



Strongyloidiasis is an infection caused by the roundworm (nematode) Strongyloides stercoralis.
Topic Resources
")
Usually, people are infected when they walk barefoot on contaminated soil and the larvae penetrate their skin.
Most people with this infection do not have any symptoms, but some have a rash, cough, wheezing, abdominal pain, diarrhea, and weight loss.
Rarely, a severe, life-threatening infection develops in people who have a weakened immune system because of a disorder (such as cancer) or in people who take medications that suppress the immune system.
Doctors diagnose the infection by finding larvae in a stool sample or by detecting antibodies to Strongyloides in a blood sample and sometimes by examining a sputum sample for larvae and taking chest x-rays.
People are treated with medications used to treat worm infections.
Helminths are parasitic worms that can infect humans and animals. There are 3 types of helminths: flukes (trematodes), tapeworms (cestodes), and roundworms (nematodes). Strongyloides stercoralis is a roundworm.
Strongyloidiasis is one of the major infections that are transmitted via contaminated soil. An estimated 614 million people are infected worldwide.
Strongyloidiasis occurs in warm, moist areas such as the subtropics and tropics, and in rural areas of the southern United States.
Strongyloides worms are sometimes called threadworms.
(See also Overview of Parasitic Infections.)
Transmission of Strongyloidiasis
The cycle of infection begins with adult Strongyloides worms that live in the small intestine of an infected person. The females produce eggs, which hatch and release larvae. Most of theses early-stage larvae are excreted in the person's stool into the soil. After a few days in soil, larvae develop into a form that can cause infection (called filariform larvae). If the larvae come in contact with a person's bare skin, they penetrate it. The larvae migrate by various routes to the small intestine, where they mature into adults in approximately 2 weeks.
The larvae in the soil that do not come in contact with people may develop into adult worms that can reproduce for several generations before their larvae come in contact with a person. These adults are called free-living adults.

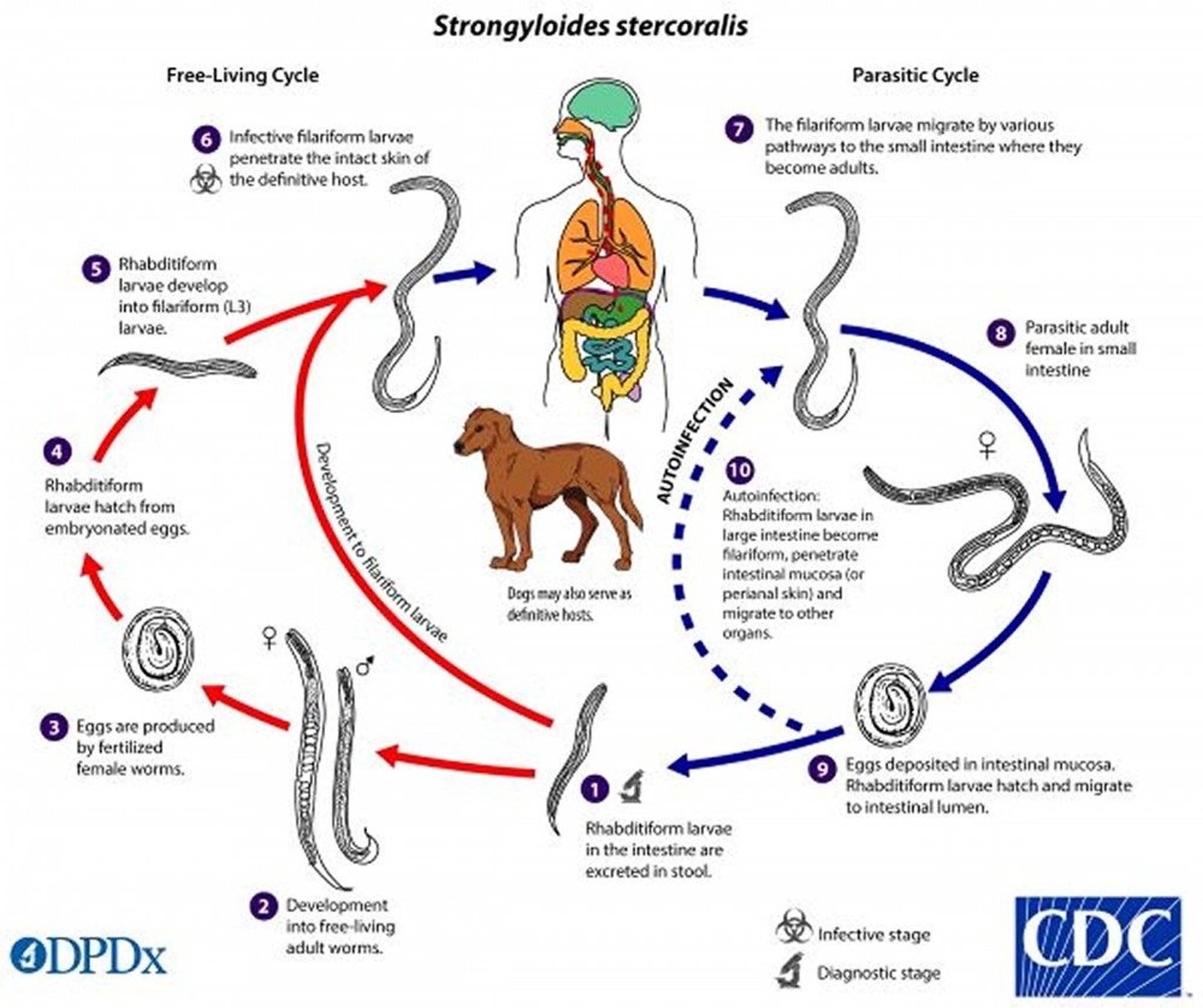
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Autoinfection
Some of the filariform larvae in the intestine can re-infect the person in 1 of 2 ways:
They can penetrate the wall of the intestine and re-enter the person's bloodstream directly.
They can be passed in stool and re-enter the person's body by penetrating the skin around the anus or the skin of the buttocks or thighs.
In both cases, the filariform larvae travel through the bloodstream to the lungs and then to the throat and back to the intestine to cause another infection. This process in called autoinfection (infection of self).
Hyperinfection syndrome and disseminated strongyloidiasis
Rarely, a severe infection called hyperinfection syndrome develops in people who have a new Strongyloides infection or in people who have been reinfected but had no symptoms the first time.
Hyperinfection syndrome affects organs that are involved in the normal Strongyloides life cycle (for example, the intestines, the lungs, and the skin), and can progress to disseminated strongyloidiasis, which can affect organs that are not usually part of the Strongyloides normal life cycle (for example, the liver, the heart, and the brain and spinal cord). Strongyloides larvae may carry bacteria from the digestive tract with them. When the larvae travel through the body, these bacteria can cause infections in the bloodstream, brain and spinal fluid, lungs, or other parts of the body.
Hyperinfection typically affects people who have a weakened immune system because of a disorder (such as cancer) or because they take medications that suppress the immune system (such as prednisone) or medications used to prevent rejection of an organ or bone marrow transplant. However, hyperinfection and dissemination are less common among people who have a weakened immune system because of advanced HIV infection (also called AIDS).Hyperinfection typically affects people who have a weakened immune system because of a disorder (such as cancer) or because they take medications that suppress the immune system (such as prednisone) or medications used to prevent rejection of an organ or bone marrow transplant. However, hyperinfection and dissemination are less common among people who have a weakened immune system because of advanced HIV infection (also called AIDS).
People who have undiagnosed strongyloidiasis may go on to develop hyperinfection or disseminated strongyloidiasis if they are given corticosteroids to treat another disorder.
Symptoms of Strongyloidiasis
Most people with strongyloidiasis do not have symptoms. When symptoms occur, they usually involve the skin, lungs, digestive tract, or a combination of all 3.
People who have an acute infection develop a red, itchy rash caused by the larvae as they travel through the skin. The rash occurs where the larvae entered the skin. People may develop a cough as the larvae travel through the lungs and windpipe (trachea).
People with larvae and adult worms in their digestive tract can have abdominal pain, diarrhea, and loss of appetite.
People who have had strongyloidiasis for a long time may have no symptoms or may have a rash, cough, wheezing, abdominal pain, diarrhea, and constipation. They may not absorb nutrients normally, resulting in weight loss.
Hyperinfection syndrome and disseminated strongyloidiasis
People with hyperinfection syndrome or disseminated strongyloidiasis often have severe symptoms involving the lungs and digestive tract. Lung symptoms include severe shortness of breath, coughing up blood, and respiratory failure. Digestive tract symptoms include intestinal blockage, bleeding, and severe problems absorbing nutrients (malabsorption).
People may have inflammation of the tissues covering the brain and spinal cord (meningitis), an abscess in the brain, or hepatitis.
Bacterial infections, such as a serious infection of the blood (bacteremia) or an infection of the abdominal cavity (peritonitis), may occur.
Hyperinfection syndrome and disseminated strongyloidiasis are often fatal in people with a weakened immune system, even when they are treated.
Diagnosis of Strongyloidiasis
Examination of a stool sample
For hyperinfection syndrome and disseminated strongyloidiasis, examination of stool, a sputum (phlegm) sample, and chest x-rays
Blood tests to detect antibodies to Strongyloides
Doctors can sometimes see Strongyloides larvae when they examine a stool sample under a microscope. Often, they must examine many samples.
Doctors may insert a flexible viewing tube (endoscope) through the mouth into the small intestine to see and take samples of tissue there. A thin tube is threaded through the endoscope and used to suction up samples of tissue.
If doctors suspect hyperinfection syndrome or disseminated strongyloidiasis, they also examine a sputum sample for larvae and take chest x-rays to look for evidence of lung infection.
Doctors also do blood tests to check for antibodies to Strongyloides. (Antibodies are proteins produced by the immune system to help defend against infection, including by parasites.) However, these tests cannot distinguish between new and old infections or between Strongyloides and other roundworm infections.
Eosinophilia is a common result on blood tests. Eosinophilia is a higher than normal number of eosinophils, which are a type of disease-fighting white blood cell that play an important role in the body's response to allergic reactions, asthma, and infection with parasitic worms (helminths).
Doctors may examine stool and test the blood of people who were possibly exposed to Strongyloides to screen them for strongyloidiasis.
Treatment of Strongyloidiasis
Medications used to treat worm infections (anthelmintics)
All people who have strongyloidiasis are treated.
For most cases of strongyloidiasis, doctors give people ivermectin or alternatively albendazole. These medications are known as anthelmintics, and they are taken by mouth.doctors give people ivermectin or alternatively albendazole. These medications are known as anthelmintics, and they are taken by mouth.
Ivermectin is more likely to cure the infection than albendazole. If people with strongyloidiasis have lived in or traveled to areas of Africa where a roundworm called Loa loa is transmitted, doctors check them for Loa loa infection (loiasis) before giving them ivermectin because ivermectin can cause serious brain inflammation (encephalitis) in people who have loiasis and strongyloidiasis at the same time.
For people who have hyperinfection syndrome or disseminated strongyloidiasis, doctors give ivermectin until larvae are not seen in sputum and stool samples for 2 weeks. Hyperinfection syndrome and disseminated strongyloidiasis are life-threatening medical emergencies, so treatment with doctors give ivermectin until larvae are not seen in sputum and stool samples for 2 weeks. Hyperinfection syndrome and disseminated strongyloidiasis are life-threatening medical emergencies, so treatment withivermectin is started immediately.
If people have a weakened immune system, they may need repeated courses of medications.
Antibiotics are used to treat bacterial infections, which may be complications of strongyloidiasis.
To determine whether the infection is eliminated, doctors examine stool samples for larvae . If Strongyloides larvae are still present in stool after treatment, people are treated again.
Prevention of Strongyloidiasis
Prevention of strongyloidiasis involves the following:
Using sanitary toilet facilities
Preventing the skin from directly contacting the soil in areas where strongyloidiasis is common (for example, by wearing shoes and using a tarp or other barrier when seated on the ground)







