



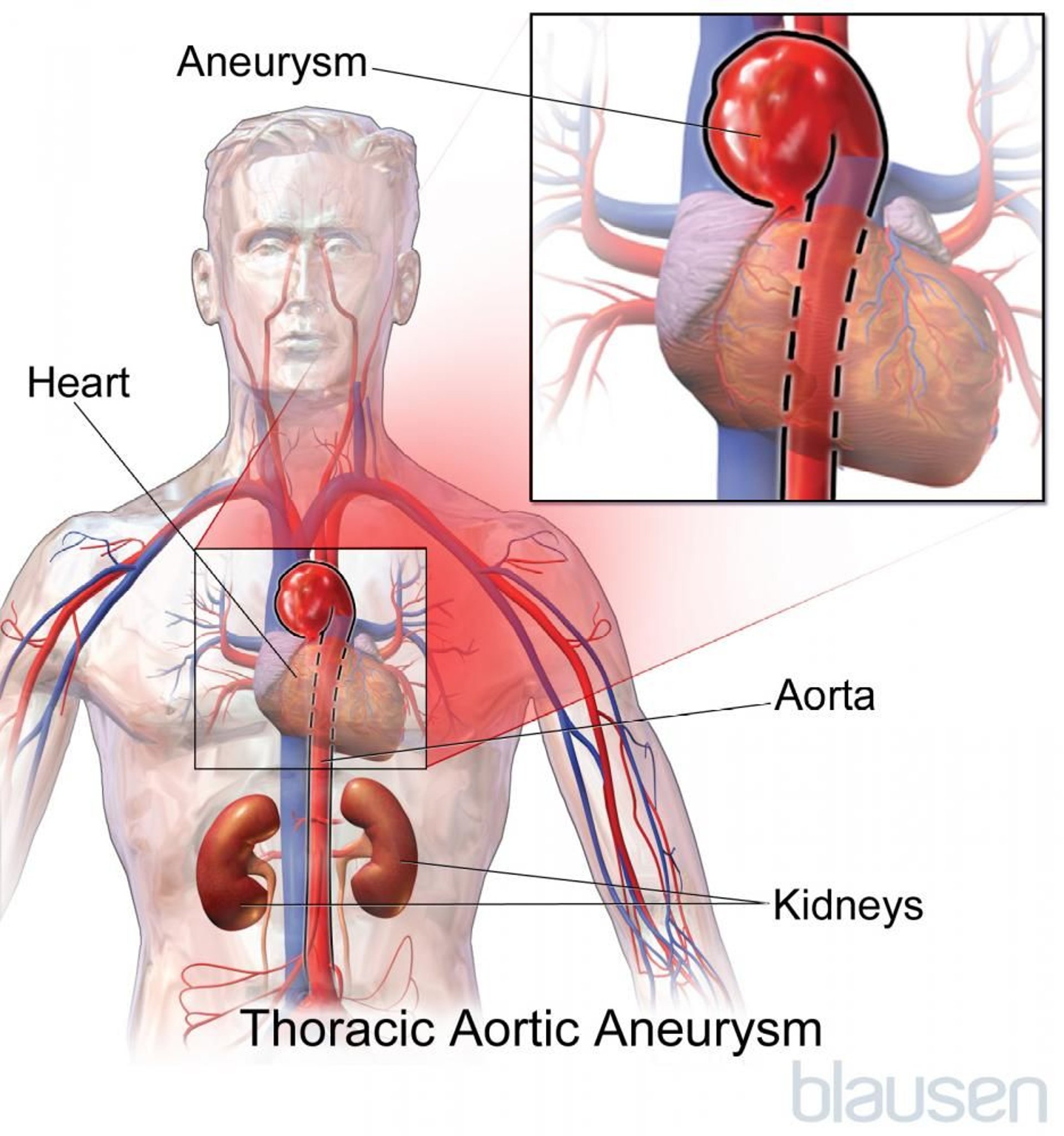
Thoracic aortic aneurysms are bulges (dilations) in the wall of the aorta in the part that passes through the chest (thorax).
Topic Resources

Thoracic aortic aneurysms may not cause symptoms, or they may cause pain, coughing, and wheezing.
Thoracic aortic aneurysms sometimes rupture, which causes excruciating pain (beginning high in the back and spreading down the back and into the abdomen), low blood pressure, and death.
Aneurysms are often discovered by chance during an imaging procedure that is done for another purpose, but doctors do x-rays, computed tomography, or another imaging procedure to determine the size and precise location.
Doctors try to repair aneurysms surgically before the aneurysm ruptures.
(See also Overview of Aortic Aneurysms and Aortic Dissection.)
The aorta is the largest artery of the body. It receives oxygen-rich blood from the heart and distributes it to the body through smaller arteries that branch off of it. The thoracic aorta is the part of the aorta that passes through the chest cavity.
Thoracic aortic aneurysms are sometimes identified incidentally because computed tomography (CT) of the chest is used widely for the diagnosis of other diseases.
Most thoracic artery aneurysms are caused by atherosclerosis.
In another common form of thoracic aortic aneurysm, the walls of the aorta degenerate (a condition called cystic medial necrosis), and the part of the aorta nearest the heart enlarges. This enlargement may cause a malfunction of the valve between the heart and the aorta (aortic valve), allowing blood to leak backward into the heart because the valve cannot close properly. This disorder is called aortic valve regurgitation.
About half of the people with an aneurysm plus cystic medial necrosis also have a connective tissue disorder called Marfan syndrome. In the other half, no cause is apparent, although many of these people have high blood pressure.

Rarely, syphilis causes an aneurysm to form in the part of the aorta nearest the heart. In other cases, bacteria can enter the bloodstream as a result of another infection (usually pneumonia or a urinary tract infection) and attach to a site in the aorta and multiply. This bacterial infection can weaken the aortic wall and result in an aneurysm at that site.
Symptoms of Thoracic Aortic Aneurysms
Thoracic aortic aneurysms may become huge without causing symptoms. When they do occur, symptoms result from the pressure of the enlarging aorta against nearby organs, nerves, or muscles and thus depend on where the aneurysm develops.
Typical symptoms are pain (usually high in the back), coughing, and wheezing. Rarely, a person coughs up blood because of pressure on or erosion of the windpipe (trachea) or nearby airways. Swallowing may be difficult if an aneurysm puts pressure on the esophagus, which carries food to the stomach. Hoarseness may result from pressure on the nerve to the voice box (larynx).
A group of symptoms called Horner syndrome may result from pressure on certain nerves in the chest. Symptoms include a constricted pupil, drooping eyelid, and lack of sweating on one side of the face. Abnormal pulsations felt in the chest may indicate a thoracic aortic aneurysm. A windpipe that is farther to the side than usual may be seen on chest x-rays.
When a thoracic aortic aneurysm ruptures, excruciating pain usually begins high in the back. It may radiate down the back and into the abdomen as the rupture progresses. The pain may also be felt in the chest and arms, as it is during a heart attack. A person can quickly go into shock and die because of internal bleeding.
Diagnosis of Thoracic Aortic Aneurysms
Imaging tests such as CT angiography, magnetic resonance angiography, or transesophageal echocardiography
Doctors may diagnose a thoracic aortic aneurysm based on symptoms, or they may find signs during a routine physical examination that suggest that a thoracic aortic aneurysm is present, such as a particular type of heart murmur (rumbling sound doctors hear when listening with a stethoscope) or physical features of Marfan syndrome.
A chest x-ray study or computed tomography (CT) scan taken for another reason may detect an aneurysm.
Computed tomography (CT) angiography, magnetic resonance angiography, or transesophageal echocardiography (a type of ultrasound in which the ultrasound probe is passed down the throat into the esophagus) is used to determine the precise size of the aneurysm. Aortography or CT angiography is usually done to help doctors determine what type of surgery, if any, is needed.
Treatment of Thoracic Aortic Aneurysms
Medications to reduce high blood pressure
Endovascular stent graft or traditional surgical repair
People with a small thoracic aortic aneurysm are given CT examinations every 6 to 12 months so doctors can monitor the aneurysm and determine whether it is expanding.
Patients are given a beta-blocker, calcium channel blocker, or another antihypertensive medication to reduce the rate at which the aneurysms grows and to reduce the risk that it might rupture. For people who smoke, quitting smoking is very important.
It is much better to treat a thoracic aortic aneurysm before it ruptures, so once it becomes 2½ inches (5.5 to 6.0 centimeters) wide or larger, doctors will recommend repair. In people who have Marfan syndrome, a rupture is more likely, so doctors may recommend surgical repair even for smaller aneurysms.
The choice of aneurysm repair technique depends on many factors, including the person's age and general health and the anatomy of their aorta and aneurysm. In general, stent grafts are the first choice for thoracic aortic aneurysms because they are much less invasive, avoiding an open chest incision that is more painful and that requires longer recovery. Open surgery is less commonly done and generally only necessary when a stent graft does not fit the shape of the aorta.
An endovascular stent graft is a hollow tube composed of fabric supported by a metal mesh that can be placed inside the aorta at the site of the aneurysm. To do an endovascular stent graft, doctors thread a long, thin wire through the large artery in the groin (femoral artery) and up to the area of the aneurysm, Then they slide the stent graft over the wire and advance it to the site of the aneurysm within the aorta. Then they open the stent graft inside the damaged part of the aorta to form a stable channel for blood flow. The stent is left in place permanently. This procedure takes 2 to 4 hours, and the hospital stay is usually shorter than open surgery.
The risk of death is low during stent graft repair of thoracic aortic aneurysms but is higher during a stent graft repair or surgery for a ruptured thoracic aneurysm. Untreated ruptured thoracic aortic aneurysms are always fatal.
If syphilis or another infection is the cause of the aneurysm, doctors give antibiotics to treat the infection. Usually, the aneurysm must also be repaired.







