


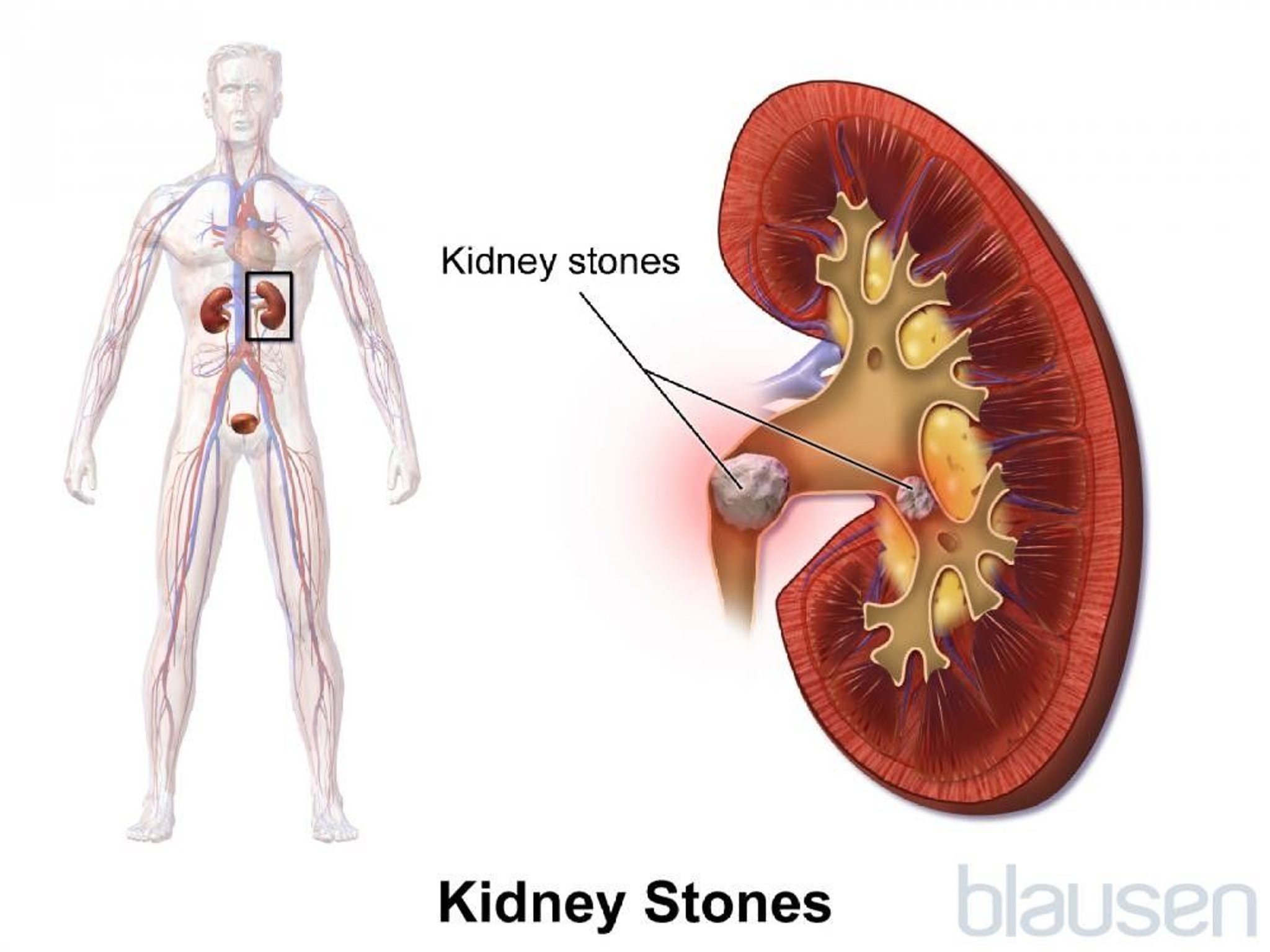
Stones, also called calculi, form in the urinary tract (kidneys, ureters, and bladder) and may cause pain, bleeding, or an infection or block of the flow of urine.
Tiny stones may cause no symptoms, but larger stones can cause excruciating pain in the area between the ribs and hips in the back.
Usually, an imaging test such as a computed tomography (CT) scan and an analysis of urine are done to diagnose stones.
Sometimes stone formation can be prevented by changing the diet or increasing fluid intake.
Stones that do not pass on their own are removed with lithotripsy (the use of shock waves to break up those stones) or an endoscopic technique (the use of specialized tools to view and operate on internal organs without an operation).
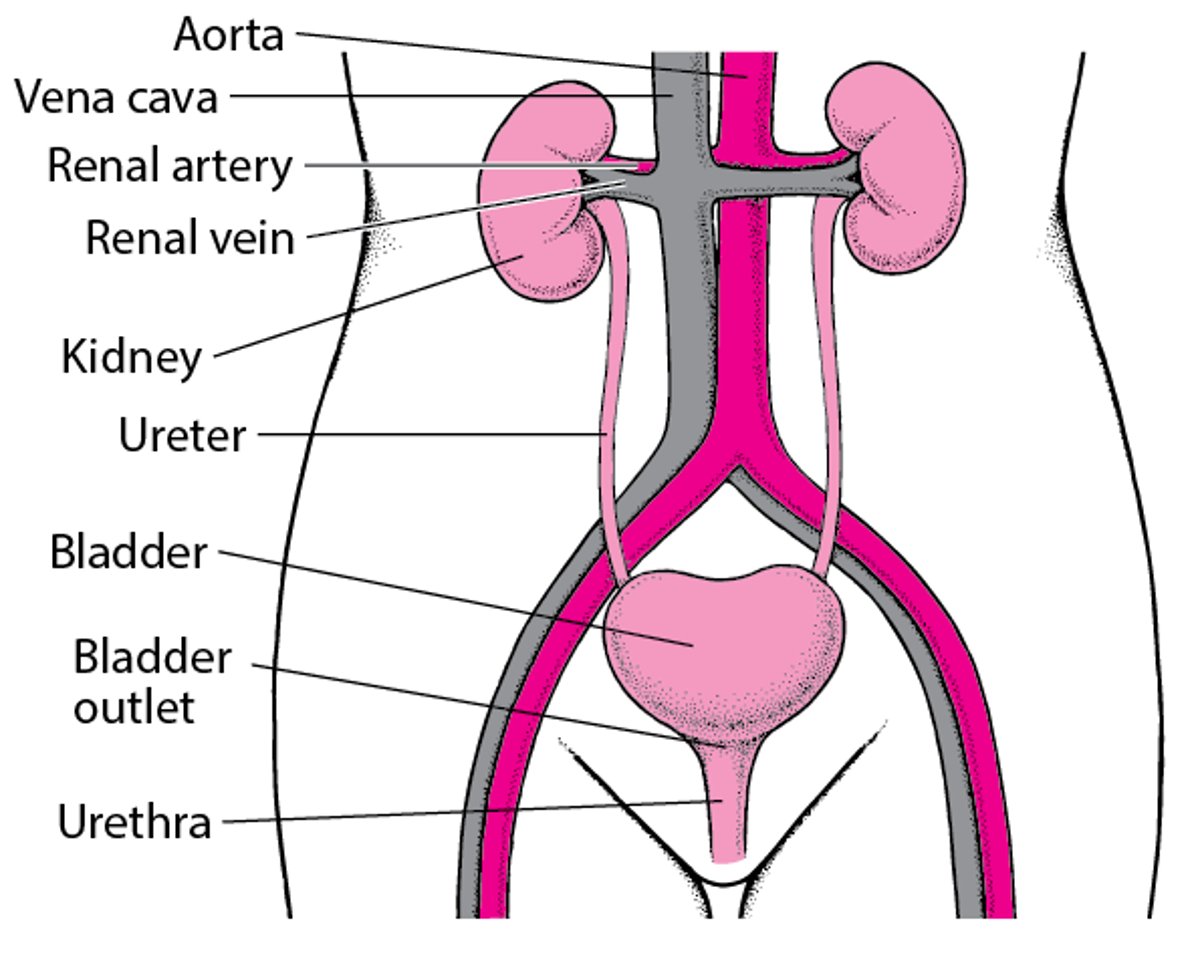
Urinary tract stones form in a kidney and may pass into a ureter or the bladder. Depending on where a stone is located, it may be called a kidney stone, ureteral stone, or bladder stone. The process of stone formation is called urolithiasis, renal lithiasis, or nephrolithiasis.
The Urinary Tract

Every year, about 1 to 2% of adults in the United States are diagnosed with stones in the urinary tract, and about 1 of 1,000 of them are hospitalized. Stones are more common among middle-aged and older adults. Stones vary in size from too small to be seen with the naked eye to 1 inch (2.5 centimeters) or more in diameter. A large, so-called staghorn stone (because its many projections resemble a deer's antlers) may fill almost the entire renal pelvis (the central collecting chamber of the kidney) and the tubes that drain into it (calyces).
Inside the Kidney

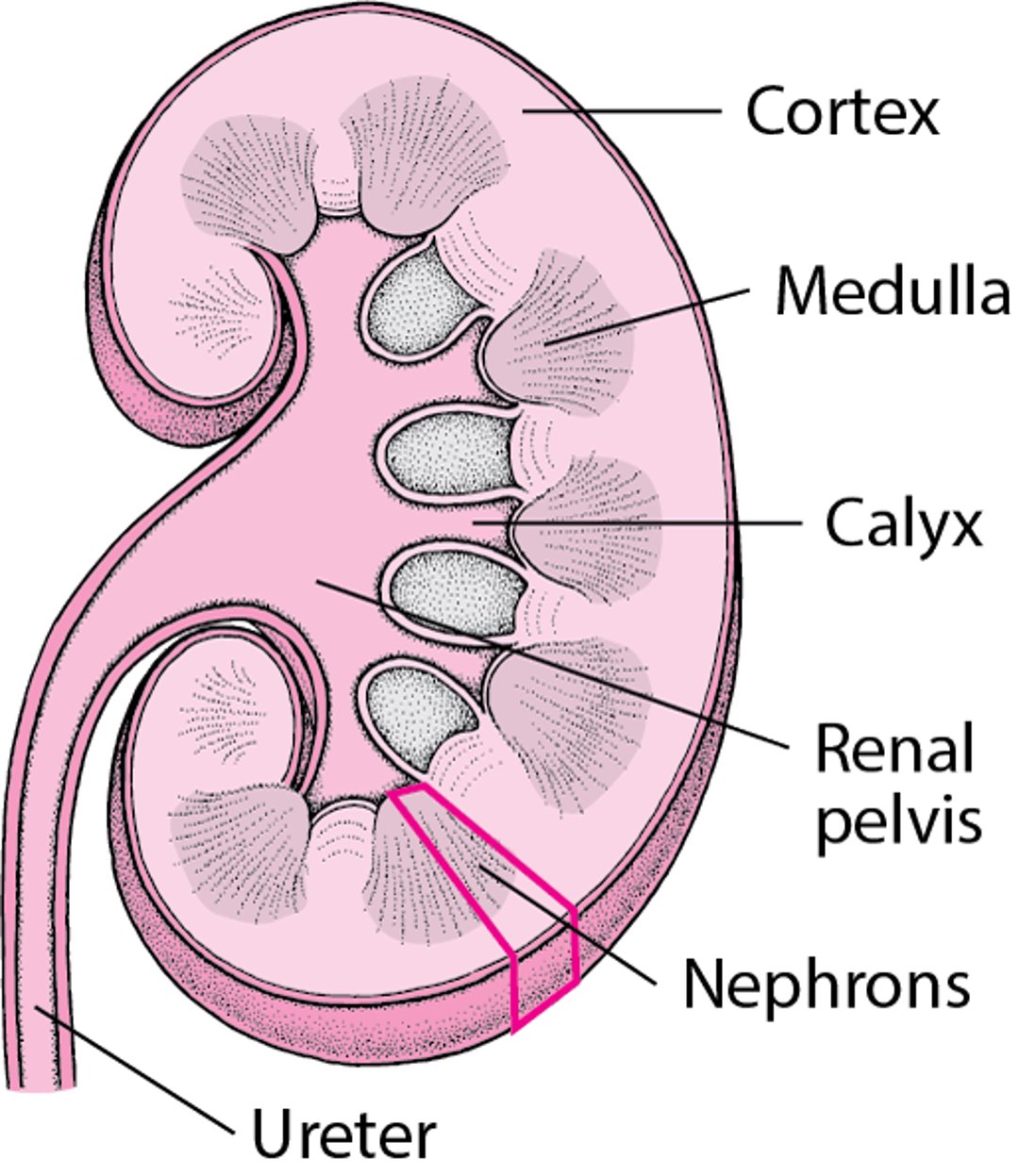



DR. E. WALKER / SCIENCE PHOTO LIBRARY
A urinary tract infection may result when bacteria become trapped in urine that pools above a blockage. When stones block the urinary tract for a long time, urine backs up in the tubes inside the kidney, causing excessive pressure that can cause the kidney to swell (hydronephrosis) and eventually cause damage.
Types of stones
Stones are made of minerals in the urine that form crystals. Sometimes the crystals grow into stones. About 85% of the stones are composed of calcium, and the remainder are composed of various substances, including uric acid, cystine, or struvite. Struvite stones—a mixture of magnesium, ammonium, and phosphate—are also called infection stones, because they form only in infected urine.
Causes of Urinary Tract Stones
Stones may form because the urine becomes too saturated with salts that can form stones or because the urine lacks the normal inhibitors of stone formation. Citrate is such an inhibitor because it normally binds with calcium, which is often involved in forming stones.

Stones are more common among people with certain disorders (for example, hyperparathyroidism, dehydration, and renal tubular acidosis), gout, and type 2 diabetes. Stones in the urinary tract are also found in people whose diet is very high in animal-source protein or vitamin C, as well as in people who do not consume enough water or calcium. People who have a family history of stone formation are more likely to have calcium stones and to have them more often. People who have undergone surgery for weight loss (bariatric surgery) may also be at increased risk of stone formation.
Rarely, medications (including indinavir) and substances in the diet (such as melamine) cause stones.Rarely, medications (including indinavir) and substances in the diet (such as melamine) cause stones.
Symptoms of Urinary Tract Stones
Stones, especially tiny ones, may not cause any symptoms. Stones in the bladder may cause pain in the lower abdomen. Stones that obstruct the ureter or renal pelvis or any of the kidney’s drainage tubes may cause back pain or renal colic. Renal colic is characterized by an excruciating intermittent pain, usually in the area between the ribs and hip on one side, that spreads across the abdomen and often extends to the genital area. The pain tends to come in waves, gradually increasing to a peak intensity, then fading, over about 20 to 60 minutes. The pain may radiate down the abdomen toward the groin or testis or vulva.
Other symptoms include nausea and vomiting, restlessness, and sweating. There may be blood or a stone or a piece of a stone in the urine. A person may have an urge to urinate frequently, particularly as a stone passes down the ureter. Chills, fever, burning or pain during urination, cloudy, foul-smelling urine, and abdominal swelling sometimes occur.
Diagnosis of Urinary Tract Stones
Symptoms
CT scan
Doctors usually suspect stones in people with renal colic. Sometimes doctors suspect stones in people who have tenderness over the back and groin or pain in the genital area without an obvious cause. Finding blood in the urine supports the diagnosis, but not all stones cause blood in the urine. Occasionally, the symptoms and physical examination findings are so distinctive that no additional tests are needed, particularly in people who have had urinary tract stones before. However, doctors need to differentiate stones from other possible causes of severe abdominal pain, including
Peritonitis, which may be caused by appendicitis, ectopic pregnancy, or pelvic inflammatory disease
Acute gallbladder disease (acute cholecystitis)
CT scan is usually the best diagnostic procedure. CT can locate a stone and also indicate the degree to which the stone is blocking the urinary tract. CT can also detect many other disorders that can cause pain similar to the pain caused by stones. The main disadvantage of CT is that it exposes people to radiation. Still, this risk is usually justified when possible causes include another serious disorder that would be diagnosed by CT, such as an aortic aneurysm or appendicitis. Newer CT devices and methods limit exposure to radiation.
Ultrasound is an alternative to CT and does not expose people to radiation. However, compared with CT, ultrasound more often misses small stones (especially when located in the ureter), the exact location of urinary tract blockage, and other serious disorders that could be causing the symptoms.
Did You Know...
|
X-rays of the abdomen expose people to much less radiation than does CT, but x-rays are much less accurate in diagnosing stones and can show only calcium stones. When doctors suspect the person has a calcium stone, x-rays are an alternative to confirm the presence of a stone or to see how far a stone has traveled down the ureter.
Excretory urography (previously called intravenous urography or intravenous pyelography) is a series of x-rays taken after intravenous injection of a dye that is visible on x-ray ("contrast agent"). This test can detect stones and accurately determine the degree to which they are blocking the urinary tract, but it is time-consuming and involves the risks of exposure to the contrast agent (for example, an allergic reaction or worsening of kidney failure). Doctors rarely use excretory urography to diagnose stones if CT or ultrasonography is available.
Urinalysis is usually done. It may show blood or pus in the urine whether or not symptoms are present.
Determining stone type
Once a stone is diagnosed, doctors often do tests to determine the type of stones. People should attempt to retrieve stones that are passed. They can retrieve stones by straining all urine through a paper or mesh filter. Any stone that is found can be analyzed. Depending on the type of stone, urine and blood tests may be necessary to measure levels of calcium, uric acid, hormones, and other substances that may increase the risk of stone formation.
Treatment of Urinary Tract Stones
Nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids as needed to relieve pain
Sometimes stone removal
Small stones that are not causing symptoms, blockage of the urinary tract, or an infection usually do not need to be treated and often pass on their own. Larger stones (over three-sixteenths of an inch [5 mm]) and those that are closer to the kidney are less likely to pass on their own.
Pain relief
The pain of renal colic may be relieved with NSAIDs. If the pain is severe, stronger pain medicine such as opioids are sometimes needed.
Stone-passing strategies
Drinking plenty of fluids or receiving large amounts of fluids intravenously has been recommended to help stones pass, but it is not clear that this approach is helpful. Alpha-adrenergic blockers (such as tamsulosin) may help the stone pass. Once a stone has passed, no other immediate treatment is needed.Drinking plenty of fluids or receiving large amounts of fluids intravenously has been recommended to help stones pass, but it is not clear that this approach is helpful. Alpha-adrenergic blockers (such as tamsulosin) may help the stone pass. Once a stone has passed, no other immediate treatment is needed.
Stone-bypass procedures
Sometimes when a blockage is severe, doctors insert a temporary tube (stent) in the ureter to bypass the obstructing stone. Doctors insert a telescopic viewing instrument (cystoscope, a kind of endoscope) into the bladder and pass the stent through the cystoscope and into the opening of the ureter. The stent is pushed up past the obstructing stone. The stent is left in place until the stone can be removed (for example, by surgery).
Alternatively, doctors may drain the blockage by inserting a drainage tube through the back into the kidney (nephrostomy tube).
Stone removal
Often, shock wave lithotripsy can be used to break up a stone in the renal pelvis or uppermost part of the ureter that is ½ inch (1 centimeter) or less in diameter. In this procedure, shock waves directed at the body by a sound wave generator break up the stone. The pieces of stone are then passed in the urine.
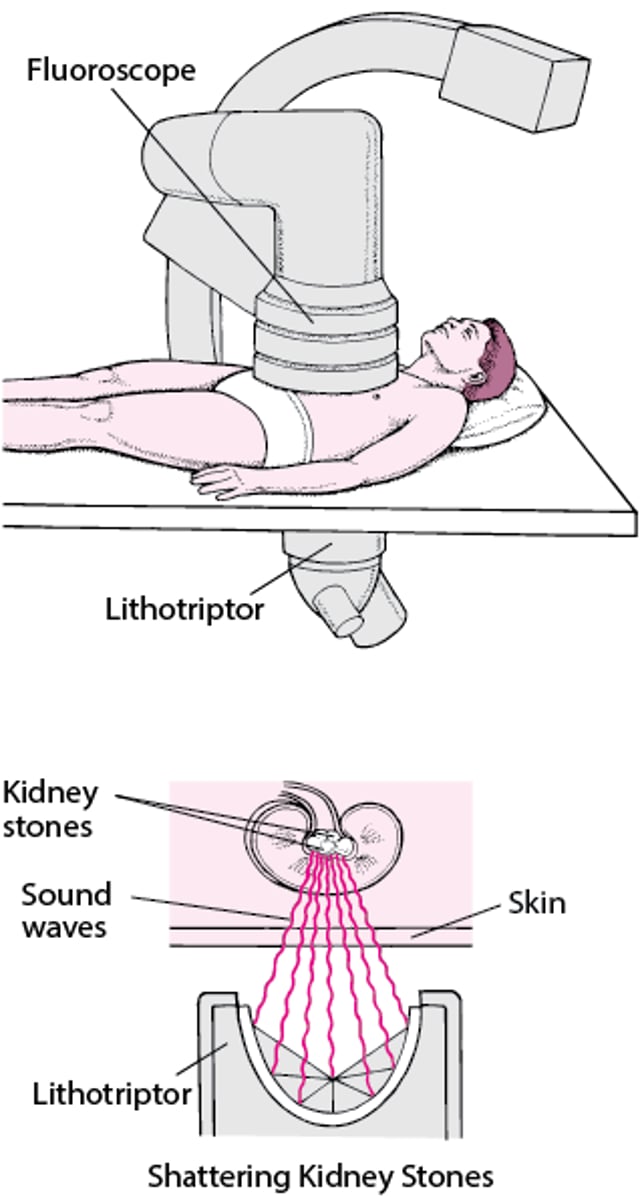
Removing a Stone With Sound Waves
Kidney stones can sometimes be broken up by sound waves produced by a lithotriptor in a procedure called extracorporeal shock wave lithotripsy (SWL). After an ultrasound device or fluoroscope is used to locate the stone, the lithotriptor is placed against the back, and the sound waves are focused on the stone, shattering it. Then the person drinks fluids to flush the stone fragments out of the kidney, to be eliminated in the urine. Sometimes blood appears in the urine or the abdomen is bruised after the procedure, but serious problems are rare. |

A ureteroscope (a small viewing telescope, a kind of endoscope) can be inserted into the urethra, through the bladder, and up the ureter to remove small stones in the lower part of the ureter that require removal. In some instances, the ureteroscope can also be used with a device to break up stones into smaller pieces that can be removed with the ureteroscope or passed in the urine (a procedure called intracorporeal lithotripsy). Most commonly, holmium laser lithotripsy is used. In this procedure, a laser is used to break up the stone.
Percutaneous nephrolithotomy may be used to remove some larger kidney stones. In percutaneous nephrolithotomy, doctors make a small incision in the person's back and then insert a telescopic viewing tube (called a nephroscope, a kind of endoscope) into the kidney. Doctors insert a probe through the nephroscope to break the stone into smaller pieces and then remove the pieces (nephrolithotripsy).
Making the urine more alkaline (for example, with potassium citrate taken for 4 to 6 months by mouth) may sometimes gradually dissolve uric acid stones. Other types of stones cannot be dissolved this way. (for example, with potassium citrate taken for 4 to 6 months by mouth) may sometimes gradually dissolve uric acid stones. Other types of stones cannot be dissolved this way.
Surgical removal is sometimes needed for larger stones that are causing an obstruction.
Endoscopic surgery is usually used to remove struvite stones. Antibiotics are not helpful in treating urinary tract infections until these stones are completely removed.
Ureteral stenting is the placement of a soft hollow tube to help urine drain from the kidney to the bladder. A ureteral stent may be necessary for 4 to 7 days after a procedure done to remove a stone. If there is a ureteral injury caused by either an obstructing stone or the removal of that stone, the stent may be left in place for 1 to 2 weeks. Irritation from the stone or from the removal procedure could cause some inflammation of the ureter. The stent helps the inflammation resolve.
Prevention of Urinary Tract Stones
In a person who has passed a calcium stone for the first time, the likelihood of forming another stone is about 11% at 2 years, and 39% at 15 years. Measures to prevent the formation of new stones vary, depending on the composition of the existing stones.
Drinking large amounts of fluids—8 to 10 ten-ounce (300-milliliter) glasses a day—is recommended for prevention of all stones. People should drink enough fluid to produce more than about 2 quarts of urine per day. Other preventive measures depend somewhat on the type of stone.
Calcium stones
People with calcium stones may have a condition called hypercalciuria, in which excess calcium is excreted in the urine. For these people, measures that decrease the amount of calcium in the urine can help prevent formation of new stones. One such measure is a diet that is low in sodium and high in potassium. Calcium intake should be about normal—1,000 to 1,500 milligrams daily (about 2 to 3 servings of dairy per day). The risk of a new stone forming is actually higher if the diet contains too little calcium, so people should not try to eliminate calcium from their diet. However, people may need to avoid sources of excess calcium, such as antacids that contain calcium.
Thiazide diuretics, such as chlorthalidone or indapamide, also reduce the concentration of calcium in the urine in such people. Potassium citrate may be given to increase a low urine level of citrate, a substance that inhibits calcium stone formation. Restricting animal protein in the diet may help reduce urinary calcium and the risk of stone formation in many people with calcium stones. Thiazide diuretics, such as chlorthalidone or indapamide, also reduce the concentration of calcium in the urine in such people. Potassium citrate may be given to increase a low urine level of citrate, a substance that inhibits calcium stone formation. Restricting animal protein in the diet may help reduce urinary calcium and the risk of stone formation in many people with calcium stones.
Did You Know...
|
A high level of oxalate in the urine, which contributes to calcium stone formation, may result from excess consumption of foods high in oxalate, such as rhubarb, spinach, cocoa, nuts, pepper, and tea, or from certain intestinal disorders (including some kinds of weight loss surgery). Calcium citrate, cholestyramine, and a diet that is low in fat and in oxalate-containing food may help to reduce urinary oxalate levels in some people. Pyridoxine (vitamin B6) decreases the amount of oxalate the body makes.A high level of oxalate in the urine, which contributes to calcium stone formation, may result from excess consumption of foods high in oxalate, such as rhubarb, spinach, cocoa, nuts, pepper, and tea, or from certain intestinal disorders (including some kinds of weight loss surgery). Calcium citrate, cholestyramine, and a diet that is low in fat and in oxalate-containing food may help to reduce urinary oxalate levels in some people. Pyridoxine (vitamin B6) decreases the amount of oxalate the body makes.
In rare cases, calcium stones result from medical conditions such as hyperparathyroidism, sarcoidosis, vitamin D toxicityvitamin D toxicity, renal tubular acidosis, or cancer, and the underlying disease must be treated.
Uric acid stones
Uric acid stones are almost always caused by excessive acid levels in the urine. Potassium citrate should be given to all people who have uric acid stones to make the urine alkaline and neutralize the high acid levels that cause uric acid stones. Occasionally, a low animal protein diet or allopurinol may be used to reduce uric acid levels in the urine. Maintaining a large fluid intake is also very important.Uric acid stones are almost always caused by excessive acid levels in the urine. Potassium citrate should be given to all people who have uric acid stones to make the urine alkaline and neutralize the high acid levels that cause uric acid stones. Occasionally, a low animal protein diet or allopurinol may be used to reduce uric acid levels in the urine. Maintaining a large fluid intake is also very important.
Cystine stones
For stones made of cystine, urinary cystine levels must be kept low by maintaining a large fluid intake and sometimes taking alpha-mercaptopropionylglycine (tiopronin) or penicillamine.For stones made of cystine, urinary cystine levels must be kept low by maintaining a large fluid intake and sometimes taking alpha-mercaptopropionylglycine (tiopronin) or penicillamine.
Struvite stones
People with recurrent struvite stones may need to take antibiotics continually to prevent urinary tract infections. Acetohydroxamic acid may also be helpful in people with struvite stones.. Acetohydroxamic acid may also be helpful in people with struvite stones.




