






Aging, estrogen deficiency, low vitamin D or calcium intake, and certain disorders can decrease the amounts of the components that maintain bone density and strength.
Osteoporosis may not cause symptoms until a bone fracture occurs.
Fractures can occur with little or no force and may occur after a minor fall.
Although fractures are often painful, some fractures of the spine do not cause pain but can cause deformities.
Doctors diagnose people at risk by testing their bone density.
Osteoporosis can usually be prevented and treated by managing risk factors, ensuring adequate calcium and vitamin D intake, engaging in weight-bearing exercise, and taking bisphosphonates or other medications.
Bones contain minerals, including calcium and phosphorus, which make them hard and dense. To maintain bone density (or bone mass), the body requires an adequate supply of calcium and other minerals and must produce the proper amounts of several hormones, such as parathyroid hormone, growth hormone, calcitonin, estrogen, and testosterone. An adequate supply of vitamin D is needed to absorb calcium from food and incorporate it into bones. Vitamin D is absorbed from the diet and also manufactured in the skin using sunlight.
So that bones can adjust to the changing demands placed on them, they are continuously broken down and reformed. This process is known as remodeling. In this process, small areas of bone tissue are continuously removed and new bone tissue is deposited. Remodeling affects the shape and density of the bones.
Loss of Bone Density in Women
In women, bone density (or mass) progressively increases until about age 30, at which time bones are at their strongest. After that, bone density gradually decreases. The decrease in bone density accelerates after menopause, which occurs on average around age 51. |

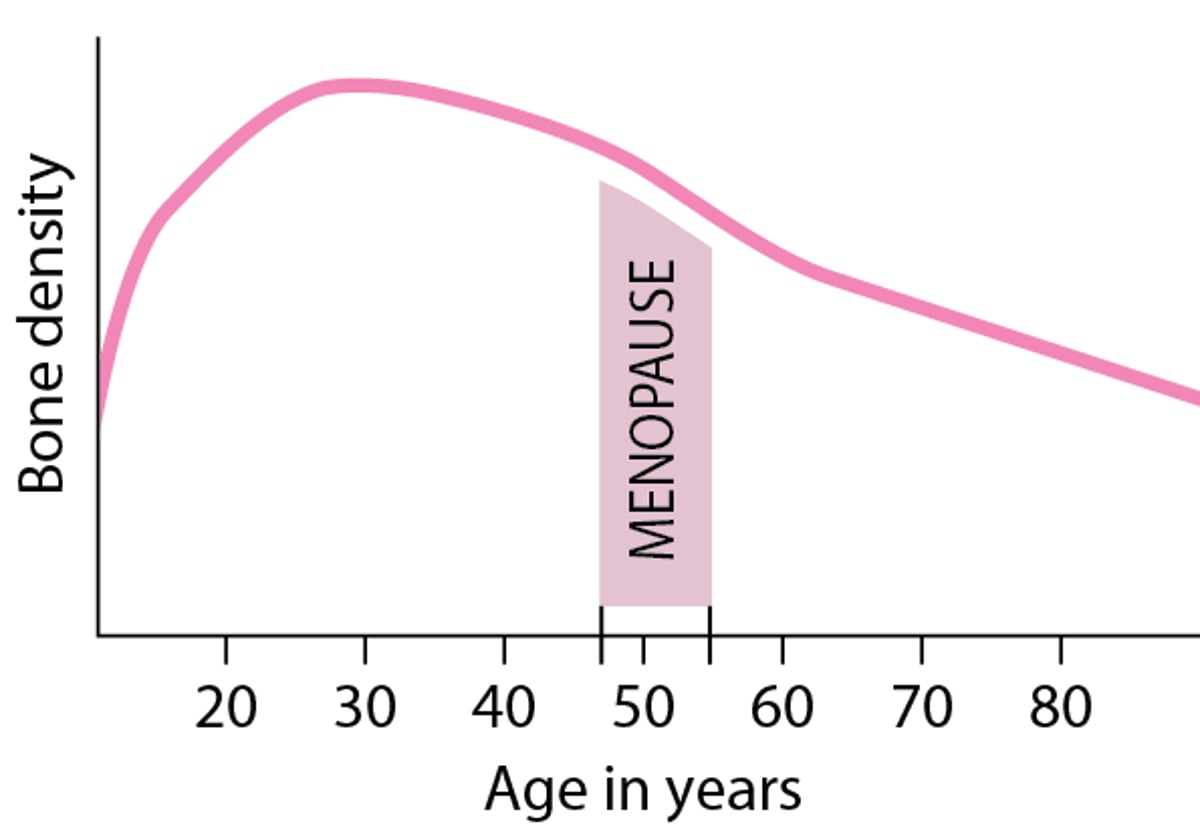
Because more bone is formed than is broken down in the young adult years, bones progressively increase in density until about age 30, when they are at their strongest. After that, as breakdown exceeds formation, bones slowly decrease in density. If the body is unable to maintain an adequate amount of bone formation, bones continue to lose density and may become increasingly fragile, eventually resulting in osteoporosis.
Types of Osteoporosis

Osteoporosis is more common in women. It affects almost 20% (1 in 5) of women aged 50 and over and almost 5% (1 in 20) of men aged 50 and over. Approximately 50% of postmenopausal women and 20% of men over age 50 years will sustain an osteoporosis-related fracture in their lifetimes. There are two main types of osteoporosis:
Primary osteoporosis: Occurs spontaneously
Secondary osteoporosis: Is caused by another disorder or by a medication
Primary osteoporosis
Nearly all occurrences of osteoporosis in both men and women are primary. Most cases occur in postmenopausal women and in older men.
A major cause of osteoporosis is a lack of estrogen, particularly the rapid decrease that occurs at menopause. Most men over 50 have higher estrogen levels than postmenopausal women, but these levels also decline with aging, and low estrogen levels are associated with osteoporosis in both men and women. Estrogen deficiency increases bone breakdown and results in rapid bone loss. In men, low levels of male sex hormones also contribute to osteoporosis. Bone loss is even greater if calcium intake or vitamin D levels are low. Low vitamin D levels result in calcium deficiency, and increased activity of the parathyroid glands causes the glands to release too much parathyroid hormone (see hyperparathyroidism), which can also stimulate bone breakdown. Bone production also decreases.
A number of other factors, such as certain medications, tobacco use, heavy alcohol use, a family history of osteoporosis (for example, if a person's mother or father has had a hip fracture), and small body stature, increase the risk of bone loss and the development of osteoporosis in women. These risk factors are also important in men.
Secondary osteoporosis
Examples of disorders that may cause secondary osteoporosis are chronic kidney disease, and hormonal disorders (especially Cushing disease, hyperparathyroidism, hyperthyroidism, hypogonadism, high levels of prolactin, and diabetes mellitus). Certain types of cancer, such as multiple myeloma, can cause secondary osteoporosis, as can other diseases such as celiac disease and rheumatoid arthritis. Examples of medications that, if used for a long time, may cause secondary osteoporosis are progesterone, steroids (also sometimes referred to as glucocorticoids or corticosteroids), thyroid hormones, aromatase inhibitors (for breast cancer), and antiseizure medications. Excessive alcohol and cigarette smoking may contribute to osteoporosis.
Idiopathic osteoporosis
Idiopathic osteoporosis is a rare type of osteoporosis. The word idiopathic simply means that the cause is unknown. This type of osteoporosis occurs in premenopausal women, in men under age 50, and in children and adolescents who have normal hormone levels, normal vitamin D levels, and no obvious reason to have weak bones.
Symptoms of Osteoporosis
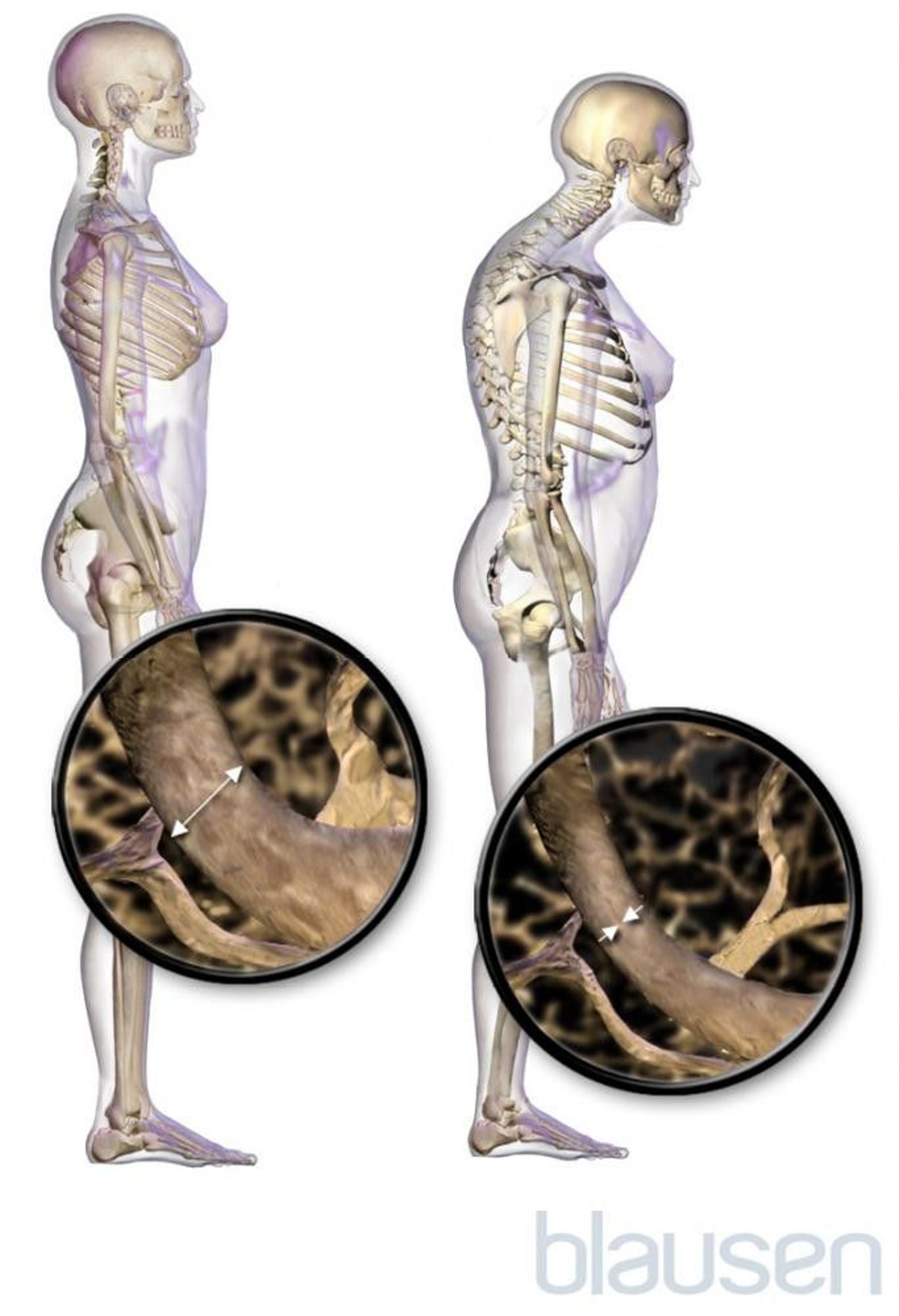
At first, osteoporosis causes no symptoms. Bone density loss occurs very gradually. Some people never develop symptoms. However, when osteoporosis causes bones to break (fracture), people may have pain depending on the location of the fracture. Fractures tend to heal slowly in people who have osteoporosis and may lead to deformities such as curvature of the spine.
In long bones, such as the bones of the arms and legs, the fracture usually occurs at the ends of the bones rather than in the middle. Long bone fractures typically are painful.

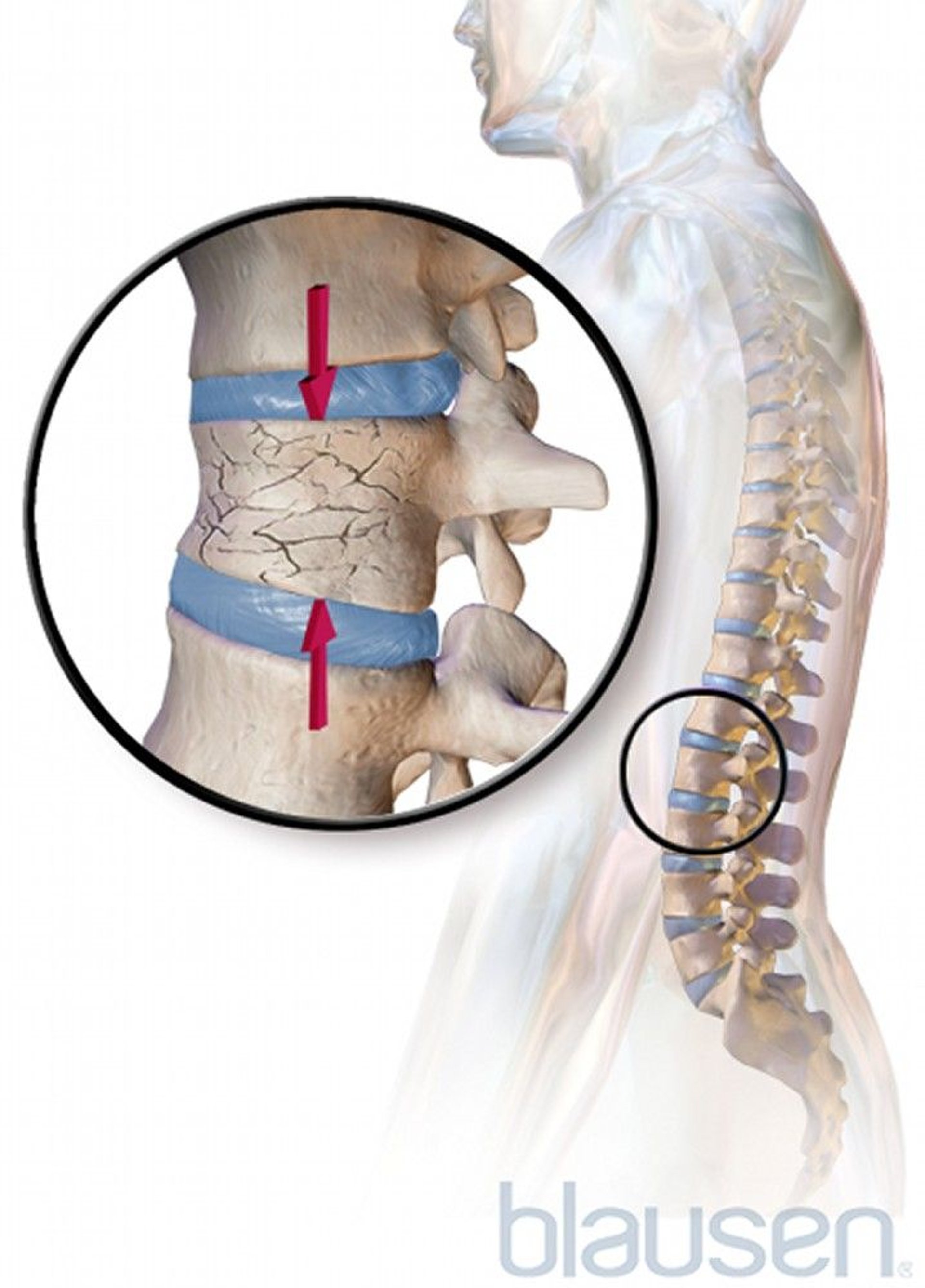
The bones of the spine (vertebrae) are particularly at risk of fracture due to osteoporosis. These fractures are the most common osteoporosis-related fracture. They usually occur in the middle to lower back. Typically, the drum-shaped body of one or more vertebrae collapses into itself and becomes compressed into a wedge shape. These vertebral compression fractures may occur in people who have any type of osteoporosis, including those on medications that cause bone density loss and increased risk of fracture. The weakened vertebrae may collapse spontaneously or after a slight injury, such as with coughing or with a fall from a standing height.
Most of these vertebral compression fractures do not cause pain. However, pain can develop, usually starting suddenly, staying in a particular area of the back, and worsening when a person stands or walks. The area may be tender. Usually the pain and tenderness begin to go away gradually after 1 week. However, lingering pain may last for months or be constant. If several vertebrae break, an abnormal curvature of the spine may develop, causing muscle strain and soreness as well as deformity.


Living Art Enterprises, LLC /SCIENCE PHOTO LIBRARY
Fragility fractures are fractures that result from a relatively minor strain or fall, such as a fall from a standing height or less, including a fall out of bed, that normally would not cause a fracture in a healthy bone. Fragility fractures commonly occur in the wrist, hip, and spine (vertebral compression fractures). Other bones include the upper arm bone (humerus) and the pelvis.
Hip fracture, one of the most serious fractures, is a major cause of disability and loss of independence in older adults, and is associated with reduced survival.
Wrist fractures occur often, especially in people with postmenopausal osteoporosis.
People who have had one fracture in which osteoporosis had been a factor are at much higher risk of having more such fractures.
Fractures of the nose, ribs, collarbone, knee cap, and bones in the feet are not considered osteoporosis-related fractures.
Did You Know...
|
Diagnosis of Osteoporosis
Bone density testing
A fracture caused by something that would not normally cause a fracture, such as falling from a standing height or out of bed (called a fragility fracture)
A doctor may suspect osteoporosis in the following people:
All women age 65 or older
Women between menopause and age 65 who have risk factors for osteoporosis
All men and women who have had a previous fracture caused by little or no force, even if the fracture occurred at a young age
People whose bones appear less dense on x-rays or who have vertebral compression fractures on x-rays
People who are at risk of developing secondary osteoporosis
If osteoporosis is suspected and people have not had x-rays, doctors may order imaging to diagnose a fracture. Certain findings on x-rays suggest osteoporosis, but the diagnosis of osteoporosis is confirmed by bone density testing.
Bone density testing
Bone density testing can be used to detect or confirm suspected osteoporosis, even before a fracture occurs.
Dual-energy x-ray absorptiometry (DXA scan) is the most useful test of bone density. The DXA scan takes high-energy and low-energy x-rays of the spine and hip, which are the sites at which major fractures are likely to occur. The difference between the high- and low-energy x-ray readings allows doctors to calculate bone density. The result is reported as a T-score, which compares a person's bone density to the density of a healthy person of the same sex and race/ethnicity at the age of peak bone mass, which is about age 30. The lower the bone density, the lower the T-score. A T-score of -2.5 or lower defines osteoporosis.
DXA scans are painless, involve very little radiation, and can be completed in about 10 to 15 minutes. They may be useful for monitoring the response to treatment as well as for making the diagnosis of osteoporosis. DXA scans may also reveal osteopenia, a condition in which bone density is decreased but not as severely as in osteoporosis. People who have osteopenia also have an increased risk of fractures. It is important for your doctor to calculate a fracture risk assessment (FRAX) score if you have osteopenia on DXA scan, to provide an estimate of your risk for fracture.
People who are already taking osteoporosis medications (eg, a bisphosphonate, an anabolic agent, denosumab) should have repeat DXA scans to monitor the effectiveness of the treatment. , denosumab) should have repeat DXA scans to monitor the effectiveness of the treatment.
Osteoporosis can also be diagnosed in a person with a fracture from something that would not normally cause a fracture (known as a fragility fracture), even if their bone density test is normal.
Other tests
Blood tests may be done to measure calcium, vitamin D, and levels of certain hormones.
Further testing may be needed to rule out treatable conditions that might lead to osteoporosis. If such a condition is found, the diagnosis is called secondary osteoporosis.
Treatment of Osteoporosis
Calcium and vitamin D
Risk factor modification
Weight-bearing exercise
Medications
Treatment of fractures
Osteoporosis treatment involves risk factor modification, which includes ensuring adequate intake of calcium and vitamin D and engaging in weight-bearing exercises (such as walking, climbing stairs, or weight training, all of which strengthen bones). Other lifestyle modifications, such as avoidance of tobacco or excess alcohol intake as well as fall prevention, are also important strategies to reduce the risk of fracture. Treatment with medications is usually recommended. When treating people who have osteoporosis, doctors also manage conditions and risk factors that can contribute to ongoing bone loss.
Calcium and vitamin D
Consuming an adequate amount of nutrients, particularly calcium and vitamin D, is helpful, especially before maximum bone density is reached (around age 30) but also after this time. Vitamin D helps the body absorb calcium.
All men and women should consume at least 1,000 milligrams of calcium each day. Postmenopausal women, older men, children who are going through puberty, and women who are pregnant or breastfeeding may need to consume 1,200 to 1,500 milligrams each day. Calcium in food is preferred over calcium supplements. Foods rich in calcium include dairy products (such as milk and yogurt), certain vegetables (such as broccoli), nut milks (such as almond milk), and nuts (such as macadamia). See table Amount of Calcium in Some Foods.
However, if people cannot consume the recommended amounts by diet alone, they need to take supplements. Many calcium preparations are available, and some include supplemental vitamin D. The most common supplements are calcium carbonate or calcium citrate. Calcium citrate supplements should be taken by people who take a gastric acid suppressant (for example, an H2 blocker, such as famotidine, or proton pump inhibitor, such as omeprazole, which are used to reduce stomach acid production) or who have had gastric bypass surgery.However, if people cannot consume the recommended amounts by diet alone, they need to take supplements. Many calcium preparations are available, and some include supplemental vitamin D. The most common supplements are calcium carbonate or calcium citrate. Calcium citrate supplements should be taken by people who take a gastric acid suppressant (for example, an H2 blocker, such as famotidine, or proton pump inhibitor, such as omeprazole, which are used to reduce stomach acid production) or who have had gastric bypass surgery.
Amount of Calcium in Some Foods
Food | Serving Size | Approximate Amount of Calcium (in milligrams) |
|---|---|---|
Yogurt, plain, low fat | 8 ounces | 450 |
Yogurt, Greek, plain, low fat | 8 ounces | 260 |
Milk, low fat (1 %) | 1 cup | 310 |
Milk, fat free (skim) | 1 cup | 300 |
Soy beverage (soy milk), unsweetened | 1 cup | 300 |
Almond beverage (almond milk), unsweetened | 1 cup | 440 |
Rice beverage (rice milk), unsweetened | 1 cup | 280 |
Cheese, reduced, low, or fat free (various) | 1½ ounce | 120-490 |
Collard greens, cooked | 1 cup | 270 |
Spinach, cooked | 1 cup | 250 |
Bok choy, cooked | 1 cup | 190 |
Kale, cooked | 1 cup | 180 |
Chard, cooked | 1 cup | 100 |
Tofu, raw, regular, prepared with calcium sulfate | ½ cup | 430 |
Sardines, canned | 3 ounces | 330 |
Grapefruit juice, 100%, fortified | 1 cup | 350 |
Orange juice, 100%, fortified | 1 cup | 350 |
Adapted from the US Department of Agriculture and US Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025. Available at DietaryGuidelines.gov. | ||
People with osteoporosis should consume 400 to 800 international units (IUs) of supplemental vitamin D each day. People with osteoporosis who have vitamin D deficiency may need even higher doses. Sometimes doctors check the level of vitamin D in the blood to determine how much supplemental vitamin D should be taken. The most common food source is fortified foods, mainly cereals and dairy products. Vitamin D is also present in fish liver oils and fatty fish. Supplemental vitamin D is usually given as cholecalciferol, the natural form of vitamin D, or ergocalciferol, the synthetic plant-derived form.
Weight-bearing exercise
Weight-bearing exercise, such as walking and stair-climbing, increases bone density. Exercises that do not involve weight bearing, such as swimming, do not increase bone density but do increase core strength and balance and reduce the risk of falls. Most experts recommend about 30 minutes of weight-bearing exercise daily. A physical therapist can develop a safe exercise program for people and demonstrate how to safely perform daily activities to minimize the risk of falls and spine fractures.
In premenopausal women, high levels of exercise, such as those maintained by athletes, without adequate dietary caloric intake can lead to weight loss and amenorrhea (absence of menstrual cycles), which can cause a reduction in bone density.
Medications
Bisphosphonates (alendronate, risedronate, ibandronate, and zoledronic acid) are useful in treating all types of osteoporosis and are usually the first medications used. Bisphosphonates have been shown to reduce bone turnover and thus reduce bone loss as well as reduce the risk of fractures. Alendronate and risedronate can be taken by mouth (orally). Zoledronic acid can be given by vein (intravenously). Ibandronate can be taken orally or intravenously.(alendronate, risedronate, ibandronate, and zoledronic acid) are useful in treating all types of osteoporosis and are usually the first medications used. Bisphosphonates have been shown to reduce bone turnover and thus reduce bone loss as well as reduce the risk of fractures. Alendronate and risedronate can be taken by mouth (orally). Zoledronic acid can be given by vein (intravenously). Ibandronate can be taken orally or intravenously.
An oral bisphosphonate must be swallowed on an empty stomach with a full glass of water (8 ounces, 250 mL) after arising for the day. No other food, drink, or medication should be consumed for the next 30 to 60 minutes because food in the stomach may decrease the absorption of the medication. Because oral bisphosphonates can irritate the lining of the esophagus, the person must not lie down for at least 30 minutes (60 minutes for ibandronate) after taking a dose. Certain people, including those who have An oral bisphosphonate must be swallowed on an empty stomach with a full glass of water (8 ounces, 250 mL) after arising for the day. No other food, drink, or medication should be consumed for the next 30 to 60 minutes because food in the stomach may decrease the absorption of the medication. Because oral bisphosphonates can irritate the lining of the esophagus, the person must not lie down for at least 30 minutes (60 minutes for ibandronate) after taking a dose. Certain people, including those who havedifficulty swallowing, gastrointestinal symptoms (for example, heartburn or nausea), and certain disorders of the esophagus or stomach, should not take the bisphosphonates orally. These people can be given ibandronate or zoledronic acid intravenously. In addition, the following people should not take bisphosphonates:, gastrointestinal symptoms (for example, heartburn or nausea), and certain disorders of the esophagus or stomach, should not take the bisphosphonates orally. These people can be given ibandronate or zoledronic acid intravenously. In addition, the following people should not take bisphosphonates:
Women who are pregnant or nursing
People who have low levels of calcium in the blood
People who have severe kidney disease
Most people need to take these medications for 3 or 5 years, but some people at particularly high risk for fracture may need to take them longer. How long people need to take a bisphosphonate is determined by the doctor and is based on a person's medical condition and risk factors for fracture. During and after treatment with a bisphosphonate, doctors usually perform periodic tests to determine whether bone mass is decreasing. If bone mass is decreasing after stopping a bisphosphonate, treatment with a bisphosphonate may be restarted or another medication may be initiated.
Osteonecrosis of the jaw is a rare condition that has occurred in some people who take bisphosphonates, denosumab, or romosozumab. In this condition, the jaw bone heals poorly, particularly in people who have had invasive dental work involving the jaw bone. The risk of developing osteonecrosis of the jaw is exceptionally low in people taking bisphosphonates, and the likely benefits of treating osteoporosis to prevent bone fractures usually far outweigh the potential risks. When used as prescribed, bisphosphonates prevent many more fractures than cases of osteonecrosis of the jaw they might cause. People who take bisphosphonates intravenously, who have had radiation therapy to the head and neck to treat cancer, or a combination are at highest risk.
Long-term use of bisphosphonates may increase the risk of developing unusual fractures of the thigh bone (femur). To reduce the risk of these fractures, doctors may have people stop taking bisphosphonates for 1 to 2 years or longer. These planned periods of time are called bisphosphonate holidays or drug holidays. How long a bisphosphonate holiday lasts is carefully considered by doctors. Doctors base the decision on certain factors such as a person's age, DXA scan results, whether they have had fractures, and how likely they are to have a fall. People who are on a bisphosphonate holiday should be routinely monitored for decreasing bone density. Because the risk of fracture does increase while people are on a drug holiday, doctors try to balance the benefits of the bisphosphonates with the possible side effects.
Overall, when used as prescribed, the benefits of bisphosphonates in preventing bone fractures far outweigh the potential risks.
DenosumabDenosumab is similar to the bisphosphonates in that it prevents bone loss. Denosumab is given as an injection under the skin in a doctor's office every 6 months . Like bisphosphonates, denosumab very rarely causes osteonecrosis of the jaw and may increase the risk of developing unusual fractures of the thigh bone. Denosumab has been studied in people with chronic kidney disease and, with appropriate monitoring, has been found to be safe to use. This medication has a boxed warning related to the risk for low blood calcium levels in people with chronic kidney disease receiving this medication; careful guidance and monitoring by a doctor is important. People taking denosumab should not miss doses or undergo a drug holiday because delayed doses or stopping this medication may cause a rapid loss in bone density and increase the risk of vertebral fractures, possibly multiple vertebral fractures.
RaloxifeneRaloxifene is an estrogen-like medication that may be useful in preventing and treating bone loss, but it does not have some of estrogen's negative side effects. Raloxifene is used in people who cannot or prefer not to take bisphosphonates. Raloxifene can reduce the risk of vertebral fractures and may reduce the risk of invasive breast cancer.
Men do not benefit from estrogen but may benefit from testosterone replacement therapy if their Men do not benefit from estrogen but may benefit from testosterone replacement therapy if theirtestosterone level is low.
Hormonal therapy (for example, with estrogen) helps maintain bone density in women and can be used for prevention or treatment. However, because the risks of hormonal therapy may exceed its benefits for many women, hormonal therapy is usually not the treatment option used. Decisions about using estrogen replacement therapy after menopause are complex (see Hormone Therapy for Menopause).
Calcitonin,Calcitonin, which inhibits the breakdown of bone, has been studied for treatment of osteoporosis. Calcitonin has not been shown to reduce fracture risk, but it can help relieve pain caused by vertebral fractures. Calcitonin is usually taken by nasal spray. Its use can decrease blood levels of calcium, so these levels must be monitored.
RomosozumabRomosozumab increases bone density in the hip and lumbar spine and reduces the risk of fracture in postmenopausal women. Romosozumab is given as an injection once a month for 1 year. There is a boxed warning on this medication such that people should not take romosozumab within 12 months after having had a heart attack or stroke.
Anabolic agents (teriparatide and abaloparatide) increase the formation of new bone, increase bone density, and decrease the likelihood of fractures. Teriparatide (a synthetic form of (teriparatide and abaloparatide) increase the formation of new bone, increase bone density, and decrease the likelihood of fractures. Teriparatide (a synthetic form ofparathyroid hormone) and abaloparatide (a medication similar to ) and abaloparatide (a medication similar toparathyroid hormone) are self-injected daily. This therapy is used in some people who:
Develop marked bone loss or new fractures while being treated with a bisphosphonate
Cannot take bisphosphonates
Have unusually severe osteoporosis or many fractures (particularly vertebral fractures)
Have osteoporosis caused by long-term use of steroids (also sometimes referred to as glucocorticoids or corticosteroids)
Romosozumab also acts as an anabolic agent.Romosozumab also acts as an anabolic agent.
Treatment of pain and fractures
Back pain resulting from a vertebral compression fracture can be treated with pain relievers and sometimes moist heat and massage and/or supportive devices (such as back braces). People may be given calcitonin to decrease the pain caused by vertebral fractures. Exercises to strengthen muscles in the back may help relieve chronic back pain. After a fracture, people should usually avoid bed rest and also avoid heavy lifting. As soon as they are able, people should do and/or supportive devices (such as back braces). People may be given calcitonin to decrease the pain caused by vertebral fractures. Exercises to strengthen muscles in the back may help relieve chronic back pain. After a fracture, people should usually avoid bed rest and also avoid heavy lifting. As soon as they are able, people should doweight-bearing exercises.
Fractures resulting from osteoporosis must be treated. For hip fractures, usually the joint is stabilized and often part or all of the hip is replaced surgically. Surgery may be needed for a wrist fracture, or the wrist may need to be placed in a cast. Additionally, people who have had an osteoporosis-related fracture should be treated with an osteoporosis medication and should make sure they consume adequate amounts of calcium and vitamin D.
A collapsed vertebra can be repaired by a procedure called vertebroplasty. In this procedure, a material called methyl methacrylate (MMA)—an acrylic bone cement—is injected into the collapsed vertebra, helping to relieve pain and reduce deformity. Kyphoplasty is a similar procedure, in which a small balloon is used to expand the vertebra before the injection of the MMA. With vertebroplasty and kyphoplasty, deformity may be reduced in the MMA-injected bone, but the risk of fractures in adjacent bones in the spine or ribs does not decrease and may even increase. Other risks may include rib fractures, cement leakage, and possibly heart or lung problems. When these procedures should be done has not been clearly determined.
Prevention of Osteoporosis
Prevention of osteoporosis is generally more successful than treatment because it is easier to prevent loss of bone density than to restore density once it has been lost. Prevention measures are recommended for anyone who has bone loss or who has risk factors for bone loss, regardless of whether they have had an osteoporosis-related fracture. Osteoporosis prevention involves:
Managing risk factors (for example, quitting smoking and avoiding excess alcohol)
Consuming adequate amounts of calcium and vitamin D
Engaging in weight-bearing exercise (such as walking, climbing stairs, or weight training)
Taking certain medications (for some people who already have mild bone loss [osteopenia])
Certain measures can help prevent fractures. Many older adults are at risk of falls because of poor coordination and balance, poor vision, muscle weakness, confusion, and use of medications that cause light-headedness when people stand or of medications that cause confusion. Modifying the home environment for safety and working with a physical therapist to develop an exercise program can help prevent falls. Strengthening exercises, including core strengthening, may help improve balance.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
The National Osteoporosis Foundation: Information about preventing osteoporosis and broken bones and promoting strong bones for life
Drugs Mentioned In This Article



