


Atrial fibrillation is a rapid, irregularly irregular atrial rhythm. Symptoms include palpitations and sometimes weakness, effort intolerance, dyspnea, and presyncope. Atrial thrombi may form, causing a significant risk of embolic stroke. Diagnosis is by electrocardiography. Treatment involves rate control with medications, prevention of thromboembolism with anticoagulation, and sometimes conversion to sinus rhythm by medications or cardioversion.
(See also Overview of Arrhythmias.)
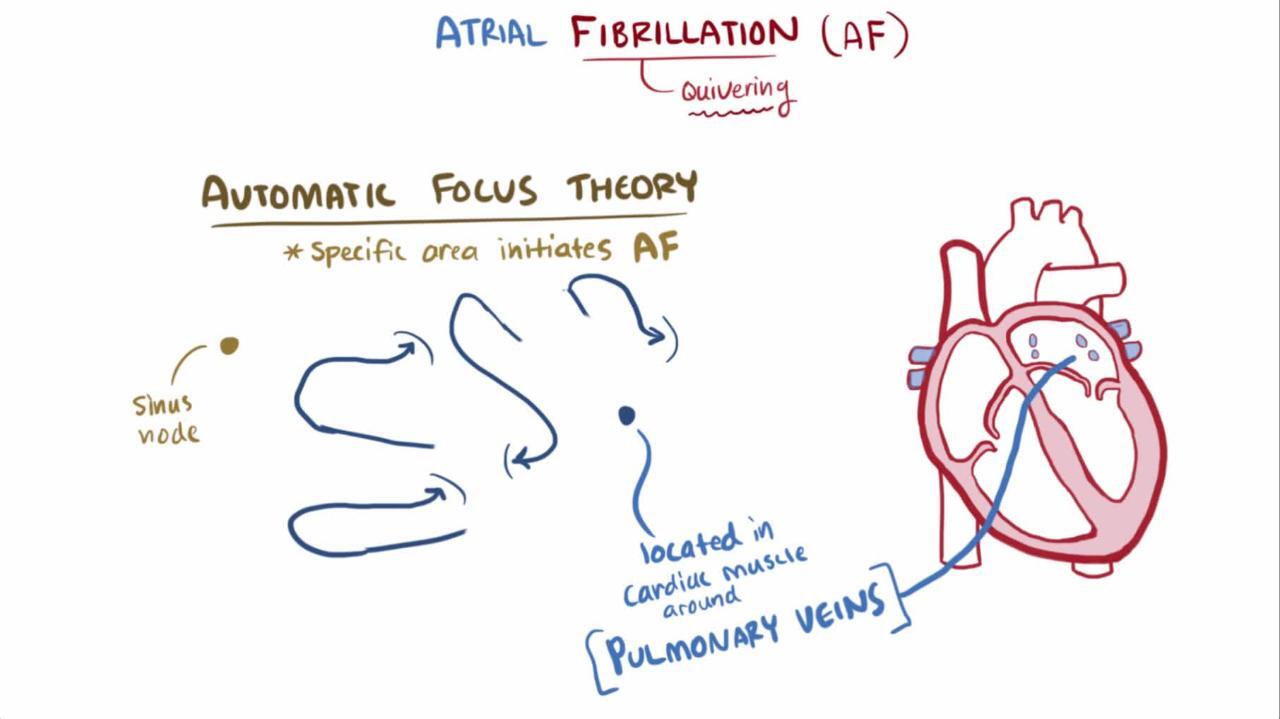
Atrial fibrillation is initiated and maintained by multiple electrophysiologic and structural mechanisms. Early in its course the dominant mechanisms are focal automaticity and micro-reentry (drivers) predominantly originating from muscular sleeves in venous structures adjacent to the atria, especially the pulmonary veins. Atrial electrical remodeling then encourages functional reentrant circuits, including leading circle reentry and rotors (spatiotemporal organization of activation wavefronts as rapid, localized reentrant spiral waves with centrifugal spread). Finally, atrial structural remodelling, including atrial fibrosis, permits structural reentry (reentrant activation wavefronts circling an anatomical barrier such as scar), which, in addition to the other phenomena, produces multiple atrial wavelets of disorganized activations. In atrial fibrillation, the atria do not contract, and the atrioventricular (AV) conduction system is bombarded with many electrical stimuli, causing inconsistent impulse transmission and an irregularly irregular ventricular rate, which is usually in the tachycardia rate range.
Atrial fibrillation is one of the most common arrhythmias, affecting between 3 and 6 million adults in the United States (1). Males and White people are more likely to have atrial fibrillation than females and Black people. The lifetime risk of developing atrial fibrillation is approximately 25% in males and 20% in females. Prevalence increases with age; < 1% at age 50 years, 1 to 4% at age 65 years, and 6 to 15% at age 80 years (2). Atrial fibrillation tends to occur in patients with an underlying heart disorder.
Complications of atrial fibrillation
The absent atrial contractions predispose to thrombus formation; the overall annual risk of cerebrovascular embolic events is 3 to 5%, and atrial fibrillation is responsible for approximately 20 to 25% of all strokes (2). Risk of stroke is higher in older patients and in patients with moderate to severe mitral stenosis, mechanical heart valve, hyperthyroidism, hypertension, diabetes, left ventricular systolic dysfunction, or previous thromboembolic events. These factors are considered in scoring systems that predict the risk of future thromboembolic events such as the CHA(2)DS(2)-VASc score, which is widely used in patients without moderate or severe mitral stenosis or a mechanical heart valve (who need anticoagulation regardless of their CHA(2)DS(2)-VASc score). Systemic emboli can also cause malfunction or necrosis of other organs (eg, heart, kidneys, gastrointestinal tract, eyes) or a limb.
Atrial fibrillation also may impair cardiac output; loss of atrial contraction can lower cardiac output at normal heart rate by as much as 20% (3). Such a decrease is usually well tolerated except when the ventricular rate becomes too fast (eg, > 140 beats/minute), or when patients have borderline or low cardiac output to begin with. In such cases, heart failure may develop.

General references
1. Go AS, Hylek EM, Phillips KA, et al: Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 285(18):2370–2375, 2001. doi: 10.1001/jama.285.18.2370.
2. Andrade J, Khairy P, Dobrev D, et al: The clinical profile and pathophysiology of atrial fibrillation: relationships among clinical features, epidemiology, and mechanisms. Circ Res 114(9):1453–1468, 2014. doi: 10.1161/CIRCRESAHA.114.303211.
3. Klavebäck S, Skúladóttir H, Olbers J, et al: Changes in cardiac output, rhythm regularity, and symptom severity after electrical cardioversion of atrial fibrillation. Scand Cardiovasc J 57(1):2236341, 2023. doi: 10.1080/14017431.2023.2236341
Etiology of Atrial Fibrillation
The most common causes of atrial fibrillation are
Valvular heart disorders: mitral stenosis, mitral regurgitation, tricuspid regurgitation
Binge alcohol drinking (holiday heart)
Less common causes of atrial fibrillation include
Atrial septal defects and other congenital heart defects
Lone atrial fibrillation is atrial fibrillation without an identifiable cause in patients < 60 years.
Classification of Atrial Fibrillation
Paroxysmal atrial fibrillation is atrial fibrillation that lasts < 1 week having converted spontaneously or by an intervention to normal sinus rhythm. Episodes may recur (1).
Persistent atrial fibrillation is continuous atrial fibrillation that lasts > 1 week (1).
Long-standing persistent atrial fibrillation lasts > 1 year, but there is still the possibility of restoring sinus rhythm (1).
Permanent atrial fibrillation cannot be converted to sinus rhythm (the term also includes patients for whom a decision has been made not to attempt conversion to sinus rhythm [1]). The longer atrial fibrillation is present, the less likely is spontaneous conversion and the more difficult is cardioversion because of atrial remodeling (rapid atrial rate-induced changes in atrial electrophysiology, including a decrease in atrial refractoriness, spatial dispersion of atrial refractoriness, slowed atrial conduction velocity, or combinations of these) (2).
Classification references
1. Joglar JA, Chung MK, Armbruster AL, et al: 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1):e1–e156, 2024. doi: 10.1161/CIR.0000000000001193
2. Allessie M, Ausma J, Schotten U: Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovasc Res54(2):230–246, 2002. doi: 10.1016/s0008-6363(02)00258-4
Symptoms and Signs of Atrial Fibrillation
Atrial fibrillation is often asymptomatic, but many patients have palpitations, chest discomfort, or symptoms of heart failure (eg, weakness, light-headedness, dyspnea), particularly when the ventricular rate is very rapid (often 140 to 160 beats/minute). Patients may also present with symptoms and signs of acute stroke or of other organ damage due to systemic emboli.
The pulse is irregularly irregular with loss of a waves in the jugular venous pulse. A pulse deficit (the apical ventricular rate is faster than the rate palpated at the wrist) may be present because left ventricular stroke volume is not always sufficient to produce a peripheral pressure wave for a beat closely coupled to the previous beat.
Diagnosis of Atrial Fibrillation
Electrocardiography (ECG)
Echocardiography
Thyroid function tests
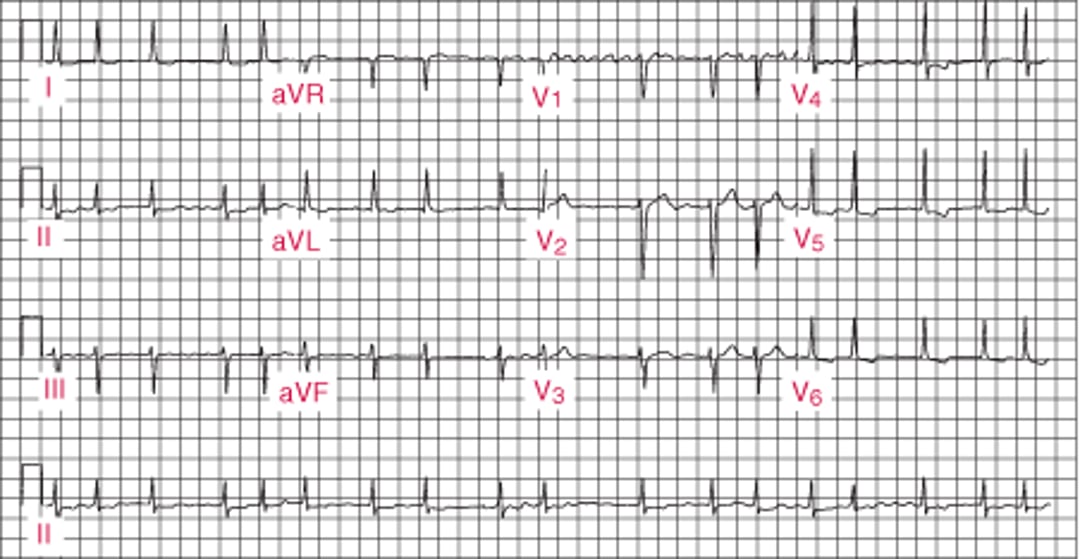
Diagnosis of atrial fibrillation is by ECG (see figure Atrial Fibrillation). Findings include
Absence of P waves
Presence of f (fibrillatory) waves between QRS complexes; f waves are irregular in timing and irregular in morphology; baseline undulations at rates > 300 beats/minute, usually best seen in lead V1 and not always apparent in all leads
Irregularly irregular R-R intervals
Atrial Fibrillation

Other irregular rhythms may resemble atrial fibrillation on ECG but can be distinguished by the presence of discrete P or flutter waves, which can sometimes be made more visible with vagal maneuvers. Muscle tremor or electrical interference may resemble f waves, but the underlying ventricular rhythm is regular.
Atrial fibrillation may also cause a phenomenon that mimics ventricular extrasystoles or ventricular tachycardia (Ashman phenomenon). This phenomenon typically occurs when a short R-R interval follows a long R-R interval; the longer interval lengthens the refractory period of the infra-Hisian conduction system, and the subsequent short R-R QRS complex(es) are conducted aberrantly, typically with right bundle branch morphology (1).
Echocardiography and thyroid function tests are important in the initial evaluation (2).
Echocardiography is done to assess structural heart defects (eg, left atrial enlargement, left ventricular wall motion abnormalities suggesting past or present ischemia, valvular disorders, cardiomyopathy) and to identify additional risk factors for stroke (eg, atrial blood stasis or thrombus, complex aortic plaque). Atrial thrombi are more likely in the atrial appendages, where they are best detected by transesophageal rather than transthoracic echocardiography.
Pearls & Pitfalls
|
Diagnosis references
1. Morton MB, Morton JB, Mond HG: Aberrant Ventricular Conduction: Revisiting an Old Concept. Heart Lung Circ 32(5):555–566, 2023. doi: 10.1016/j.hlc.2023.03.001
2. Joglar JA, Chung MK, Armbruster AL, et al: 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation149(1):e1–e156, 2024. doi: 10.1161/CIR.0000000000001193
Treatment of Atrial Fibrillation
Rate control with medications or AV node ablation
Sometimes rhythm control with synchronized cardioversion, medications, or atrial fibrillation substrate ablation
Prevention of thromboembolism
Patients with hemodynamically unstable atrial fibrillation may benefit from hospitalization. Patients with recurrent episodes do not require hospitalization unless other symptoms suggest the need for it. Once causes have been managed, treatment of atrial fibrillation focuses on ventricular rate control, rhythm control, and prevention of thromboembolism.
Ventricular rate control
Patients with atrial fibrillation of any duration require rate control (typically to < 100 beats/minute at rest) to control symptoms and prevent tachycardia-induced cardiomyopathy (1).
For acute paroxysms of rapid rate (eg, 140 to 160 beats/minute), IV AV node blockers are used (for doses, see table Antiarrhythmic Medications). CAUTION: AV node blockers should not be used in patients with Wolff-Parkinson-White syndrome when an accessory AV pathway is involved (indicated by wide QRS duration); these medications may increase frequency of conduction via the bypass tract, possibly causing ventricular fibrillation (1).
1).
heart failure is present. These medications may be used orally for long-term rate control (1).
1). Amiodarone may also convert the atrial fibrillation to sinus rhythm; however, this conversion may not be desirable in some patients who are not receiving an anticoagulant (see Prevention of thromboembolism).
Rhythm control
In patients with heart failure or other hemodynamic compromise directly attributable to new-onset atrial fibrillation, restoration of normal sinus rhythm is indicated to improve cardiac output (1). In other cases, conversion of atrial fibrillation to normal sinus rhythm is optimal, but the antiarrhythmic medications that are capable of doing so (class Ia, Ic, III) have a risk of adverse effects and may increase mortality. Conversion to sinus rhythm does not eliminate the need for chronic anticoagulation.
For acute conversion, synchronized cardioversion or medications can be used.
Before conversion is attempted, the ventricular rate should be controlled to < 120 beats/minute, and most patients should be anticoagulated (for criteria and methods, see Prevention of thromboembolism) because conversion of atrial fibrillation, regardless of the method used, transiently increases the risk of thromboembolism.
Synchronized cardioversion (200 joules biphasic, followed by 300 and 360 joules biphasic as needed) converts atrial fibrillation to normal sinus rhythm in approximately 90% of patients, although recurrence rate is high (2). Efficacy and maintenance of sinus rhythm after the procedure is improved with use of class Ia, Ic, or III antiarrhythmic medications during the 24 to 48 hours before the procedure. Cardioversion is more effective in patients with shorter duration of atrial fibrillation, lone atrial fibrillation, or atrial fibrillation with a reversible cause; it is less effective when the left atrium is enlarged (> 5 cm) or if a significant underlying structural heart disorder is present.
Medications for conversion of atrial fibrillation to sinus rhythmAntiarrhythmic Medications). A meta-analysis reported 4-hour, medication-specific cardioversion rates ranging from approximately 25% to 65%; the most effective agents were IV vernakalant, IV flecainide, IV propafenone, oral flecainide, and IV ibutilide (3). Excepting amiodarone and sotalol, which also slow ventricular response rate to atrial fibrillation, these medications should not be used until the rate has been controlled.
≥≥ 70 kg, otherwise 450 mg) that patients carry and self-administer when palpitations develop (“pill-in-the-pocket” approach) (5). This approach must be limited to patients who have no sinoatrial or AV node dysfunction, bundle branch block, QT prolongation, Brugada syndrome, or structural heart disease. Its major hazard (estimated at 1%) is the possibility of converting atrial fibrillation to a slowish atrial flutter that conducts 1:1 in the 200 to 240 beat/minute range (5). This potential complication can be reduced in frequency by coadministration of an AV nodal–suppressing medication (eg, a beta-blocker or a nondihydropyridine calcium antagonist).
Angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), and aldosterone blockers may attenuate the myocardial fibrosis that provides a substrate for atrial fibrillation, but the role of these medications in routine atrial fibrillation treatment has yet to be defined.
Ablation procedures for atrial fibrillation
For patients who are not candidates for rate control or rhythm control or in whom these approaches fail, ablation of the AV node may be done to cause complete heart block; insertion of a permanent pacemaker is then necessary. Ablation of the slow AV nodal pathway (AV node modification) reduces the number of atrial impulses reaching the ventricles and eliminates the need for a pacemaker, but this approach is considered less effective than complete ablation and is rarely used.
Catheter ablation procedures that accomplish electrical isolation of the pulmonary veins from the left atrium can prevent atrial fibrillation without causing AV block. Pulmonary vein isolation has a lower success rate (60 to 80%) and a higher major complication rate (1 to 5%) than ablation procedures used to treat supraventricular arrhythmias (6). Randomized trials in patients who have not had antiarrhythmic medications have shown a lower recurrence rate for atrial tachyarrhythmias with ablation (approximately 30%) than with pharmacotherapy (approximately 50%) after 17 months of follow up and no significant difference in major adverse events (7). Furthermore, meta-analysis suggests that, compared to medical therapy, catheter ablation reduces all-cause mortality, most evident in patients with coexisting heart failure, and reduces hospitalizations in patients with paroxysmal atrial fibrillation and in those with persistent atrial fibrillation with or without heart failure (8). Accordingly, guidelines give catheter ablation for rhythm control a class I indication in patients with atrial fibrillation in whom a rhythm control approach with antiarrhythmic medication has failed, in patients with coexisting heart failure with reduced ejection fraction, and in selected patients as first-line therapy early in the course of atrial fibrillation (1).
There is also an open heart surgical ablation procedure for atrial fibrillation treatment (the maze procedure), but it is mostly reserved for patients with another indication for open heart surgery rather than used as a stand-alone procedure (9).
Randomized clinical trials addressing the need for continued long-term oral anticoagulation after an apparently successful ablation procedure are underway. Guidelines recommend long-term anticoagulation after ablation using the same guidelines as for patients who have not had an ablation regardless of the apparent success of the procedure (1).
Prevention of thromboembolism
Long-term measures to prevent thromboembolism are taken for certain patients with atrial fibrillation depending on their estimated risk of stroke versus risk of bleeding (eg, as per the CHA(2)DS(2)-VASc score [8] and the HAS-BLED tool [10]).
CHA(2)DS(2)-VASc Score
Variable | Points |
|---|---|
History of congestive heart failure | 1 |
History of hypertension | 1 |
Age ≥ 75 years | 2 |
History of diabetes mellitus | 1 |
Prior stroke/transient ischemic attack (TIA) | 2 |
Vascular disease | 1 |
Age 65–74 years | 1 |
Sex (female) | 1 |
The guidelines for antithrombotic therapy in atrial fibrillation differ in different regions. The guidelines in the United States are as follows (1).
Long-term oral anticoagulant therapy is recommended for patients with atrial fibrillation with the following (class I recommendation):
Moderate to severe rheumatic mitral stenosis
Mechanical artificial heart valve (with or without atrial fibrillation)
Nonvalvular atrial fibrillation (ie, absent moderate to severe rheumatic mitral stenosis or mechanical heart valve) with CHA(2)DS(2)-VASc scores of ≥ 2 in males and ≥ 3 in females
Hypertrophic cardiomyopathy
The annual risk of thromboembolism for these patients is ≥ 2%.
Long-term oral anticoagulant therapy is reasonable for (class IIa recommendation):
Patients with nonvalvular atrial fibrillation and CHA(2)DS(2)-VASc scores of 1 in males and 2 in females
The annual risk of thromboembolism for these patients is between 1 and 2%.
Long-term oral anticoagulant therapy is not recommended for patients with:
Nonvalvular atrial fibrillation and CHA(2)DS(2)-VASc scores of 0 in males and 1 in females
The annual risk of thromboembolism for these patients is < 1%.
The following recommendations apply to the means of anticoagulation:
Patients with atrial fibrillation and moderate to severe rheumatic mitral stenosis
These general guidelines are altered in patients with more than moderate renal impairment with decreasing enthusiasm for anticoagulation as renal impairment progresses from chronic kidney disease stages 1, 2, and 3 (eGFR > 30 mL/minute [class I recommendation]), through chronic kidney disease stage 4 (eGFR 15 to 30 mL/minute [class IIa recommendation]), to chronic kidney disease stage 5 (eGFR < 15 mL/minute or on dialysis [class IIb recommendation]).
Because 90% of left atrial thrombi in patients with nonvalvular atrial fibrillation are located in the left atrial appendage, stroke prevention in such patients may be accomplished by surgical ligation of the left atrial appendage or by occlusion with a transcatheter device. Guidelines give a class IIa indication for left atrial appendage closure in patients with atrial fibrillation and a CHA(2)DS(2)-VASc score of ≥ 2 when appropriate antithrombotic therapy is contraindicated and a class IIb indication in such patients based on patient preference (1).
An individual patient's risk of bleeding may be estimated with any of a number of prognostic tools, of which the most commonly used is HAS-BLED (11) (see table HAS-BLED Tool for Predicting Risk of Bleeding in Patients With Atrial Fibrillation). The HAS-BLED score serves best in identifying conditions that, if modified, reduce bleeding risk rather than in identifying patients with a higher risk of bleeding who should not receive anticoagulation.
HAS-BLED Tool for Predicting Risk of Bleeding in Patients With Atrial Fibrillation
Variable | Points |
|---|---|
Uncontrolled hypertension | 1 |
Abnormal kidney function | 1 |
Abnormal liver function | 1 |
Prior stroke | 1 |
Prior bleeding | 1 |
1 | |
Older age (> 65 years) | 1 |
Medication use (defined as concomitant use of a nonsteroidal anti-inflammatory drug [NSAID] or an antiplatelet medication) | 1 |
Alcohol use (defined as > 8 alcohol units per week) | 1 |
Prevention of thromboembolism in patients undergoing cardioversion
Guidelines suggest the following measures for prevention around the time of cardioversion (1):
Anticoagulation in Patients Ungergoing Cardioversion
* Anticoagulant can be given for < 3 weeks if TEE does not show atrial thrombus. TEE = tranesophageal echocardiography (to rule out left atrial thrombus). |


If atrial fibrillation has been present > 48 hours, patients should typically be given an oral anticoagulant for > 3 weeks before medical or DC conversion. If immediate cardioversion is desirable, transesophageal echocardiography (TEE) is recommended to exclude atrial thrombus prior to cardioversion. Anticoagulation can be given for a shorter time before conversion if TEE does not show left atrial thrombus. Anticoagulation should be continued for at least 4 weeks after cardioversion (each is a class I recommendation).
If atrial fibrillation has been present < 48 hours in patients with a CHA(2)DS(2)-VASc score of ≥ 2 and therapeutic anticoagulation for > 3 weeks has not been done, TEE should be done to rule out left atrial thrombus before cardioversion (class IIb recommendation).
If atrial fibrillation has been present < 12 hours and patients have a CHA(2)DS(2)-VASc score of 0 to 1 (see table CHA(2)DS(2)-VASc score), the benefit of precardioversion TEE and of pericardioversion anticoagulation is uncertain (implying, without so stating, that the latter group of patients may undergo cardioversion without a precardioversion TEE or precardioversion anticoagulation.
Pearls & Pitfalls
|
Treatment references
1. Joglar JA, Chung MK, Armbruster AL, et al: 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1):e1–e156, 2024. doi: 10.1161/CIR.0000000000001193
2. Crijns HJ, Weijs B, Fairley AM, et al: Contemporary real life cardioversion of atrial fibrillation: Results from the multinational RHYTHM-AF study. Int J Cardiol 172(3):588–594, 2014. doi:10.1016/j.ijcard.2014.01.099
3. Tsiachris D, Doundoulakis I, Pagkalidou E, et al: Pharmacologic Cardioversion in Patients with Paroxysmal Atrial Fibrillation: A Network Meta-Analysis. Cardiovasc Drugs Ther 35(2):293–308, 2021. doi: 10.1007/s10557-020-07127-1
4. Valembois L, Audureau E, Takeda A, et al: Antiarrhythmics for maintaining sinus rhythm after cardioversion of atrial fibrillation. Cochrane Database Syst Rev 9(9):CD005049, 2019. doi: 10.1002/14651858.CD005049.pub5
5. Ibrahim OA, Belley-Côté EP, Um KJ, et al: Single-dose oral anti-arrhythmic drugs for cardioversion of recent-onset atrial fibrillation: a systematic review and network meta-analysis of randomized controlled trials. Europace 23(8):1200–1210, 2021. doi: 10.1093/europace/euab014
6. Voskoboinik A, Moskovitch JT, Harel N, Sanders P, Kistler PM, Kalman JM: Revisiting pulmonary vein isolation alone for persistent atrial fibrillation: A systematic review and meta-analysis. Heart Rhythm 14(5):661–667, 2017. doi:10.1016/j.hrthm.2017.01.003
7. Razzack AA, Lak HM, Pothuru S, et al: Efficacy and Safety of Catheter Ablation vs Antiarrhythmic Drugs as Initial Therapy for Management of Symptomatic Paroxysmal Atrial Fibrillation: A Meta-Analysis. Rev Cardiovasc Med 23(3):112, 2022. doi: 10.31083/j.rcm2303112
8. Ravi V, Poudyal A, Lin L, et al: Mortality benefit of catheter ablation versus medical therapy in atrial fibrillation: An RCT only meta-analysis. J Cardiovasc Electrophysiol 33(2):178–193, 2022. doi: 10.1111/jce.15330
9. Guo Q, Yan F, Ouyang P, et al: Bi-atrial or left atrial ablation of atrial fibrillation during concomitant cardiac surgery: A Bayesian network meta-analysis of randomized controlled trials. J Cardiovasc Electrophysiol 32(8):2316–2328, 2021. doi:10.1111/jce.15127
10. Lip GY, Nieuwlaat R, Pisters R, et al: Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Hart Survey on atrial fibrillation. Chest 137(2):263–272, 2010. doi: 10.1378/chest.09-1584
11. Pisters R, Lane DA, Nieuwlaat R, et al: A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest 138(5):1093–1100, 2010. doi: 10.1378/chest.10-0134
Key Points
Atrial fibrillation is an irregularly irregular atrial rhythm that may be episodic or continuous.
QRS complexes are typically narrow; a wide complex may occur with intraventricular conduction defects or Wolff-Parkinson-White syndrome.
Patients should have electrocardiography, echocardiography, and thyroid function testing.
Heart rate is controlled typically to <
Restoration of sinus rhythm does not eliminate the need for anticoagulation but may help patients with continuing symptoms or hemodynamic compromise (eg, heart failure); synchronized cardioversion or medication can be used.
Long-term oral anticoagulation to prevent stroke is required for patients with risk factors for thromboembolism.
Anticoagulation is usually necessary before cardioversion.







