



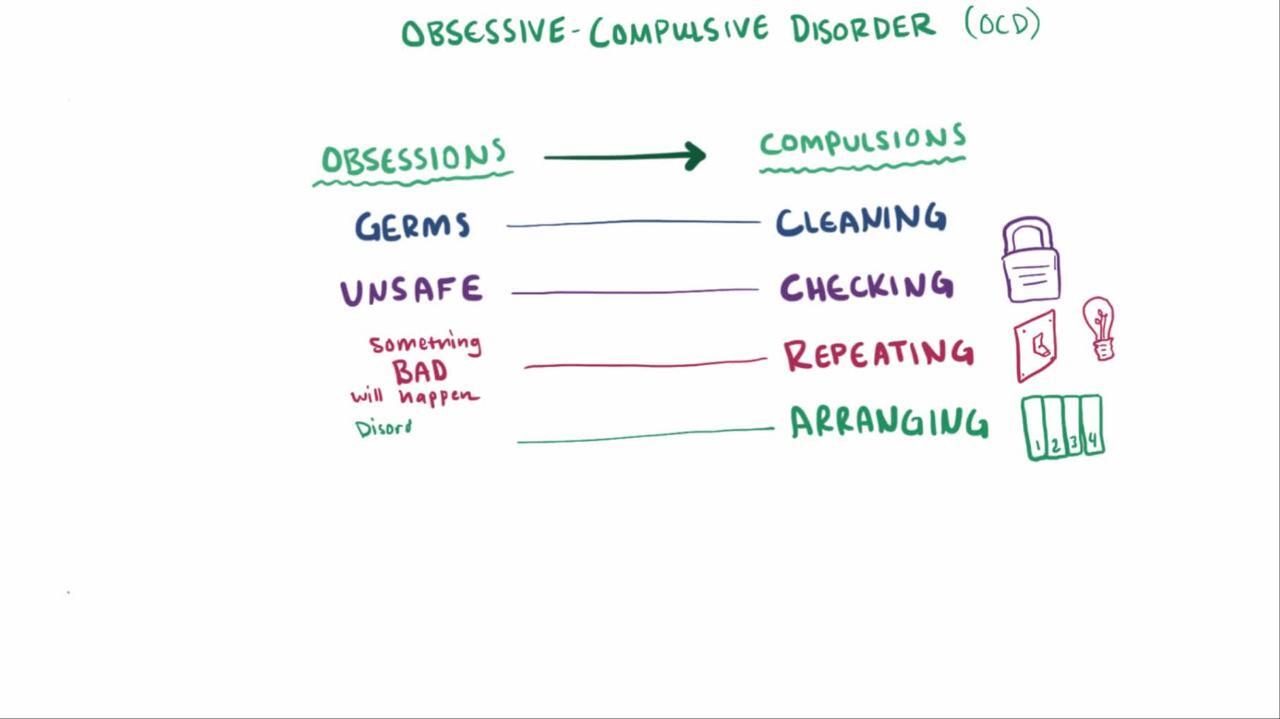
Obsessive-compulsive disorder is characterized by obsessions, compulsions, or both. Obsessions are recurring, persistent, unwanted, anxiety-provoking, intrusive ideas, images, or urges. Compulsions (also called rituals) are certain actions or mental acts that people feel driven to repeatedly perform to try to lessen or prevent the anxiety caused by the obsessions.
Topic Resources
")
Many obsessive-compulsive thoughts and behaviors are related to concerns about harm or risk.
Doctors diagnose the disorder when a person has obsessions, compulsions, or both.
Treatment may include exposure therapy (with prevention of compulsive rituals) and certain antidepressants (selective serotonin reuptake inhibitors or clomipramine).Treatment may include exposure therapy (with prevention of compulsive rituals) and certain antidepressants (selective serotonin reuptake inhibitors or clomipramine).
Obsessive-compulsive disorder (OCD) is slightly more common among women than men and affects about 1 to 2% of the population. On average, OCD begins at about age 19 to 20 years, but about 25% of cases begin by age 14 (see also Obsessive-Compulsive Disorder in Children and Adolescents). Up to 30% of people with OCD have had or have a tic disorder.
OCD differs from psychotic disorders, which are characterized by loss of contact with reality, although in a very small minority of OCD cases there is no insight. OCD also differs from obsessive-compulsive personality disorder, although people with these disorders may have some of the same characteristics, such as being orderly, reliable, or perfectionistic.

Symptoms of OCD
People with obsessive-compulsive disorder (OCD) have obsessions—thoughts, images, or urges that occur over and over even though people do not want them to. These obsessions intrude even when people are thinking about and doing other things. Also, obsessions usually cause great distress or anxiety. The themes of the obsessions include harm (to self or others), cleaning or contamination, forbidden or taboo thoughts (for example, aggressive or sexual obsessions), and the need for symmetry.
Common obsessions include the following:
Concerns about contamination (for example, worrying that touching doorknobs will cause disease)
Doubts (for example, worrying that the front door was not locked)
Concern that items are not perfectly lined up or even
Because the obsessions are not pleasurable, people often try to ignore and/or control them.
Compulsions (also called rituals) are one way people respond to their obsessions. For example, they may feel driven to do something—repetitive, purposeful, and intentional—to try to prevent or relieve the anxiety caused by their obsessions.
Common compulsions include the following:
Washing or cleaning to be rid of contamination
Checking to allay doubt (for example, checking many times to make sure a door is locked)
Counting (for example, repeating an action a certain number of times)
Ordering (for example, arranging tableware or workspace items in a specific pattern)
Most rituals, such as excessive handwashing or repeated checking to make sure a door has been locked, can be observed. Other rituals, such as repetitive counting in one's mind or quietly mumbling statements intended to diminish danger, cannot be observed.
Rituals may have to be done in a precise way according to rigid rules. The rituals may or may not be logically connected to the obsession. When compulsions are logically connected to the obsession (for example, showering to avoid being dirty or checking the stove to prevent fire), they are clearly excessive. For example, people may shower for hours each day or always check the stove 30 times before they leave the house. All obsessions and rituals are time-consuming. People may spend hours each day on them. They may cause so much distress or interfere with functioning so much that people are incapacitated.
Most people with OCD have both obsessions and compulsions.
Most people with OCD are at least somewhat aware that their obsessive thoughts do not reflect actual risks or reality and that their compulsive behaviors are excessive. However, a few people are convinced that their obsessions are well-founded and that their compulsions are reasonable.
Most people with OCD are aware that their compulsive behaviors are excessive. Thus, they may perform their rituals secretly, even though the rituals may occupy several hours each day.
As a result of OCD symptoms, relationships may deteriorate, and people with OCD may do less well in school, at work, or in other aspects of daily functioning.
Many people with OCD also have other mental health disorders. About 76% of people with OCD also have a lifetime diagnosis of an anxiety disorder, about 41% have a lifetime diagnosis of major depressive disorder, and 23 to 32% have obsessive-compulsive personality disorder.
About 35 to 50% of people with OCD have suicidal thoughts at some point, and about 10 to 15% attempt suicide. Risk of a suicide attempt is increased if people also have major depressive disorder (see Suicidal Behavior).
Did You Know...
|
Diagnosis of OCD
A doctor's evaluation based on specific psychiatric diagnostic criteria
Doctors diagnose obsessive-compulsive disorder based on symptoms: the presence of obsessions, compulsions, or both. The obsessions or compulsions must be at least one of the following:
Time-consuming
Cause significant distress or interfere with the person's ability to function
Treatment of OCD
Exposure and ritual prevention therapy; cognitive therapy is often added
Certain antidepressants
Exposure and ritual (response) prevention therapy, a type of cognitive-behavioral therapy, is often effective in treating obsessive-compulsive disorder. Exposure therapy involves gradually and repeatedly exposing people to whatever situations or people triggers obsessions, rituals, or discomfort while asking them not to perform the compulsive ritual (ritual prevention therapy). Discomfort or anxiety gradually diminishes during repeated exposure as people learn that rituals are unnecessary for decreasing discomfort. The improvement usually persists for years, perhaps because people who have mastered this approach are able to continue to practice it after formal treatment has ended. Cognitive therapy is often added to exposure and ritual prevention therapy.
Selective serotonin reuptake inhibitors (such as fluoxetine), a type of antidepressant, and clomipramine, a tricyclic antidepressant, are often effective. Higher doses than are commonly used for the treatment of depression may be needed. Many experts believe that a combination of exposure and ritual prevention therapy along with medication is the best treatment, especially for more severe symptoms.(such as fluoxetine), a type of antidepressant, and clomipramine, a tricyclic antidepressant, are often effective. Higher doses than are commonly used for the treatment of depression may be needed. Many experts believe that a combination of exposure and ritual prevention therapy along with medication is the best treatment, especially for more severe symptoms.
Psychodynamic psychotherapy (which emphasizes the identification of unconscious patterns in current thoughts, feelings, and behaviors) and psychoanalysis have generally not been effective for people with obsessive-compulsive disorder.







