



- Overview of the Peripheral Nervous System
- Overview of Neuromuscular Junction Disorders
- Amyotrophic Lateral Sclerosis (ALS) and Other Motor Neuron Diseases (MNDs)
- Charcot-Marie-Tooth Disease
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
- Eaton-Lambert Syndrome
- Guillain-Barré Syndrome (GBS)
- Hereditary Neuropathies
- Hereditary Neuropathy With Liability to Pressure Palsies (HNPP)
- Isaacs Syndrome
- Mononeuropathy
- Multiple Mononeuropathy
- Myasthenia Gravis
- Nerve Root Disorders
- Plexus Disorders
- Polyneuropathy
- Spinal Muscular Atrophies (SMAs)
- Stiff-Person Syndrome
- Thoracic Outlet Syndromes (TOS)
Mononeuropathy is damage to a single peripheral nerve.





Pressure on a nerve for a long time is the most common cause of mononeuropathy.
The affected area may tingle, feel prickly, or be numb, and the affected muscle may be weak.
Usually, mononeuropathy is diagnosed based on symptoms and results of a physical examination.
Modifying or stopping the activity that caused the problem and taking pain relievers usually help, but sometimes corticosteroid injections, physical therapy, or surgery is needed.
(See also Overview of the Peripheral Nervous System.)
Causes of Mononeuropathy
Physical injury is the most common cause of a mononeuropathy. Injury is commonly caused by pressure on a nerve, such as the following:
Prolonged pressure on a nerve that runs close to the surface of the body near a prominent bone, such as a nerve in an elbow, a shoulder, a wrist, or a knee (as may occur during a long, deep sleep, especially in people with alcohol use disorder)
Pressure from a misfitting cast or from crutches that fit poorly or that are used incorrectly
Pressure from staying in a cramped position for a long time, as when gardening or when playing cards with the elbows resting on a table

Pressure may also injure nerves when people cannot move for long periods, as when they are under anesthesia for surgery, are confined to bed (particularly older adults), are paralyzed, or have lost consciousness.
Less commonly, nerve injury results from the following:
Accidents
Prolonged exposure to cold or heat
Radiation therapy for cancer
Repeated injuries, such as those due to tight gripping of small tools or to excessive vibration from an air hammer
Infections, such as leprosy or Lyme disease
A pocket of blood (hematoma)
Cancer, which may directly invade a nerve
If the pressure on the nerve is mild, people may feel only pins-and-needles sensations without any weakness. For example, people may hit their elbow (funny bone), or a foot may fall asleep. These episodes can be considered temporary mononeuropathies.
Nerves that run close to the body’s surface near a bone are more vulnerable to injury. For example, the following nerves may be damaged:
Median nerve in the wrist (as occurs in carpal tunnel syndrome)
Peroneal nerve near the knee (resulting in peroneal nerve palsy)
Radial nerve in the upper arm (resulting in radial nerve palsy)
Ulnar nerve in the elbow (resulting in ulnar nerve palsy, as occurs in cubital tunnel syndrome)
Did You Know...
|
Symptoms of Mononeuropathy
Mononeuropathies cause abnormal sensations, including pins-and-needles or loss of sensation, in the area supplied by the injured nerve. Pain and weakness may or may not be present. Occasionally, weakness results in paralysis, which can lead to permanent shortening and stiffening of muscles (contractures).
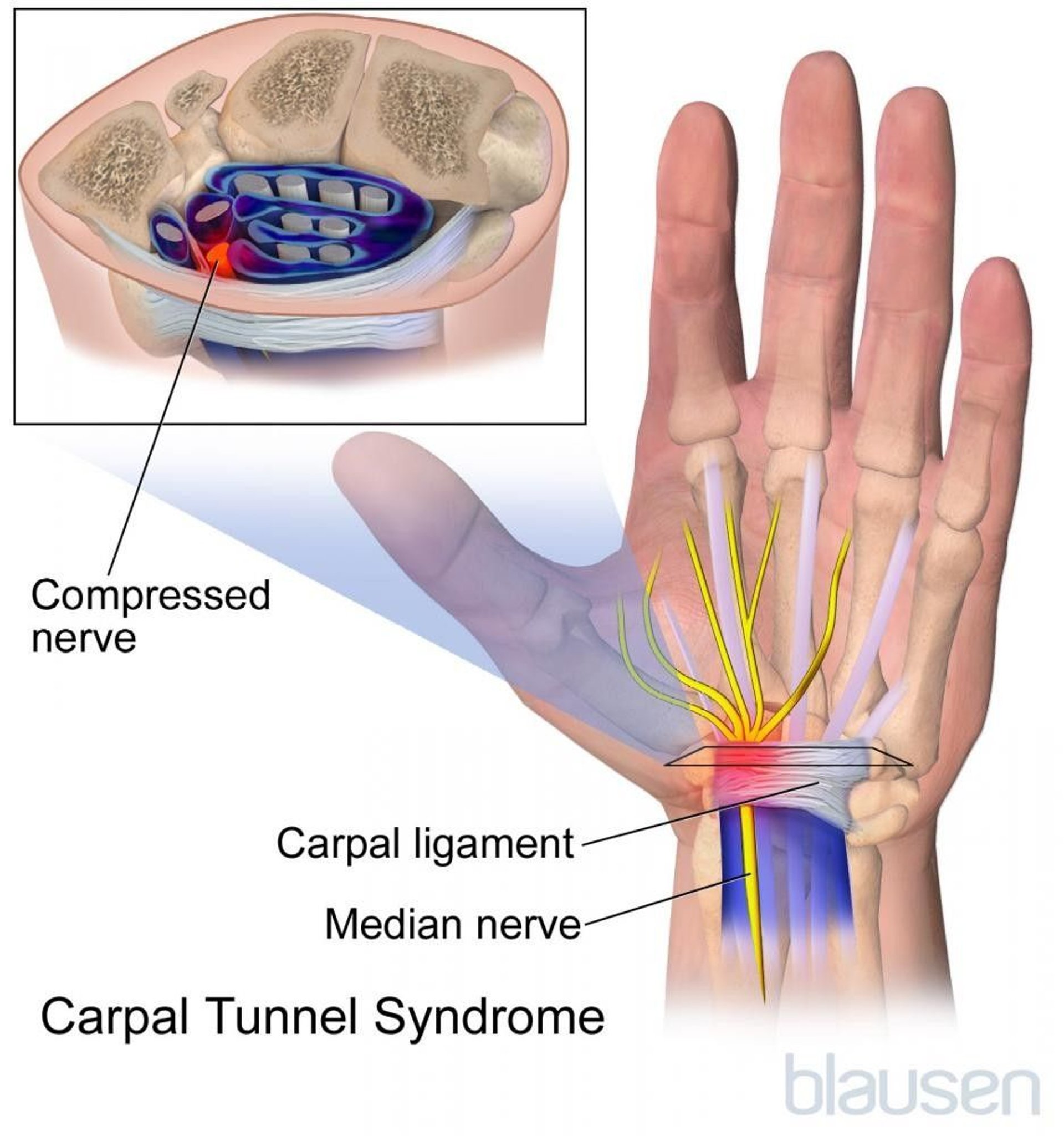
Carpal tunnel syndrome
Carpal tunnel syndrome is the most common mononeuropathy. It results from pressure on the median nerve, which passes through a narrow passageway at the wrist (called the carpal tunnel).
Pregnant women and people who have diabetes, an underactive thyroid gland (hypothyroidism), certain forms of amyloidosis, or rheumatoid arthritis are at increased risk of developing carpal tunnel syndrome. Also at risk are people whose work requires repeated forceful movements with the wrist extended, such as using a screwdriver. Another possible (but controversial) risk factor is use of a computer keyboard that is not positioned correctly. However, most cases develop for unknown reasons.
Pressure on the median nerve causes pain and abnormal sensations (such as numbness, tingling, or burning) in the following:
Some fingers (the thumb, the second and third fingers, and thumb side of the fourth finger)
The palm side of the hand and wrist
Sometimes the arm

Chronic carpal tunnel syndrome can cause muscles in the hand on the thumb side to weaken and waste away (atrophy).
Peroneal nerve palsy
The peroneal nerve passes close to the surface of the skin just below the knee, on the outer side of the leg. Pressure on this nerve results in peroneal nerve palsy.
Peroneal nerve palsy weakens the muscles that lift the foot, so that people cannot flex their ankle to lift the front part of their foot (a condition called footdrop). As a result, they may drag the front part of the foot along the ground as they walk.
Peroneal nerve palsy is most common among thin people who are confined to bed, people who are incorrectly strapped into a wheelchair, and people (especially thin people) who habitually cross their legs for long periods of time.
Avoiding pressure on the nerve—for example, by not crossing the legs—usually relieves the symptoms.
Radial nerve palsy
The radial nerve passes along the underside of the bone in the upper arm. Prolonged pressure on this nerve results in radial nerve palsy. This disorder is sometimes called Saturday night palsy because it occurs in people who drink heavily (often during weekends) and then sleep soundly with an arm resting against a bar counter, draped over the back of a chair, or under their partner’s head. If crutches fit incorrectly and press on the inside of the arm near the armpit, they can cause this disorder.
The nerve damage weakens the wrist and fingers so that the wrist may flop into a bent position with the fingers curved (a condition called wristdrop). Occasionally, the back of the hand may lose feeling.
Usually, radial nerve palsy resolves once the pressure is relieved.
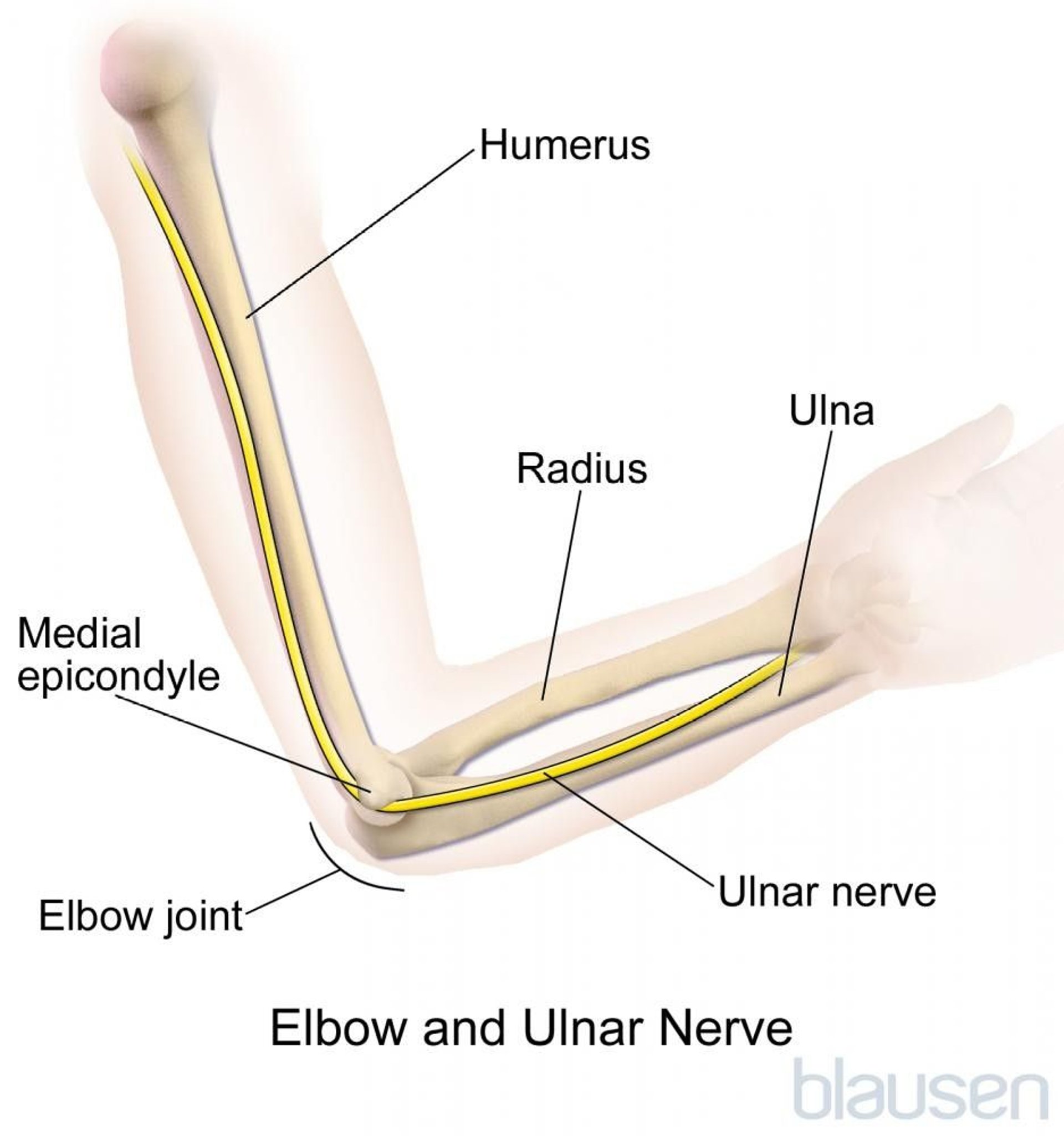
Ulnar nerve palsy
The ulnar nerve passes close to the surface of the skin at the elbow. The nerve is easily damaged by repeatedly leaning on the elbow or by hitting the elbow (funny bone). Sometimes the nerve is damaged by an abnormal bone growth in the area. The ulnar nerve, if damaged and swollen, may be squeezed (compressed) as it passes through a narrow passageway at the elbow (the cubital tunnel). The resulting disorder is called cubital tunnel syndrome. (The ulnar nerve passes through the cubital tunnel as it runs from the upper arm to the wrist and hand.)
Usually, people feel a tingling, pins-and-needles sensation in the little and ring fingers. Ulnar nerve palsy that results from more severe injury makes the muscles in the hand weak. Severe, chronic ulnar nerve palsy can cause muscles to waste away (atrophy), resulting in a clawhand deformity (the fingers are frozen in a bent position because the muscles become tight).
Avoiding pressure on the elbow is recommended.
Diagnosis of Mononeuropathy
A doctor's evaluation
Sometimes electromyography and nerve conduction studies
Usually, doctors can diagnose mononeuropathies based on symptoms and results of a physical examination.
Electromyography and nerve conduction studies are usually done to do the following:
Rule out other possible causes
Determine where the nerve is damaged
Determine how severe the disorder is
Treatment of Mononeuropathy
Treatment of the cause
If pressure is temporary, rest, removal of pressure, and nonsteroidal anti-inflammatory drugs (NSAIDs)
Sometimes corticosteroid injections, a splint, surgery, and/or physical therapy
If the cause of a mononeuropathy is a disorder, it is treated. For example, a tumor may be surgically removed.
Usually, when temporary pressure is the cause, the following can help relieve symptoms:
Resting
Not putting pressure on the nerve
Placing heat on the affected area
Taking NSAIDs, such as ibuprofen, to reduce inflammationTaking NSAIDs, such as ibuprofen, to reduce inflammation
Some people with carpal tunnel syndrome benefit from corticosteroid injections into the carpal tunnel.
Wrist splints, usually worn at night, are often used to treat carpal tunnel syndrome until the symptoms resolve. These devices reduce wrist movements, which cause inflammation and swelling in the carpal tunnel. Thus, the splints reduce pressure on the nerve, and symptoms of carpal tunnel syndrome lessen. Wrist splints should not be worn all day because when movement of the wrist is reduced for a long time, the wrist may become stiff and the muscles may waste away. Splints or braces are less helpful for cubital tunnel syndrome.
Surgery may be done to relieve pressure on a nerve if the disorder progresses despite other treatments. In such cases, surgery for carpal tunnel syndrome is usually effective.
For severe, chronic ulnar nerve palsy, physical therapy helps prevent tightening of muscles.







