



Topic Resources

The thickened muscle creates a partial blockage (obstruction) that interferes with the passage of stomach contents into the small intestine.
Infants feed well but vomit forcefully (projectile vomiting) shortly after eating and can become dehydrated and undernourished.
The diagnosis is based on results of an abdominal ultrasound.
Typically the problem is corrected by fluids given by vein (intravenously) and minor surgery.
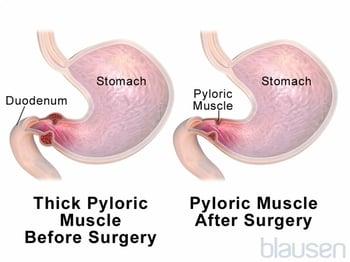
The pylorus is the muscular sphincter located where the stomach joins the first part of the small intestine (duodenum). Normally, the pylorus contracts to keep food in the stomach for digestion and relaxes to let the food out of the stomach and into the intestine. For reasons that doctors do not fully understand, the pylorus becomes thickened and sometimes closes off (called stenosis), blocking material from leaving the stomach. This blockage usually occurs in the first month or two of life.
Risk factors for pyloric stenosis
Risk factors include:
Male sex (especially firstborn boys)
Parents or siblings who had pyloric stenosis
Use of certain antibiotics (for example, erythromycin) during the first few weeks of lifeUse of certain antibiotics (for example, erythromycin) during the first few weeks of life
Smoking during pregnancy
Bottle-feeding with formula
Rarely, some older children have pyloric obstruction caused by swelling due to peptic ulcers or an uncommon disorder similar to a food allergy (such as eosinophilic gastroenteritis).
Symptoms of Hypertrophic Pyloric Stenosis
Symptoms of hypertrophic pyloric stenosis typically develop when an infant is 3 to 6 weeks old.
Infants with pyloric stenosis are hungry and feed well but vomit forcefully (projectile vomiting) shortly after eating. Some infants vomit so much that they become dehydrated and undernourished. Until dehydration is severe, or infants become significantly undernourished, they otherwise appear well.
After several days to weeks, infants become progressively dehydrated and lose weight. Some infants have a yellowish discoloration of the skin and the whites of the eyes (jaundice) at this point.
Diagnosis of Hypertrophic Pyloric Stenosis
Abdominal ultrasound
The doctor may be able to feel a small lump (about the size of an olive) in the infant’s abdomen (the enlarged pylorus). Occasionally, if the infant is observed after feeding and before forcefully vomiting, a wavelike contraction across the abdomen called a peristaltic wave can be seen. Most commonly, however, the doctor does abdominal ultrasound to confirm the diagnosis.
Doctors may do blood tests to evaluate children for dehydration and an electrolyte imbalance (metabolic alkalosis) resulting from severe vomiting.
Treatment of Hypertrophic Pyloric Stenosis
Intravenous fluids
Surgical procedure
Doctors give infants fluids by vein (intravenously) to treat the dehydration and correct any electrolyte imbalance.
Then, a surgeon cuts the thickened muscle to relieve the blockage, allowing formula or breast milk to enter the small intestine more readily. This surgery (called pyloromyotomy) is relatively minor, and most infants can eat within a day of the procedure.

Drugs Mentioned In This Article






