


Topic Resources


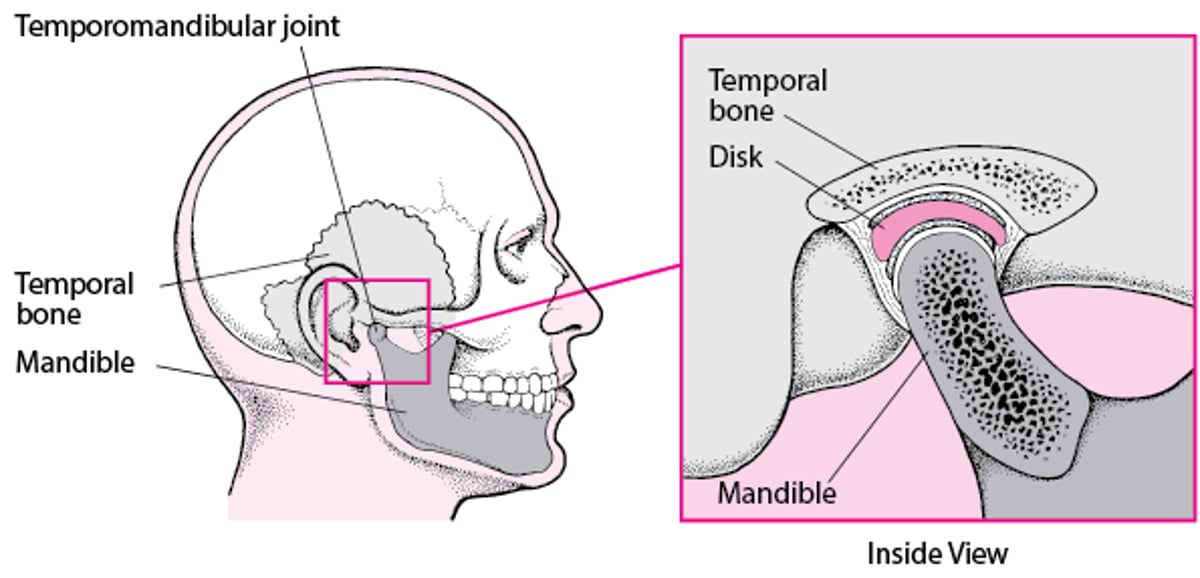
There are 2 temporomandibular joints, one on each side of the face just in front of the ears. The joints connect the temporal bones on each side of the skull with the lower jawbone (mandible). Ligaments, tendons, and muscles support the joints and are responsible for jaw movement.
Temporomandibular disorders (TMDs) are caused by problems with the jaw muscles or joints or the fibrous tissues connecting them.
People may have headaches and tenderness of the chewing muscles or may hear clicking/popping sounds of the joints in the jaw.
Doctors or dentists can usually diagnose these disorders by taking a history and doing a physical examination, but sometimes an imaging test is needed.
Treatment usually involves self-help and doctor-directed measures, oral appliance (splint) therapy, and pain relief.
The temporomandibular joint (TMJ) is one of the most complicated joints in the body: It opens and closes like a hinge and slides forward, downward, backward, and from side to side. During chewing, it may sustain an enormous amount of pressure depending on the position and health of the upper and lower teeth, which act much like a doorstop for the joint during closing. The TMJ contains a piece of dense fibrous tissue called the articular disc. The disc serves as a cushion or shock absorber between the skull and the lower jawbone, keeping them from excessively rubbing against each other.
TMDs, previously called TMJ disorders, are most common among women in their early 20s and those between the ages of 40 and 50. In rare cases, infants are born with TMJ abnormalities. TMDs include problems with the bones, joints, the muscles, and the bands of fibrous tissue that connect them (fascia).
Dislocation of the jaw, which is a dental emergency, is characterized by a wide-open mouth and pain that makes it difficult to return to a closed-mouth (teeth together) position.
Causes of Temporomandibular Disorders
Most often, the cause of a temporomandibular disorder (TMD) is a combination of muscle tension and anatomic problems within the joints. Sometimes there is a psychological component as well as other factors. Clenching and grinding of the teeth (bruxism) or repeatedly clenching or thrusting the lower jaw into an unusual position, bodywide disorders (such as osteopenia, autoimmune disorders, systemic rheumatic disorders, or genetic bone disorders), infections, injury, misalignment of teeth, and even constant gum chewing can cause symptoms. Specific causes include:
Muscle fatigue and overuse, leading to temporomandibular myofascial pain syndrome
Internal temporomandibular joint (TMJ) derangement
Arthritis
Ankylosis
Hypermobility
Abnormal jaw bone growth
Temporomandibular myofascial pain syndrome
Temporomandibular myofascial pain syndrome is the most common disorder affecting the temporomandibular region. Muscle pain and tightness around the jaw and limited mouth opening occur, as well as headache and pain in other areas of the head and neck. Pain is caused mainly by muscle fatigue or overuse, sometimes resulting from clenching or grinding the teeth while awake or asleep due to psychological or sleep-related stress. Clenching and grinding while asleep exert far more force than clenching and grinding while awake. Pain can also be brought on by injury to the head or neck, sleep disorders, problems of misalignment of the upper and lower sets of teeth, or even toothache. The TMJ can be normal. Temporomandibular myofascial pain syndrome is more common among women than men and tends to occur in younger people.
The Temporomandibular Joint

Internal temporomandibular joint derangement
In the most common form of internal TMJ derangement, the disc inside the joint lies in front of (anterior to) its normal position. The disc can be moved out of place when the ligaments that hold it in place become elongated or, often, stretched due to injury to the joint (sprained ligament).
Internal TMJ derangement can occur with or without reduction. Reduction means the parts of a joint have returned to their normal positions. Disc displacement with reduction is more common than displacement without reduction and occurs in about one-third of the adult population. In derangement with reduction, the disc lies in front of its normal position only when the mouth is closed. As the mouth opens and the jaw slides forward, the disc slips back into its normal position, often making a popping or clicking sound. As the mouth closes, the disc slips forward again. In internal TMJ derangement without reduction, the disc never slips back into its normal position, and the degree to which the mouth can be opened is limited. TMJ derangement can cause inflammation around the joint (capsulitis). Internal TMJ derangements may or may not be painful.
Arthritis
Arthritis in a temporomandibular joint may result from osteoarthritis, rheumatoid arthritis, infectious arthritis, or injury, particularly injury that causes bleeding into the joint. Such injuries are fairly common among children who are struck directly on the chin or on the side of the chin.
Osteoarthritis, a type of arthritis in which the cartilage of the body's joints degenerates, is most common among people over age 50. Osteoarthritis of the TMJ may occur when the fibrocartilage disc inside the joint is displaced or has developed holes, causing the bone of the joint to change shape as part of degenerative changes.
Rheumatoid arthritis, a disease in which the body attacks its own cells (an autoimmune disease) causing inflammation, frequently affects the temporomandibular joint. The temporomandibular joint is usually among the last joints to be affected by rheumatoid arthritis.
Infectious arthritis is caused by an infection that has spread from an adjoining area of the head or neck or that has been carried by the bloodstream to the joint from another part of the body.
Traumatic arthritis is arthritis caused by an injury (such as when the jaw is stretched widely during a difficult tooth extraction). Traumatic arthritis is rare.
Secondary degenerative arthritis is similar to traumatic arthritis but occurs because of an old injury to the jaw or those with prior joint damage due to a systemic rheumatic disease (eg, rheumatoid arthritis, juvenile idiopathic arthritis).
Ankylosis
Ankylosis is loss of joint movement resulting from a fibrosing (scarring) or fusion of bones within the joint or from calcification (the deposit of calcium into body tissues) of the ligaments around it. Ankylosis most often results from an injury or an infection, but it may be present at birth or a result of rheumatoid arthritis.
Hypermobility
Hypermobility of the jaw is looseness of the jaw that results when the ligaments that hold the joint together become excessively elongated. In hypermobility, dislocation is usually caused by the shape of the joints, ligament looseness (laxity), and muscle tension. It may be caused by trying to open the mouth too wide or by being struck on the jaw.
Symptoms of Temporomandibular Disorders
Symptoms of temporomandibular disorders (TMDs) include headaches, tenderness of the chewing muscles, and clicking or popping or locking of the joints. Sometimes the pain seems to occur near the joint rather than in it. Temporomandibular disorders may be the reason for recurring headaches that do not respond to usual medical treatment. Other symptoms include pain or stiffness in the neck and shoulders, dizziness, earaches or stuffiness in the ears, and disrupted sleep.
People with temporomandibular disorders often have difficulty opening their mouth wide. For example, most people without temporomandibular disorders can place the tips of their index, middle, and ring fingers held together and placed vertically in the space between the upper and lower front teeth without forcing the jaw to open. For people with temporomandibular disorders (with the exception of those with hypermobility), this space usually is markedly smaller.
Temporomandibular myofascial pain syndrome
People with temporomandibular myofascial pain syndrome (previously known as temporomandibular joint [TMJ] syndrome or TMJ dysfunction) may feel pain, fatigue, and tightness on the sides of the face when awakening or after stressful periods during the day. Clenching and grinding of the teeth while asleep and sleep-disordered breathing, such as obstructive sleep apnea, may cause a person to awaken with a headache, which may slowly diminish over the day. However, some people have symptoms while awake, including a headache, if they continue to clench and grind their teeth while awake. As the jaw opens, it may move slightly (deviate) to one side or the other and may not open all the way. The chewing muscles are typically painful and tender to the touch. Small spots or knots in the muscles (called trigger points) are tender and when pressed can cause referred pain in other locations in the head and neck.
Internal temporomandibular joint derangement
Internal joint derangement related to disc displacement with reduction usually causes a clicking or popping sound in the joint when the mouth opens wide or the jaw shifts from side to side. The person's jaw may also appear to move towards the affected side when they open their mouth or chew. Other people are sometimes able to hear these sounds. In many people, these joint sounds are the only symptoms. However, some people also have pain, particularly when chewing foods with a tough consistency. In a small percentage of people, these sounds progress to locking of the joints.
Internal joint derangement related to disc displacement without reduction does not cause a sound but makes it difficult for people to open their mouth wide. It usually causes pain and a feeling that the joint is out of place. Typically, this type of joint derangement starts suddenly in people whose joint previously clicked all the time (disc displacement with reduction). Sometimes people discover they are not able to fully open their jaw when they wake up. After 6 to 12 months, the pain may decrease, and the limitation on how much the mouth can be opened may resolve.
Arthritis
With osteoarthritis, because it occurs mainly when the disc is out of place or has developed holes, the person feels and often hears a grating sensation in the temporomandibular joints when opening and closing the mouth. Stiffness, mild pain, or a combination may occur. When osteoarthritis is severe, the top of the jawbone flattens out, and the person cannot open the mouth wide. The jaw may also shift toward the affected side, and the person may be unable to move it back. The person may notice a change in how the upper and lower teeth meet on the unaffected side.
Rheumatoid arthritis sometimes causes pain, swelling in the temporomandibular joint, and limited jaw movement. It usually affects both temporomandibular joints about equally, which is rarely the case in other types of TMDs. When rheumatoid arthritis is severe, especially in children, the top of the jawbone may degenerate and shorten, causing deformities of the face. This damage can lead to rapid misalignment of many or all of the upper and lower teeth. Though rare, if the damage is severe, the bones of the joint may eventually fuse together (ankylosis).
In infectious arthritis, the area over and around the temporomandibular joint is inflamed, and jaw movement is limited and painful.
Traumatic arthritis causes pain and tenderness in the temporomandibular joint, and limitation of jaw movement.
Ankylosis
Typically, fusion of the ligaments and bone around the joint (extra-articular ankylosis) is not painful, but the mouth can open only about 1 inch (about 2½ centimeters) or less. Fusion of bones within the joint (intra-articular ankylosis) causes pain and more severely limits jaw movement.
Hypermobility
In a person with hypermobility, the jaw may slip forward completely out of its socket (dislocate), causing pain and an inability to close the mouth. Dislocation may occur suddenly and repeatedly.
Abnormal jaw bone growth
Sometimes a portion of the jaw bone called the mandibular condyle can grow too much (hyperplasia) or too little (hypoplasia) on one side more than the other. This causes the jaw bone to grow unevenly and to be misaligned.
Diagnosis of Temporomandibular Disorders
A dentist's or doctor's evaluation
Sometimes imaging tests
For infectious arthritis, aspiration of fluid
Sometimes polysomnography (sleep study)
A dentist or doctor almost always diagnoses a temporomandibular disorder based solely on a person's medical and dental history and on a physical examination. Part of the examination involves gently pressing on the side of the face or placing the little finger in the person's ear and gently pressing forward while the person opens and closes the jaw, and listening with a stethoscope and feeling for sounds of catching, clicking, or popping. Also the doctor gently presses on the chewing muscles to detect pain or tenderness and notes whether the jaw slides when the person bites. The person is asked to open the mouth as wide as is comfortable. An average-sized person can open the mouth at least 1½ inches (about 4 centimeters).
When a doctor suspects an internal joint derangement, further tests can be done. Magnetic resonance imaging (MRI) is a test that can help doctors assess whether internal joint derangement has occurred or why a person is not responding to treatment.
A doctor suspects osteoarthritis when a creaking/grating sound is heard when the person opens the mouth (crepitus). X-rays and/or a computed tomography (CT) scan can confirm the diagnosis.
Infectious arthritis may be suspected when the area over and around the temporomandibular joint is inflamed and when movement of the joint is painful and limited. Infection in another part of the body serves as a clue as well. To confirm the diagnosis of infectious arthritis, the doctor may insert a needle into the temporomandibular joint and withdraw fluid (aspiration), which is then analyzed for bacteria.
If hypermobility is the cause, the person typically can open the mouth wider than the breadth of 3 fingers. The jaw may be chronically dislocated. If ankylosis is the cause, the jaw's range of motion tends to be markedly reduced.
If symptoms of muscle pain and tightness continue, doctors may arrange testing for a sleep disorder. This test is called polysomnography.
Treatment of Temporomandibular Disorders
Oral appliance (mouth guard) therapy and pain relievers
Self-help measures
Sometimes physical therapy
Sometimes surgery
Sometimes other medications (such as muscle relaxants, sleep aids, or botulinum toxin)
Treatment varies considerably according to the cause. Two common treatments are oral appliance therapy (also called splint therapy or a mouth guard) and analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs) to relieve pain.
Temporomandibular myofascial pain syndrome
Oral appliance
An oral appliance often is the main treatment for jaw muscle pain and tightness. For people who realize that they clench or grind their teeth, oral appliance therapy can help them break the habit. A thin plastic oral appliance is made by a dentist to fit over either the upper or the lower set of teeth and is adjusted to give the person an even bite. The oral appliance, usually worn while sleeping (a mouth guard), often reduces grinding and clenching, allowing the jaw muscles to rest and recover. For pain while awake, an oral appliance allows the jaw muscles to remain relaxed and the bite to be stable, thereby reducing discomfort. The oral appliance can also prevent damage to teeth that are under exceptional stress from the grinding and clenching. Oral appliances are used while awake only until symptoms subside, usually less than 8 weeks. Longer use may be warranted depending on the severity of symptoms.
Self-help measures
People should use self-help measures to relieve pain and restore normal function.
Switching to a diet of softer foods, cutting food into smaller pieces, chewing slowly, and not opening the mouth as wide will decrease muscle tension and stress on the temporomandibular joints.
Keeping the upper and lower teeth apart while awake will help break the habit of clenching or grinding the teeth, also decreasing muscle tension and stress on the temporomandibular joints.
Developing some system to help remember to correct poor posture will help the jaw and neck/shoulder muscles recover.
Following proper sleep behavior, including going to sleep at the same time in a quiet and comfortable environment, will decrease pain and allow the body to heal.
Applying moist heat to fatigued muscles will also help.
Physical therapy
Physical therapy may also be prescribed. Physical therapy may involve ultrasound treatment (in which sound waves are used to provide heat and tissue stimulation to promote healing), electromyographic biofeedback (in which the person learns to relax the muscles), spray and stretch exercises (in which the jaw is stretched open after the skin over the painful area has been sprayed with a skin refrigerant or numbed with ice). Transcutaneous electrical nerve stimulation (TENS—see sidebar Physical Therapy for Jaw Muscles) also may help. Stress management, sometimes along with electromyographic biofeedback, and counseling helps some people.
Medications
Medications may also be helpful. For instance, muscle-relaxers, such as cyclobenzaprine, may be prescribed to ease tightness and pain. A benzodiazepine (antianxiety medication that also relaxes muscles) can sometimes be taken temporarily at bedtime to help relieve symptoms. However, these medications are not a cure, generally are not recommended for older adults, and are prescribed for only a short time, usually for a month or less. Medications may also be helpful. For instance, muscle-relaxers, such as cyclobenzaprine, may be prescribed to ease tightness and pain. A benzodiazepine (antianxiety medication that also relaxes muscles) can sometimes be taken temporarily at bedtime to help relieve symptoms. However, these medications are not a cure, generally are not recommended for older adults, and are prescribed for only a short time, usually for a month or less.
Analgesics such as acetaminophen or other NSAIDs also may help relieve pain. A prescription for opioid analgesics is usually not given because treatment may be needed for some time and these medications can be addictive. Sleep aids (sedatives) may be used occasionally and for a short time to help people who have trouble sleeping because of the pain. People who may have a sleep disorder, such as Analgesics such as acetaminophen or other NSAIDs also may help relieve pain. A prescription for opioid analgesics is usually not given because treatment may be needed for some time and these medications can be addictive. Sleep aids (sedatives) may be used occasionally and for a short time to help people who have trouble sleeping because of the pain. People who may have a sleep disorder, such asobstructive sleep apnea, should ask their doctor before using any benzodiazepines or sedatives (including over-the-counter sleep aids) or muscle-relaxing medications because these medications can worsen that disorder.
Botulinum toxin injected into the muscle or anesthetics injected into muscular trigger points have been used to relieve muscle spasms and pain.
In some cases of chronic pain, antidepressant medications may be useful.
Regardless of the type of treatment, most people experience significant relief within about 3 months. If the symptoms are not severe, many people recover without treatment.
Internal temporomandibular joint derangement
In internal joint derangement with or without reduction, treatment is needed only if a person has jaw pain or trouble moving the jaw. People are often given NSAIDs for pain. If a person seeks treatment right after symptoms develop, a dentist or doctor may be able to manually move the disc back into its normal position.
If a person has had the disorder for fewer than 3 to 6 months, an oral anterior repositioning appliance may be used. The appliance holds the lower jaw forward, keeps the disc in position, and permits the supporting ligaments to tighten and become pain free. Over 2 to 4 months, the oral appliance is adjusted to allow the jaw to return back to its normal position, with the expectation that the disc will remain in place. However, the longer the disc is displaced, the less likely its repositioning will succeed.
A person with internal joint derangement with or without reduction should avoid opening the mouth wide—for instance, when yawning or biting into a thick sandwich—because injured joints are not as protected in these activities as they would be in a normal jaw. People with this disorder are advised to cut food into small pieces and to eat food that is easy to chew.
Sometimes the slipped disc becomes stuck in front of the temporomandibular joint (TMJ), preventing the jaw from opening fully. The disc must then be manually moved even further out of position to allow the joint to move fully. Passive jaw-motion devices, which stretch the jaw, have been used to slowly increase jaw motion. These devices are used several times a day. One such device is a threaded screw-type instrument that is placed between the front teeth and turned, much like a car jack, to gradually and gently push the disc forward, thereby creating a wider mouth opening. If such a device is not available, then a doctor may use a stack of tongue depressors placed between the front teeth, with an additional tongue depressor being added to the middle of the stack to increase mouth opening little by little.
If internal joint derangement cannot be treated by nonsurgical means, an oral and maxillofacial surgeon may need to do surgical procedures. However, the need for traditional surgery is rare since the introduction of procedures such as arthroscopy. All surgical procedures are used in combination with oral appliance therapy, self-help measures, and supervision by a dentist or doctor.
Arthritis
A person with osteoarthritis in a temporomandibular joint needs to rest the jaw as much as possible, use an oral appliance or other device to control muscle tightness, and take an analgesic (such as acetaminophen or an NSAID) for pain. The pain usually goes away in 6 months with or without treatment. Even without treatment, most of the symptoms subside, probably because the band of tissue behind the disc becomes scarred and functions like the original disc. Usually, jaw movement is sufficient for normal activities, though the jaw may not open as wide as it used to. The oral appliance is usually worn while asleep, but it is sometimes also worn while awake.in a temporomandibular joint needs to rest the jaw as much as possible, use an oral appliance or other device to control muscle tightness, and take an analgesic (such as acetaminophen or an NSAID) for pain. The pain usually goes away in 6 months with or without treatment. Even without treatment, most of the symptoms subside, probably because the band of tissue behind the disc becomes scarred and functions like the original disc. Usually, jaw movement is sufficient for normal activities, though the jaw may not open as wide as it used to. The oral appliance is usually worn while asleep, but it is sometimes also worn while awake.
Rheumatoid arthritis of the temporomandibular joint is treated with the medications used for rheumatoid arthritis of any joint. NSAIDs may be given for severe pain. Maintaining joint mobility and preventing fusion of the joint are particularly important. Usually, the best way to accomplish these goals is by exercising the jaw under a physical therapist's direction. To relieve symptoms, particularly muscle tightness, the person wears an oral appliance during sleep. If joint fusion prevents all movement of the jaw, the person may need surgery and, in rare cases, an artificial joint to restore jaw mobility.
Infectious arthritis is treated with antibiotics, proper hydration, pain control, and restriction of movement. Penicillin is usually the antibiotic used initially, until test results determine the type of bacteria present and thus the best antibiotic to use. Pus in the joint, if present, may be removed with a needle. Once the infection is controlled, people do jaw-opening exercises to help prevent scarring and limitation of motion.
Traumatic arthritis is treated with NSAIDs and sometimes steroids (also referred to as glucocorticoids or corticosteroids). Steroids are medications that may reduce inflammation and ease symptoms such as swelling, redness, and pain. Treatment also includes application of heat, a soft diet, and restriction of jaw movement.
Ankylosis
Occasionally, jaw-opening exercises can help, but people with bone fusion usually need surgery to restore jaw movement, and exercises are then needed for months to years to maintain the surgical correction.
Hypermobility
Prevention and treatment of dislocation resulting from hypermobility are the same as those for other causes of a dislocated jaw. When dislocation occurs, help is sometimes needed to snap the jaw back into position. Many people who experience repeated dislocations, however, learn how to maneuver the joint back into place themselves by consciously relaxing the muscles and lightly shifting the lower jaw until it pops back into place. To prevent recurrent dislocations, doctors may inject a substance into the joint (for example, blood) that causes scarring and thereby reduces mobility. Surgery to reshape the bone or tighten the ligaments around the temporomandibular joint is sometimes necessary to prevent recurrent dislocations.
Abnormal jaw bone growth
Surgery is usually required to lengthen or shorten one side of the jaw bone to even out the jaw bone. This helps correct the alignment of the jaw.
Drugs Mentioned In This Article



