



Meningococcal infections are caused by the bacteria Neisseria meningitidis (meningococci) and include meningitis and sepsis.




Infection is spread by direct contact with nasal and throat secretions.
People feel generally ill and have other often serious symptoms, depending on the area infected.
Identifying the bacteria in blood or in a sample taken from infected tissue confirms the diagnosis.
Antibiotics and fluids must be given intravenously as soon as possible.
Vaccination can help prevent meningococcal infections.
Most meningococcal infections are
Meningitis: Infection of the tissues covering the brain and spinal cord (meninges)
Sepsis: Infection of the bloodstream (called meningococcemia when caused by meningococci)
Infections of the lungs, joints, eyes, heart, rectum, and organs of the reproductive and urinary systems may occur but are less common.
In temperate climates, most meningococcal infections occur during winter and spring. Local outbreaks can occur, most often in sub-Saharan Africa from Senegal to Ethiopia. This area, which includes 26 countries, is known as the meningitis belt.
Meningococci reside in the throat and nose of some people without causing symptoms. Such people are called carriers. People often become carriers after outbreaks. However, infection usually occurs in people who have not been exposed previously to meningococci, rather than in carriers. Infection is spread by direct contact with nasal and throat secretions of an infected person (including carriers).
The most commonly infected people are
Children aged 6 months to 3 years (see also Meningitis in Children)
Infections are also more common among
Adolescents and young adults (16 to 20 years of age)
Military recruits
First-year college students living in dormitories
Travelers to places where meningococcal disease is common
People with HIV infection
Men who have sex with men
People whose spleen has been removed or damaged
People who do not have enough complement proteins, which support the immune system
People who take eculizumab or ravulizumab (medications that block a component of the immune system called the complement system)
Microbiologists working with meningococci
Close contacts of people who have a meningococcal infection
Other factors that may increase risk of a meningococcal infection include getting a viral infection, living in a crowded household, having a chronic illness, and smoking or being exposed to cigarette smoke (passive smoking).
Outbreaks of meningococcal infection are rare in the United States and account for only a small percentage of cases. Outbreaks tend to occur among people who spend time in or live in close quarters with others, for example, in dormitories, schools, or day care centers, and most often involve people 16 to 23 years of age.
Symptoms of Meningococcal Infections
Most people with a meningococcal infection feel very ill.
Meningitis often causes fever, headache, red rash, and a stiff neck. It can also cause nausea, vomiting, and sensitivity to light.
Infants may have feeding problems and a weak cry, and they may be irritable and sluggish.

© Springer Science+Business Media
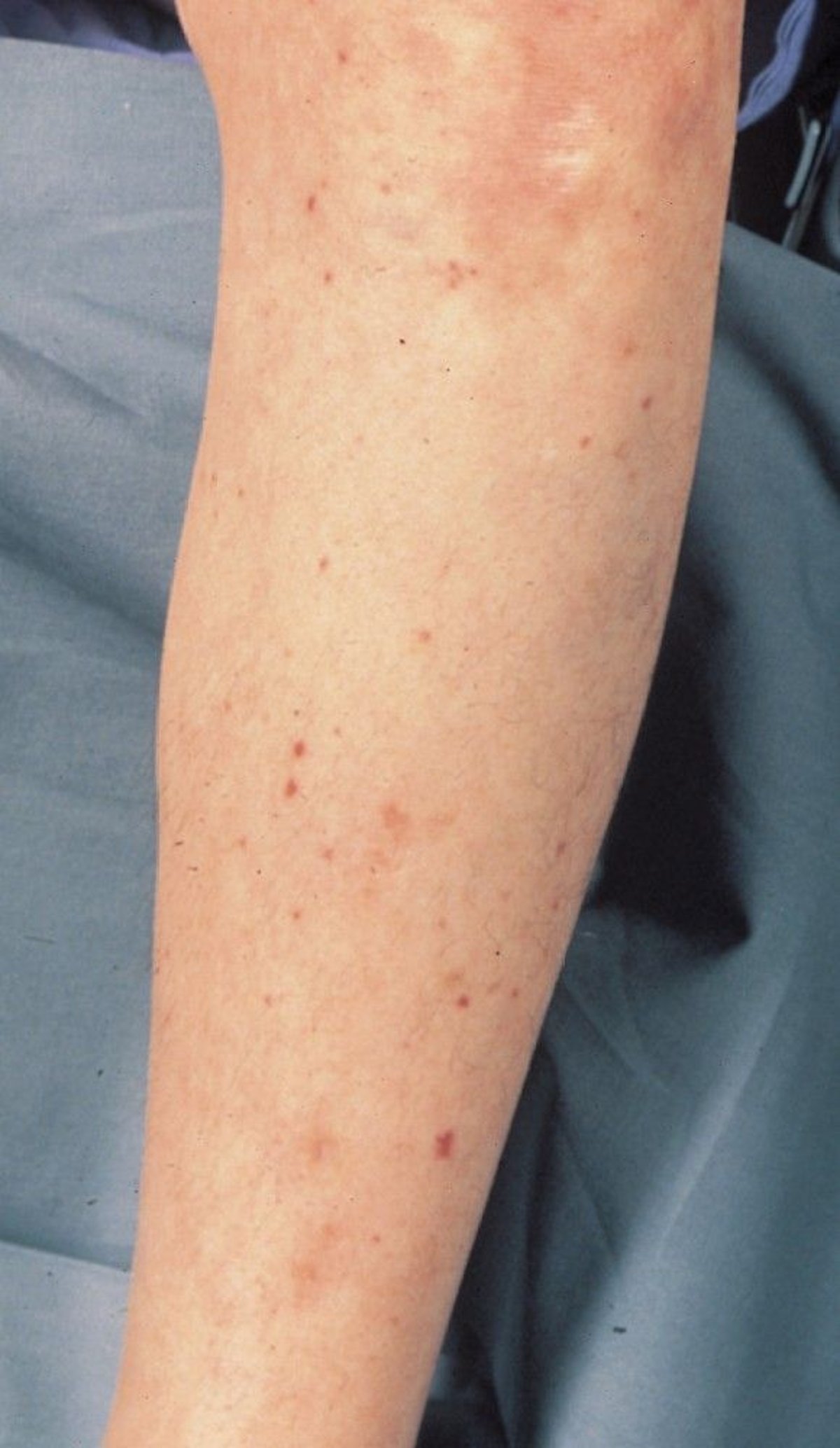
Bloodstream infections may cause a rash of red or purple spots. A severe infection may cause sepsis, which is characterized by dangerously low blood pressure (shock), a tendency to bleed, and dysfunction (failure) of many organs (such as the kidneys and liver).


© Springer Science+Business Media
Rarely, meningococcal infection causes a chronic illness that causes mild, recurring symptoms that mostly involve the joints and skin.
Diagnosis of Meningococcal Infections
Examination and culture of samples of blood or other infected tissues, including cerebrospinal fluid obtained by spinal tap
Sometimes polymerase chain reaction technique
Doctors suspect meningococcal infection in people who have typical symptoms, particularly if symptoms occur during an outbreak.
To confirm the diagnosis, doctors take samples of blood or other infected tissues or do a spinal tap (lumbar puncture) to obtain a sample of the fluid that surrounds the brain and spinal cord (cerebrospinal fluid). The samples are examined under a microscope to check for and identify bacteria. The samples are also sent to a laboratory, where the bacteria can be identified after it is grown (cultured) or other laboratory tests are done.
If the bacteria is difficult to culture or other test results are inconclusive, doctors can do tests to identify pieces of the bacteria’s genetic material. Tests that detect genetic material in microorganisms are called nucleic acid–based tests. Polymerase chain reaction (PCR) technique is an example of this type of test. The PCR technique is done on samples of cerebrospinal fluid, blood, or other infected tissues. It is used to produce many copies of a gene from the bacteria, making the bacteria much easier to identify.

Sometimes doctors do blood tests that detect antibodies to the bacteria or the capsule that encloses the bacteria. However, the results of these tests still have to be confirmed by culture.
The bacteria may also be tested to determine which antibiotics are effective (a process called susceptibility testing).
Treatment of Meningococcal Infections
Antibiotics given by vein (intravenously)
Fluids given intravenously
Possibly corticosteroids
People are usually admitted to an intensive care unit and given antibiotics and fluids intravenously as soon as possible, before doctors get the culture results identifying the organism causing the infection.
If meningococci are confirmed, doctors change the antibiotics to those that tests show are most effective against the bacteria, typically ceftriaxone or penicillin. These antibiotics are given intravenously.If meningococci are confirmed, doctors change the antibiotics to those that tests show are most effective against the bacteria, typically ceftriaxone or penicillin. These antibiotics are given intravenously.
Doctors give corticosteroids (such as dexamethasone) to children and adults who they suspect have meningitis because these medications may decrease the neurologic damage caused by the infection. However, if the meningitis is caused by Doctors give corticosteroids (such as dexamethasone) to children and adults who they suspect have meningitis because these medications may decrease the neurologic damage caused by the infection. However, if the meningitis is caused byNeisseria meningitidis, doctors can typically stop giving corticosteroids because these medications only seem to help people whose meningitis is caused by Streptococcus pneumoniae or Haemophilus influenzae. Corticosteroids may need to be continued in people whose adrenal glands do not make enough of the corticosteroid cortisol.
Prognosis for Meningococcal Infections
Overall, meningococcal meningitis is fatal in 10 to 15% of people.
Severe meningococcal bloodstream infections with septic shock are fatal in up to 40% of people.
Of people who recover from meningococcal meningitis, 10 to 20% have serious complications, such as permanent hearing loss, intellectual disability, or complications of bloodstream infections, including gangrene of the fingers, toes, or limbs, which may require amputation.
Prevention of Meningococcal Infections
After exposure to meningitis
Family members, medical personnel, and other people who have been in close contact with people who have a meningococcal infection should be given an antibiotic to prevent infection from developing. Antibiotics may be given by mouth or by injection.
Vaccination
For more information, see also Meningococcal Vaccine and the vaccine schedules for children and adolescents and adults from the Centers for Disease Control and Prevention (CDC).
During an outbreak, meningococcal vaccine is also given (in addition to antibiotics) to people in close contact with a person who has a meningococcal infection.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
See the following U.S. government sites for comprehensive information on everything from updates on outbreaks and risk factors to educational materials and quick links to related topics:
Centers for Disease Control and Prevention (CDC): Meningococcal Disease




