


- Introduction to Diagnosis of Heart and Blood Vessel Disorders
- Medical History and Physical Examination for Heart and Blood Vessel Disorders
- Electrocardiography
- Continuous Ambulatory Electrocardiography
- Echocardiography and Other Ultrasound Procedures
- X-Rays of the Chest
- Computed Tomography (CT) of the Heart
- Positron Emission Tomography (PET) of the Heart
- Magnetic Resonance Imaging (MRI) of the Heart
- Radionuclide Imaging of the Heart
- Tilt Table Testing
- Electrophysiologic Testing
- Stress Testing
- Central Venous Catheterization
- Pulmonary Artery Catheterization
- Cardiac Catheterization and Coronary Angiography
Cardiac catheterization is a procedure that can measure heart function through a catheter inserted into a vein or artery and guided into the heart. Coronary angiography, which can be done during cardiac catheterization, is a type of medical imaging that uses x-rays and a contrast agent to produce images of blood vessels that feed the heart (coronary arteries).
Topic Resources

Cardiac catheterization and coronary angiography are minimally invasive methods of studying the heart and the blood vessels that supply the heart (coronary arteries) without doing surgery. These tests are usually done when noninvasive tests do not give sufficient information, when noninvasive tests suggest that there is a heart or blood vessel problem, or when a person has symptoms that make a heart or coronary artery problem very likely. One advantage to these tests is that during the test, doctors can also treat various diseases, including coronary artery disease.
More than a million cardiac catheterizations and angiographic procedures are done every year in the United States. They are relatively safe, and complications are rare. With cardiac catheterization and angiography, the chance of a serious complication—such as stroke, heart attack, or death—is 1 in 1,000. Fewer than 1 in 10,000 people undergoing these procedures die, and most of those who die already have a severe heart disorder or other disorder. The risk of complications and death is increased for older adults.
Cardiac Catheterization
Cardiac catheterization is used extensively for the diagnosis and treatment of various heart disorders. Cardiac catheterization can be used to measure how much blood the heart pumps out per minute (cardiac output), to detect birth defects of the heart, and to detect and biopsy tumors affecting the heart (for example, a myxoma).

This procedure is the only way to measure directly the pressure of blood in each chamber of the heart and in the major blood vessels going from the heart to the lungs.
In cardiac catheterization, a thin catheter (a small, flexible, hollow plastic tube) is inserted into an artery or vein in the neck, arm, or groin/upper thigh through a puncture made with a needle. A local anesthetic is given to numb the insertion site. The catheter is then threaded through the major blood vessels and into the chambers of the heart and/or into the coronary arteries. The procedure is done in the hospital and takes 40 to 60 minutes.
Various small instruments can be advanced through the tube to the tip of the catheter. They include instruments to measure the pressure of blood in each heart chamber and in blood vessels connected to the heart, to view or take ultrasound images of the interior of blood vessels, to take blood samples from different parts of the heart, or to remove a tissue sample from inside the heart for examination under a microscope (biopsy). Common procedures done through the catheter include the following:
Coronary angiography: A catheter is used to inject a radiopaque contrast agent into the blood vessels that feed the heart (coronary arteries) so that they can be seen on x-rays.
Ventriculography: Ventriculography is a type of angiography in which x-rays are taken as a radiopaque contrast agent is injected through a catheter into the left or right ventricle of the heart. With this procedure, doctors can see the motion of the left or right ventricle and can thus evaluate the pumping ability of the heart. Based on the heart's pumping ability, doctors can calculate the ejection fraction (the percentage of blood pumped out by the left ventricle with each heartbeat). Evaluation of the heart's pumping helps determine how much of the heart has been damaged.
Percutaneous coronary intervention (PCI): A catheter with a balloon attached to the tip is threaded into a narrowed coronary artery and the balloon is inflated to open the narrowed area. Doctors typically use the catheter to insert a wire mesh tube (a stent) into the artery to hold it open.
Valvuloplasty: A catheter is used to widen a narrowed heart valve opening.
Valve replacement: A catheter is used to replace a valve in the heart without removing the old valve or doing surgery.
If an artery is used for catheter insertion, the puncture site must be steadily compressed for 10 to 20 minutes after all the instruments are removed. Compression prevents bleeding and bruise formation. However, bleeding occasionally occurs at the puncture site, leaving a large bruise that can persist for weeks but that almost always goes away on its own. Alternatively, suture devices may be used to close the hole in the artery from the catheter.
Because inserting a catheter into the heart may cause abnormal heart rhythms, the heart is monitored with electrocardiography (ECG). Usually, doctors can correct an abnormal rhythm by moving the catheter to another position. If this maneuver does not help, the catheter is removed. Very rarely, the heart wall is damaged or punctured when a catheter is inserted, and immediate surgical repair may be required.
Cardiac catheterization may be done on the right or left side of the heart.
Catheterization of the right side of the heart
Catheterization of the right side of the heart is done to obtain information about the heart chambers on the right side (right atrium and right ventricle) and the tricuspid valve (located between these two chambers) and evaluate the amount of blood the heart is pumping. The right atrium receives oxygen-depleted blood from the veins of the body, and the right ventricle pumps the blood into the lungs, where blood takes up oxygen and drops off carbon dioxide. In this procedure, the catheter is inserted into a vein, usually in the neck, arm, or the groin.
Right-side catheterization is used to detect and quantify heart function and abnormal connections between the right and left sides of the heart. Doctors also use right-side catheterization when evaluating people for heart transplantation or placing a mechanical device to help pump blood or for diagnosing and treating pulmonary hypertension or heart failure.
Pulmonary artery catheterization, in which a balloon at the catheter's tip is passed through the right atrium and ventricle and lodged in the pulmonary artery (which connects the right ventricle to the lungs), is sometimes done during catheterization of the right side of the heart during certain major operations and in intensive care units.
Catheterization of the left side of the heart
Catheterization of the left side of the heart is done to obtain information about the heart chambers on the left side (left atrium and left ventricle), the mitral valve (located between the left atrium and left ventricle), and the aortic valve (located between the left ventricle and the aorta). The left atrium receives oxygen-rich blood from the lungs, and the left ventricle pumps that blood to the body. This procedure is usually combined with coronary angiography to obtain information about the coronary arteries.
For catheterization of the left side of the heart, the catheter is inserted into an artery, usually in an arm (near the elbow or wrist), neck, or the groin, and passed from that artery into the aorta, the large artery that carries blood from the heart.
Coronary Angiography
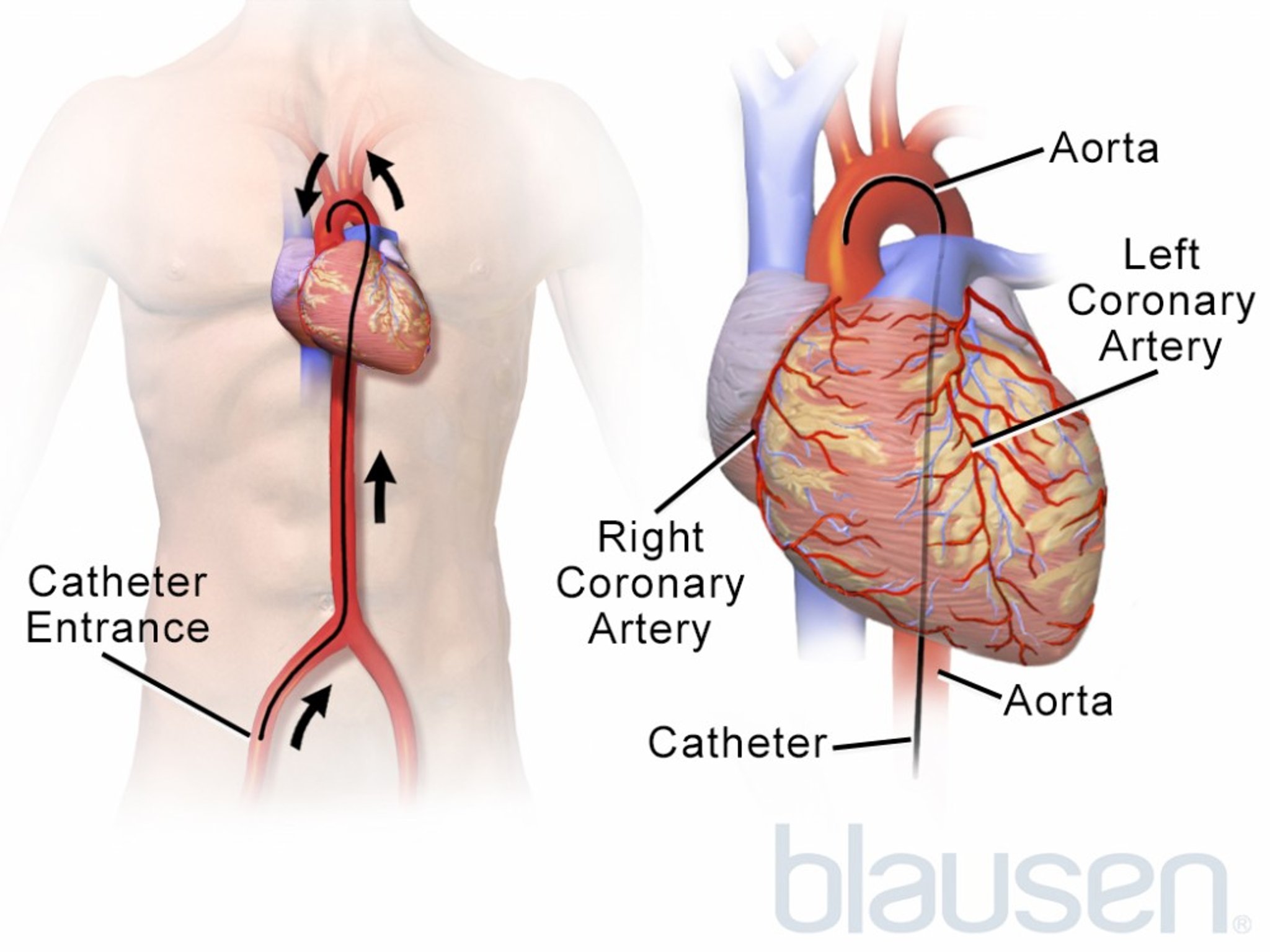
In angiography, a radiopaque contrast agent, which is a liquid that can be seen on x-rays, is injected into a blood vessel and x-rays are taken to produce detailed images of the blood vessel. Coronary angiography provides information about the coronary arteries, which supply the heart with oxygen-rich blood. Coronary angiography is done during cardiac catheterization of the left side of the heart because the coronary arteries branch off the aorta just after it leaves the left side of the heart (see Blood Supply of the Heart). The two procedures are almost always done at the same time.
After injecting a local anesthetic, a doctor inserts a thin catheter into an artery through an incision in an arm (near the elbow or wrist) or the neck or groin. The catheter is threaded toward the heart, then into the coronary arteries. During insertion, the doctor uses fluoroscopy (a continuous x-ray procedure) to observe the progress of the catheter as it is threaded into place.
After the catheter tip is in place, a radiopaque contrast agent is injected through the catheter into the coronary arteries, and the outline of the arteries appears on a video screen and is recorded.
Doctors use these images to detect blockages (coronary artery disease) or spasms of the coronary arteries. Images can help determine whether angioplasty (opening the blockage with a small balloon inserted through the catheters) and stent placement (small, expandable hollow mesh tubes to keep the coronary artery open) is needed or whether coronary artery bypass surgery should be done to get blood past the area of blockage.
Miniature ultrasound transducers on the end of coronary artery catheters can produce images of coronary vessel walls and show blood flow. This technique (intravascular ultrasound or IVUS) is being increasingly used at the same time as coronary angiography. Miniature pressure sensors on the tip of the catheter can determine how much the pressure changes before and after a narrowing in a coronary artery. This technique (called fractional flow reserve or FFR) is used to determine the severity of the blood vessel narrowing.
Coronary angiography is seldom uncomfortable and usually takes 30 to 50 minutes. Unless the person is very ill, the person can go home a short time after the procedure.
When the radiopaque contrast agent is injected into the aorta or heart chambers, the person has a temporary feeling of warmth throughout the body as the contrast agent spreads through the bloodstream. The heart rate may increase, and blood pressure may fall slightly. Rarely, the contrast agent causes the heart to slow briefly or even stop. The person may be asked to cough vigorously during the procedure to help correct such problems, which are rarely serious. Rarely, mild complications, such as nausea, vomiting, and coughing, occur.
Serious complications, such as shock, seizures, kidney problems, and sudden cessation of the heart's pumping (cardiac arrest), are very rare. Side effects of radiopaque contrast agents include allergic reactions and kidney damage. Allergic reactions to the contrast agent range from skin rashes to a rare life-threatening reaction called anaphylaxis. The team doing the procedure is prepared to treat the complications of coronary angiography immediately. Kidney damage almost always goes away on its own. However, doctors are cautious about doing angiography in people who already have impaired kidney function.
Risk of complications is higher in older adults, although it is still low. Coronary angiography is essential when angioplasty or coronary artery bypass surgery is being considered.







