere in the Western Hemisphere and has unexplained fever, headache, and prostration, with or without a history of tick contact.
Test during acute illness with PCR or immunohistology of a skin biopsy specimen, but because sensitivity is only about 70%, a negative result should not affect the decision to begin antibiotics.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Centers for Disease Control and Prevention: Information about preventing tick bites
Centers for Disease Control and Prevention: Information regarding the transmission, symptoms, diagnosis, and treatment of RMSF for healthcare providers
Centers for Disease Control and Prevention:Information and statistics about the epidemiology of RMSF







