



Topic Resources




Kidney failure or high blood pressure may result.
An imaging test can show the narrowing or blockage.
Eliminating a blockage or widening a narrowed artery may be possible and helpful.
(See also Overview of Blood Vessel Disorders of the Kidneys.)
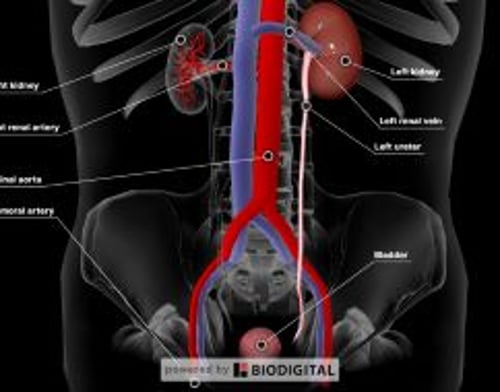
There are 2 renal arteries—one supplies blood to the right kidney, the other to the left kidney. These arteries branch into many smaller arteries.
Causes of Blocked Renal Arteries
Blockage of the renal artery or one of its large or medium-sized branches is unusual. Causes include
Movement of a blood clot from elsewhere in the body into the renal artery
Formation of a blood clot within the renal artery
Tear in the lining of the aorta or renal artery
Thickening of the walls of the renal artery
Most often such blockages occur when a clot moves through the bloodstream from elsewhere in the body (becoming an embolus) and lodges in the renal artery. Typically, such clots originate as fragments from a larger clot in the heart or from the breakup of a fatty deposit (atheroma) in the aorta (see Atheroembolic Kidney Disease).
Alternatively, a blockage may result when a blood clot forms in the renal artery itself, usually where the artery has been injured. A sudden injury may be caused by a medical procedure, such as surgery, angiography, or angioplasty. A clot may also develop where the renal artery has been gradually injured or damaged by atherosclerosis, arteritis (inflammation of arteries), or an aneurysm (a slow-forming bulge in the wall of the artery).
A tear in the lining of the aorta or the renal artery can cause a sudden obstruction of blood flow. A tear may also cause the artery to rupture. Diseases that cause the walls of arteries to become thicker and less elastic because of deposits of fatty material (atherosclerosis) or the development of fibrous material (fibromuscular dysplasia) may predispose vessels to tears. These disorders can lead to significant narrowing and partial blockage of the renal arteries even when there is no blood clot. When narrowing or blockage occurs but no blood clot exists, the condition is called renal artery stenosis.
Fibromuscular dysplasia
Fibromuscular dysplasia is a cause of renal artery blockage. It is a disorder that occurs primarily in women between the ages of 20 and 50 years. Its cause is unknown. In this disorder, fibrous material narrows the renal artery (renal artery stenosis), usually in several sites.
About 10% of all cases of renal artery stenosis in adults are due to fibromuscular dysplasia. Renal artery stenosis due to fibromuscular dysplasia frequently causes high blood pressure.
Symptoms of Blocked Renal Arteries
A partial blockage of the renal arteries usually does not cause any symptoms. If blockage is sudden and complete, the person may have a steady aching pain in the lower back or occasionally in the lower abdomen. A complete blockage may cause fever, nausea, vomiting, and back pain. Rarely, a blockage causes bleeding that turns the urine red or dark brown. Complete blockage of both renal arteries—or of one renal artery in people who have only one kidney—completely stops urine production and shuts down the kidneys (a condition called acute kidney injury).
If a blockage is the result of a clot that has moved to and lodged in one of the renal artery branches, the person may have clots elsewhere in the body, such as in the intestine, brain, and the skin of the fingers and toes. These clots may cause pain in these areas as well as small ulcers or gangrene or a small stroke.
When the blockage develops slowly, symptoms also develop more slowly. The person may develop high blood pressure that is difficult to control despite optimal treatment. Various symptoms of chronic kidney disease may also appear, beginning with fatigue, nausea, loss of appetite, itching, and difficulty concentrating. The symptoms reflect disturbances in the muscles, brain, nerves, heart, digestive tract, and skin.
A gradual narrowing of one or both of the renal arteries may cause high blood pressure or a worsening of previously controlled high blood pressure. Blood pressure may remain high despite treatment with multiple antihypertensive medications. Sometimes, when people with renal artery stenosis are given medications that interfere with the kidney's normal ability to compensate for decreased blood flow (such as angiotensin-converting enzyme [ACE] inhibitors, angiotensin II receptor blockers [ARB], or renin inhibitors) to treat high blood pressure, kidney function may decline rapidly. The effect is reversible if the medication is stopped promptly.
Diagnosis of Blocked Renal Arteries
Routine laboratory tests
Imaging tests
Doctors may suspect a blockage because of the symptoms. Routine laboratory tests, such as a complete blood count, blood tests of kidney function, and urinalysis (microscopic examination of the urine), may add further clues to the diagnosis.

Because none of the symptoms or laboratory tests can specifically identify a blockage, doctors need to do imaging tests of the kidneys. Computed tomography (CT) angiography, magnetic resonance (MR) angiography, Doppler ultrasound, and an isotope perfusion scan can show absent or diminished blood flow to the affected kidney. All of these tests have advantages and disadvantages. For example, CT angiography and MR angiography are very accurate. However, CT angiography involves using an intravenous radiopaque contrast agent, which increases the risk of kidney damage in people with decreased kidney function. MR angiography involves use of an intravenous contrast agent (gadolinium), which increases the risk of nephrogenic systemic fibrosis in people with decreased kidney function. Nephrogenic systemic fibrosis causes scar tissue to form throughout the body and is not easily reversed or cured.
Arteriography is the most accurate test doctors can use to confirm the diagnosis. With arteriography, a catheter is inserted into an artery, which occasionally causes injury to the artery. In addition, as with CT angiography, arteriography involves use of a radiopaque contrast agent that increases risk of kidney damage. Arteriography is done only if doctors are considering surgery or angioplasty to relieve the blockage. Doctors may monitor how well kidney function recovers by repeating blood tests that measure kidney function at frequent intervals.
Sometimes, additional tests such as echocardiography are done to determine the cause of blood clots.
Treatment of Blocked Renal Arteries
Preventing or dissolving blood clots
Sometimes surgery or opening the blockage with a catheter
Treatment is aimed at preventing further deterioration of blood flow and restoring blood flow that has been blocked. In the case of blood clots, the usual treatment is with anticoagulant medications (see Medications and Blood Clots). These drugs are given first intravenously and then by mouth for longer periods of time, sometimes for several months or longer. Anticoagulants prevent the initial clot from enlarging and additional clots from forming. Medications that dissolve clots (fibrinolytics, or thrombolytics—see Medications and Blood Clots) may be more effective than anticoagulants. However, fibrinolytic medications improve kidney function only when the artery is not completely blocked or when clots can be dissolved quickly. After 30 to 60 minutes of complete blockage, permanent damage is likely. Fibrinolytic medications can be helpful only if given within 3 hours.
Surgery is sometimes done to open an artery blocked by a clot, but this treatment has a greater risk of complications and death and does not improve kidney function more than anticoagulant or fibrinolytic medications alone. Treatment with medications is almost always preferred to surgery. However, when the cause is injury, the artery must be surgically repaired.
To relieve a blockage caused by atherosclerosis or fibromuscular dysplasia of a renal artery, doctors may do angioplasty. In angioplasty, doctors thread a catheter with a balloon at the end through the femoral artery in the groin to the renal artery. The balloon is then inflated to force open the obstructed area. This procedure is called percutaneous transluminal angioplasty. When doctors do this procedure, they may place a short hollow tube (stent) in the artery to prevent the blockage from occurring again. When angioplasty is unsuccessful, surgery may be considered to remove or bypass a blockage caused by atherosclerosis or fibromuscular dysplasia.
Although kidney function may improve with treatment, it usually is not restored completely. The outlook is poor when the artery is blocked by clots that have formed in other parts of the body (such as the heart). Clots from that source are likely to travel to other parts of the body (such as the brain or intestine) and cause problems there.
Long-term treatment also focuses on the prevention and treatment of underlying atherosclerosis.

More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
American Association of Kidney Patients (AAKP): AAKP improves the lives of patients through education, advocacy, and promotion of a sense of community among patients with kidney disease.
American Kidney Fund (AKF): AKF provides information about kidney disease and kidney transplant, needs-based financial assistance to help manage medical expenses, webinars for medical professionals, and opportunities for advocacy.
National Kidney Foundation (NKF): This clearinghouse provides everything from information on the basics of kidney function to access to treatment and support for people with kidney disease, continuing medical education courses, and research opportunities and grant support for medical professionals.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): General information on kidney diseases, including research discoveries, statistics, and community health and outreach programs.






