



Hyperthyroidism is increased production of thyroid hormone.
Topic Resources


Graves disease is the most common cause of hyperthyroidism, but growths (nodules) on or inflammation of the thyroid gland, medications, and infections can be causes too.
Symptoms depend on the child's age but typically include speeding up of bodily functions.
The diagnosis is based on blood tests and imaging tests.
Treatment typically includes antithyroid medications and beta-blockers.
(See also Hyperthyroidism in adults.)

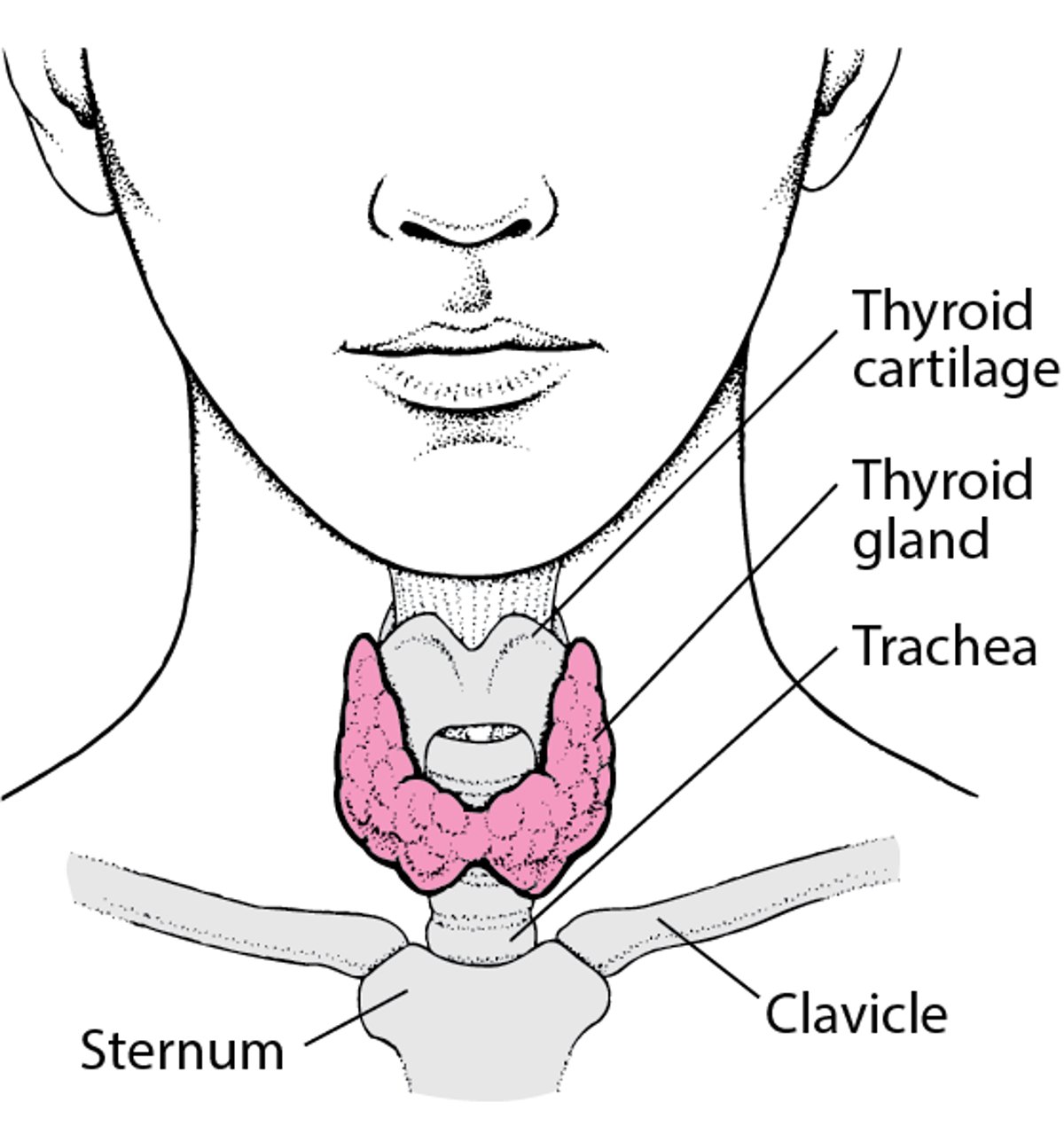
The thyroid gland is an endocrine gland located in the neck. Endocrine glands secrete hormones into the bloodstream. Hormones are chemical messengers that affect the activity of another part of the body.
The thyroid gland secretes thyroid hormone. Thyroid hormone controls the speed of the body's metabolism, including how fast the heart beats and how the body regulates temperature. If the thyroid gland produces too much thyroid hormone, these functions speed up.
Locating the Thyroid Gland

Hyperthyroidism can occur in a developing fetus or newborn or during childhood or adolescence.
Newborns
Hyperthyroidism, or Graves disease in the newborn (neonatal Graves disease), is rare but is potentially fatal if not recognized and treated by a medical doctor who specializes in disorders of the endocrine glands in children (pediatric endocrinologist). This condition usually occurs if the mother has Graves disease during pregnancy or has been treated for it before pregnancy.
In Graves disease, the mother’s body produces antibodies that stimulate her thyroid gland to produce increased amounts of thyroid hormone. These antibodies cross the placenta and also cause the fetus's thyroid gland to produce too much thyroid hormone, which can result in death of the fetus or premature birth.
Because newborns are no longer exposed to the mother's antibodies after birth, Graves disease in the newborn is usually temporary, but the duration varies.
Children and adolescents
The cause of hyperthyroidism in more than 90% of children and adolescents is Graves disease. Graves disease is not common before 5 years of age. The rate of Graves disease increases during puberty and peaks between 10 years and 15 years of age. Many children with Graves disease have a family history of autoimmune thyroid disease or other autoimmune disorders. Children with Down syndrome are at increased risk of Graves disease.
Less common causes of hyperthyroidism in children and adolescents include growths (nodules) on the thyroid gland, inflammation of the thyroid gland (Hashimoto thyroiditis, in which hyperthyroidism is temporary and children eventually develop hypothyroidism), and some medications.
Occasionally, temporary hyperthyroidism can be caused by an infection that causes inflammation of the thyroid gland (thyroiditis). The inflammation may cause the thyroid gland to release excessive amounts of thyroid hormones, resulting in hyperthyroidism. A bacterial infection may cause acute thyroiditis, and a viral infection may cause subacute thyroiditis.
Symptoms of Hyperthyroidism in Infants and Children
Symptoms of hyperthyroidism differ depending on the age of the child.
Fetuses
Hyperthyroidism is rare in a fetus. However, an affected fetus may have symptoms that appear as early as the second trimester.
Affected fetuses have poor growth, a very fast heart rate, and an enlarged thyroid gland (goiter). If the disorder is present and untreated for a long period before birth, it is fatal in about 10 to 15% of newborns others have impaired intellectual development, poor growth, and short stature.
Newborns
An affected newborn has increased bodily functions, such as a rapid heart rate and breathing, irritability, an excessive appetite but poor weight gain, and an abnormally small head (microcephaly). Other symptoms include failure to thrive, vomiting, and diarrhea. The newborn, like the mother, may have bulging eyes (exophthalmos). If the newborn has an enlarged thyroid gland (congenital goiter), the gland may press against the windpipe and interfere with breathing at birth. A very rapid heart rate can lead to heart failure.
Untreated hyperthyroidism may result in early closing of the bones of the skull (craniosynostosis), intellectual disability, growth failure, short stature, and hyperactivity later in childhood.
Children and adolescents
Symptoms of hyperthyroidism reflect the speeding up of bodily functions:
Sleep difficulties
Hyperactivity
Sweating
Fatigue
Weight loss
Increased heart rate and blood pressure
Frequent bowel movements
Tremors (shakiness)
Although bodily functions increase, concentration and school performance decrease. Goiter may be present. Children may have red or bulging eyes.
Symptoms of acute and subacute thyroiditis develop suddenly. Children have pain and tenderness over the thyroid gland and fever. In subacute thyroiditis, these symptoms are less severe, and fever may last for several weeks.
Complications of hyperthyroidism
Thyroid storm is a rare, severe complication of hyperthyroidism and is a life-threatening emergency.
In thyroid storm, the thyroid gland becomes suddenly and extremely active. All body functions are accelerated to dangerously high levels. Symptoms in affected children include an extremely fast heart rate, high body temperature, high blood pressure, heart failure, and changes in mental status. Thyroid storm can lead to coma and death.
Diagnosis of Hyperthyroidism in Infants and Children
Thyroid function tests
Sometimes imaging tests
In newborns, doctors suspect hyperthyroidism if the mother has active Graves disease or a history of Graves disease and high levels of thyroid-stimulating antibodies. Doctors do routine screening blood tests of all newborns in the hospital after birth to evaluate thyroid function. If the screening test is positive, doctors confirm the diagnosis by doing other tests to determine levels of thyroid hormones in the blood (thyroid function tests). After the diagnosis is confirmed, doctors may do imaging tests to evaluate the size and location of the thyroid gland.
In older children and adolescents, doctors also do thyroid function tests. Biotin is a common over-the-counter supplement that can interfere with thyroid function tests by causing false readings of certain hormones. Use of biotin should be stopped for at least 2 days before blood tests are done.
Doctors also do ultrasonography on older children who have Graves disease if the thyroid gland feels asymmetric or they feel a growth (nodule) on the thyroid gland. Computed tomography (CT) or ultrasonography may also be done if doctors suspect a pocket of pus (abscess) or birth defect. If a nodule is found during ultrasonography, doctors remove a piece of it using a needle (called fine-needle aspiration biopsy) to determine whether the child has thyroid cancer. Doctors may also do an imaging test called radionuclide scanning to evaluate a nodule or rule out thyroid cancer.
Treatment of Hyperthyroidism in Infants and Children
Antithyroid medications
Beta-blockers
Sometimes iodine or hydrocortisoneSometimes iodine or hydrocortisone
Sometimes surgery
Children of all ages, including newborns, are given antithyroid medications (such as methimazole), which decrease the thyroid gland's production of thyroid hormones, and sometimes beta-blockers (such as propranolol), which are medications that slow the heart rate. Beta-blockers are used only if the heart rate is too fast or blood pressure is too high. Treatment with beta-blockers is stopped after the antithyroid medications have taken effect. Children of all ages, including newborns, are given antithyroid medications (such as methimazole), which decrease the thyroid gland's production of thyroid hormones, and sometimes beta-blockers (such as propranolol), which are medications that slow the heart rate. Beta-blockers are used only if the heart rate is too fast or blood pressure is too high. Treatment with beta-blockers is stopped after the antithyroid medications have taken effect.
Newborns may also be given iodine or hydrocortisone by mouth if other therapies have not helped. These medications are stopped as soon as the antibodies that cross the placenta from the mother have disappeared from the newborn’s bloodstream. Infants treated with antithyroid medications must be monitored closely to ensure that treatment does not cause Newborns may also be given iodine or hydrocortisone by mouth if other therapies have not helped. These medications are stopped as soon as the antibodies that cross the placenta from the mother have disappeared from the newborn’s bloodstream. Infants treated with antithyroid medications must be monitored closely to ensure that treatment does not causehypothyroidism, which can affect growth and development.
Newborns who have hyperthyroidism almost always recover within 6 months and no longer need antithyroid medications. Symptoms in older children treated with antithyroid medications may eventually disappear (called remission), but symptoms may return (called relapse) in some children, so they are monitored regularly to determine whether they need further treatment.
Sometimes older children (11 years of age and older) with Graves disease need additional treatments to permanently treat the disorder. Permanent treatment (definitive therapy) may be needed if the antithyroid medications do not result in remission after 18 to 24 months of taking them, if the child does not take them, or if they are causing serious side effects. In definitive therapy, the thyroid gland is destroyed with radioactive iodine or removed with surgery. However, radioactive iodine is usually not given to children who are under age 10 and is often not effective in people who have larger thyroid glands. Therefore, surgery may be done instead for children and adolescents who have these factors.
Some nodules are removed surgically.
Acute thyroiditis is treated with antibiotics, and nonsteroidal anti-inflammatory drugs (NSAIDs) are given for pain and fever. Surgery may be needed (for example, to drain an abscess). Subacute thyroiditis is not treated with antibiotics, but NSAIDs are given for pain and fever. Children are not given antithyroid medications for either type of thyroiditis, but beta-blockers may be given.
Thyroid storm is a life-threatening emergency and has an increased risk of death. It is treated in an intensive care unit (ICU) with multiple medications.
Prognosis for Hyperthyroidism in Infants and Children
Newborns who developed hyperthyroidism as a fetus may be severely affected if hyperthyroidism is not detected until birth. Hyperthyroidism is fatal in about 10 to 15% of untreated newborns.
When symptoms start and how severe they are depend on whether the mother is taking antithyroid medications. If the mother did not take antithyroid medications while pregnant, the newborn will have hyperthyroidism at birth. If the mother did take antithyroid medications while pregnant, the newborn may not show symptoms of hyperthyroidism for about 3 to 7 days after birth. (See also treatment of Graves disease during pregnancy.)







