



")

Despite the use of cardiopulmonary resuscitation (CPR), mortality rates for out-of-hospital cardiac arrest are approximately 90% for infants and children (1). Mortality rates for in-hospital cardiac arrest for infants and children are approximately 65%. The mortality rate is 20 to 25% for respiratory arrest alone. Neurologic outcome is often severely compromised.
Pediatric resuscitation protocols are different for infants and children. Infant guidelines apply to those < 1 year of age, and child protocols are used from age 1 year up to a weight of 55 kg or the presence of signs of puberty (defined as appearance of breasts in females and axillary hair in males). Adult resuscitation protocols apply to children past the age of puberty or children weighing > 55 kg. Approximately 50 to 65% of children requiring CPR are < 1 year; of these, most are < 6 months.
Neonatal resuscitation used in the immediate perinatal period is discussed elsewhere. Approximately 6% of neonates require resuscitation at delivery; the incidence increases significantly if birth weight is < 1500 g.
The Pediatric Cerebral Performance Category Scale is used to categorize neurologic outcome after cardiac arrest.
Pediatric Cerebral Performance Category Scale*
Score | Category | Description |
|---|---|---|
1 | Normal | Age-appropriate level of functioning In preschool-aged children, appropriate development In school-aged children, attendance in regular classes |
2 | Mild disability | Can interact at an age-appropriate level Minor neurologic disease that is controlled and does not interfere with daily functioning (eg, seizure disorder) In preschool-aged children, possibly minor developmental delays, but with > 75% of all daily living developmental milestones above the 10th percentile In school-aged children, attendance in regular school but may be in a grade that is not appropriate for age |
3 | Moderate disability | Below age-appropriate functioning Neurologic disease that is not controlled and severely limits activities In preschool-aged children, most daily living developmental milestones below the 10th percentile In school-aged children, can do ADLs but attend special classes because of cognitive difficulties or a learning deficit |
4 | Severe disability | In preschool-aged children, ADL milestones below the 10th percentile and excessive dependence on others for ADLs In school-aged children, possibly severe impairment that prevents school attendance and dependence on others for ADLs In preschool-aged and school-aged children, possibly abnormal motor movements, including nonpurposeful, decorticate, or decerebrate responses to pain |
5 | Coma or vegetative state | Unawareness |
6 | Death | ― |
* Worst level of performance for any single criterion is used for categorizing. Deficits are scored only if they result from a neurologic disorder. Assessments are based on medical records or an interview with the caretaker. | ||
Adapted from Fiser DH. Assessing the outcome of pediatric intensive care. J Pediatr 121(1):68-74, 1992. doi:10.1016/s0022-3476(05)82544-2 | ||
ADLs = activities of daily living. | ||
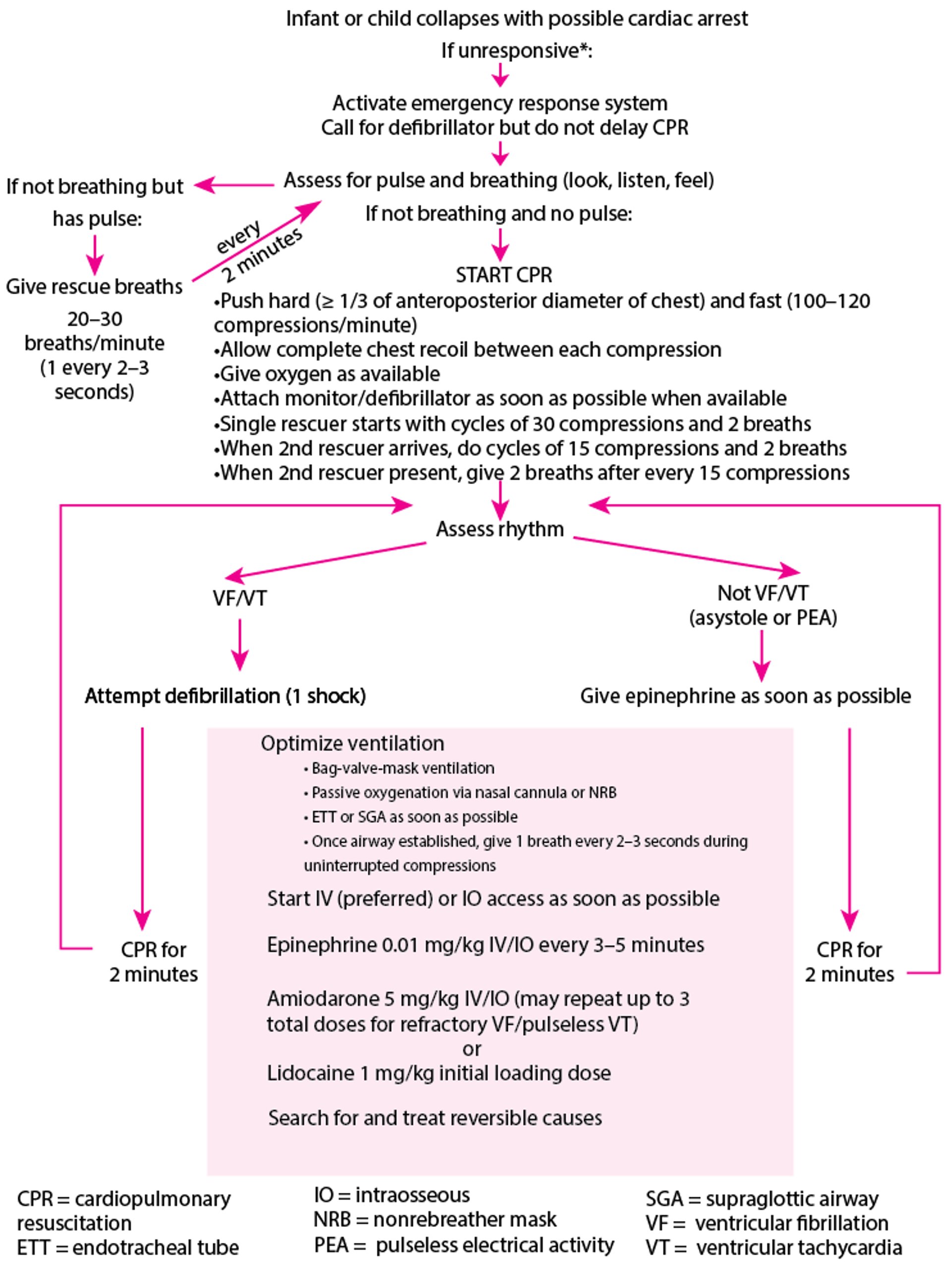
Standards and guidelines for CPR in infants and children from the American Heart association are followed (see table CPR Techniques for Health Care Professionals). For protocol after an infant or child has collapsed with possible cardiac arrest, see figure Pediatric Comprehensive Emergency Cardiac Care.
After CPR has been started, defibrillation and identification of the underlying cardiac rhythm are done.
Pediatric Comprehensive Emergency Cardiac Care
* If an adequate number of trained personnel are available, patient assessment, CPR, and activation of the emergency response system should occur simultaneously. |
Based on the Comprehensive Emergency Cardiac Care Algorithm from the American Heart Association. |

General reference
1. Jayaram N, McNally B, Tang F, Chan PS: Survival After Out-of-Hospital Cardiac Arrest in Children. J Am Heart Assoc 4(10):e002122, 2015. doi:10.1161/JAHA.115.002122
Major Differences Between Pediatric and Adult CPR
Prearrest
Bradycardia in a distressed child is a sign of impending cardiac arrest. Neonates, infants, and young children are more likely to develop bradycardia caused by hypoxemia, whereas older children initially tend to have tachycardia. An infant or child with a heart rate < 60/minute and signs of poor perfusion that do not rise with ventilatory support should have cardiac compressions (see figure Chest Compression in Infants and Children). Bradycardia secondary to heart block is unusual.
Chest compressions
During chest compressions in infants and children (below the age of puberty or < 55 kg), the chest should be depressed one-third of the anteroposterior diameter. This is approximately 4 to 5 cm. In adolescents or children > 55 kg, the recommended compression depth is the same as in adults, ie, 5 to 6 cm (see also chest compressions in adults).
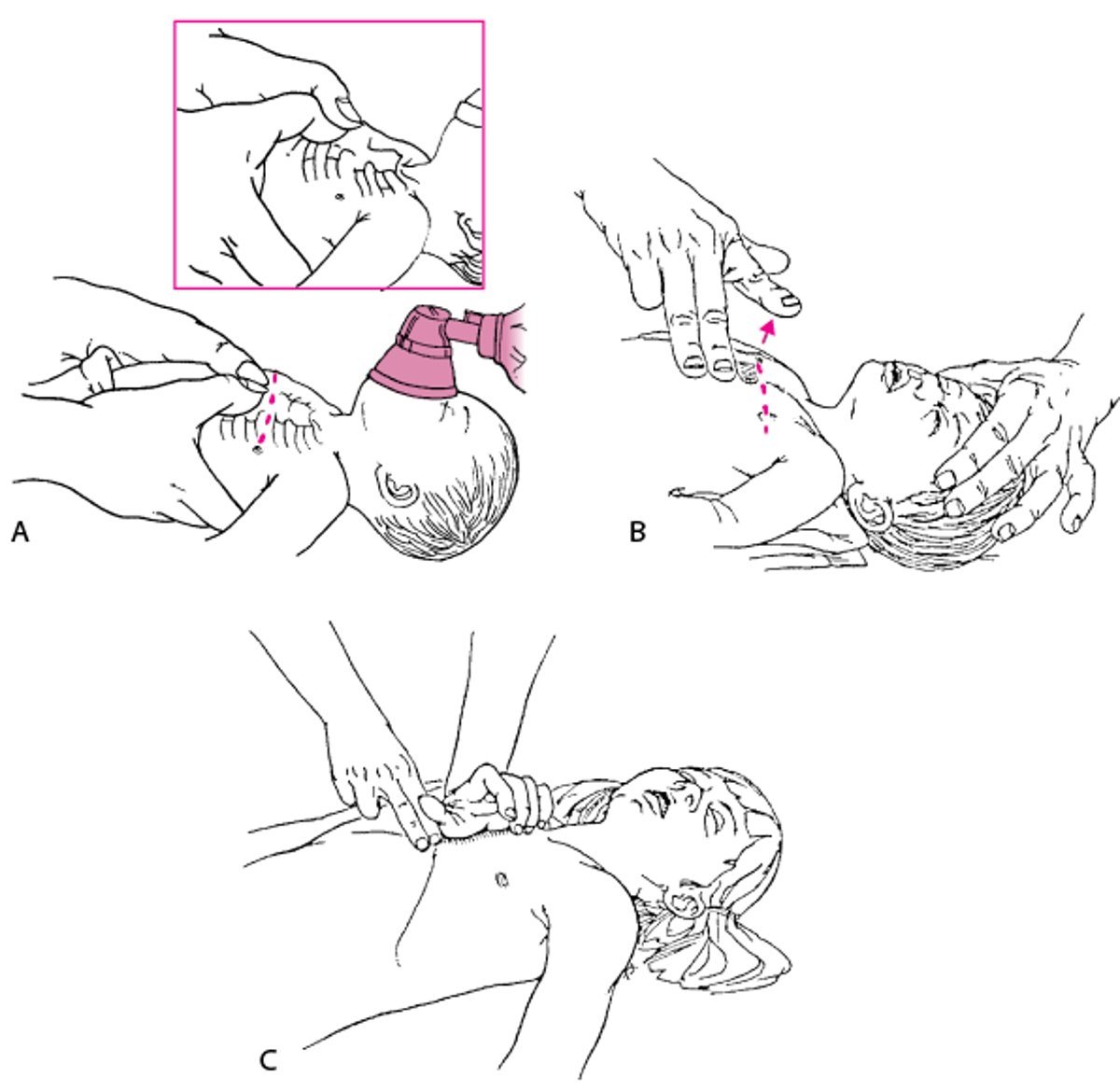
The method of chest compression is also different in infants and children (see figure Chest Compression in Infants and Children). The rate of compression in infants and children is similar to that of adults at 100 to 120 compressions/minute.
Chest Compression in Infants and Children
A: When 2 rescuers are present, side-by-side thumb placement for chest compressions is preferred for neonates and small infants whose chest can be encircled. Thumbs should overlap if used in very small neonates. B: Lone rescuers can use 2 fingers for infant compressions. Fingers should be maintained in the upright position during compression. For neonates, this technique results in too low a position, ie, at or below the xiphoid; the correct position is just below the nipple line. C: Hand position for chest compression for a child. (Adapted from American Heart Association: Standards and guidelines for CPR. Journal of the American Medical Association 268:2251–2281,1992. Copyright 1992, American Medical Association.) |

Medications
For non shockable rhythms, after CPR and adequate oxygenation and ventilation are established, epinephrine is the medication of choice (see For non shockable rhythms, after CPR and adequate oxygenation and ventilation are established, epinephrine is the medication of choice (seeFirst-line medications) and should be given as soon possible after establishment of intravenous (IV) or intraosseous (IO) access. Epinephrine dose is 0.01 mg/kg IV, which can be repeated every 3 to 5 minutes. Guidelines advise immediate IO placement and epinephrine administration for nonshockable rhythms, as evidence indicates that restoration of spontaneous circulation and survival rate in children is correlated with the speed at which the first dose of epinephrine is received () and should be given as soon possible after establishment of intravenous (IV) or intraosseous (IO) access. Epinephrine dose is 0.01 mg/kg IV, which can be repeated every 3 to 5 minutes. Guidelines advise immediate IO placement and epinephrine administration for nonshockable rhythms, as evidence indicates that restoration of spontaneous circulation and survival rate in children is correlated with the speed at which the first dose of epinephrine is received (1).
For shockable rhythms (ventricular fibrillation [VF] or pulseless ventricular tachycardia [pVT]), if defibrillation is unsuccessful, CPR is continued and epinephrine (0.01 mg/kg IV) is given every 3 to 5 minutes. If defibrillation is unsuccessful after epinephrine, amiodarone 5 mg/kg IV bolus can be given. Amiodarone may be repeated up to 2 times for refractory [pVT]), if defibrillation is unsuccessful, CPR is continued and epinephrine (0.01 mg/kg IV) is given every 3 to 5 minutes. If defibrillation is unsuccessful after epinephrine, amiodarone 5 mg/kg IV bolus can be given. Amiodarone may be repeated up to 2 times for refractoryventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). If amiodarone is not available, lidocaine may be given at a loading dose of 1 mg/kg IV followed by a maintenance infusion of 20 to 50 mcg/kg/minute. Neither is not available, lidocaine may be given at a loading dose of 1 mg/kg IV followed by a maintenance infusion of 20 to 50 mcg/kg/minute. Neitheramiodarone nor lidocaine have been shown to improve survival to hospital discharge.
Blood pressure
Blood pressure (BP) should be measured with an appropriate-sized cuff, but direct invasive arterial BP monitoring is mandatory in severely compromised children.
Because BP varies with age, an easy guideline to remember the lower limits of normal for systolic BP (< fifth percentile) by age is as follows:
< 1 month: 60 mm Hg
1 month to 1 year: 70 mm Hg
> 1 year: 70 + (2 × age in year)
Thus, in a 5-year-old child, hypotension would be defined by a BP of < 80 mm Hg (70 + [2 × 5]). Of significant importance is that children maintain BP longer because of stronger compensatory mechanisms (increased heart rate, increased systemic vascular resistance). Once hypotension occurs, cardiorespiratory arrest may rapidly follow. All effort should be made to start treatment when compensatory signs of shock (eg, increased heart rate, cool extremities, capillary refill > 2 seconds, poor peripheral pulses) are present but before hypotension develops.
Equipment and environment
Equipment size, medication dosage, and CPR parameters vary with patient age and weight (see tables CPR Techniques for Health Care Professionals, Medications Commonly Used for Resuscitation, and Guide to Pediatric Resuscitation). Size-variable equipment includes defibrillator paddles or electrode pads, masks, ventilation bags, airways, laryngoscope blades, endotracheal tubes, and suction catheters.
Weight should be measured rather than guessed; alternatively, commercially available measuring tapes that are calibrated to read standard patient weight based on body length can be used. Some tapes are printed with the recommended medication dose and equipment size for each weight. Dosages should be rounded down; eg, a 2 ½-year-old child should receive the dose for a 2-year-old child.
Guide to Pediatric Resuscitation—Mechanical Measures
Age (yr) | Term neonate | < 12 mo | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Weight, typical (kg) | 3.5 | < 10 | 10 | 12 | 14 | 16 | 18 | 20 | 22 | 25 | 28 | 30 | 35 | 40 | 45 | 50 | 55 | 60 | |
Compression techniques | Thumb compression, hands around chest (preferred) or 2 fingers | 1 hand | 2 hands | ||||||||||||||||
Airway ISO size P in cm | 000 | 00 | 00 | 0 | 0 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 8 | 8 | 8 | 8 | |
3.5 | 5 | 5 | 6 | 6 | |||||||||||||||
Masks in Laerdal sizes or equivalent | Circular 0/1 | Rendell- Baker type # 1 | Rendell-Baker type # 2 | Dome cuff mask # 3 | Dome cuff mask # 4 | ||||||||||||||
Ventilation bag with reservoir for 100% O2 delivery | Infant 240 mL | Child 400–500 mL | Adult 1600 mL | ||||||||||||||||
Laryngoscope blade size | Miller 0 Straight blade | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | |
Straight blade (preferred) or curved blade | Curved or straight blade | ||||||||||||||||||
ETT size* in mm | 3 | 3.5 | 4 | 4.5 | 4.5 | 5 | 5 | 5.5 | 5.5 | 6 | 6 | 6 | 6 | 6.5 | 6.5 | 6.5 | 6.5 | 7 | |
Uncuffed | Uncuffed | Cuffed | |||||||||||||||||
Laryngeal mask airways and other supraglottic airway devices* | |||||||||||||||||||
Suction catheter | Direct oropharyngeal Through ETT | 10 F | Pediatric tonsil suction 8 Fr | Adult tonsil suction 10 Fr | |||||||||||||||
* Refer to specific device manufacturer's sizing instructions. | |||||||||||||||||||
ETT = endotracheal tube; Fr = French. | |||||||||||||||||||
Courtesy of Dr. B. Paes and Dr. M. Sullivan, the Departments of Pediatrics and Medicine, St. Joseph’s Hospital, The Children’s Hospital, Hamilton Health Sciences Corporation, McMaster University, Hamilton, Ontario, Canada. | |||||||||||||||||||
Temperature management
Susceptibility to heat loss is greater in infants and children because of a large surface area relative to body mass and less subcutaneous tissue. A neutral external thermal environment (maintaining the infant's body temperature and a stable metabolic state with minimal oxygen and energy use) is crucial during CPR and postresuscitation. Hypothermia with core temperature < 35° C makes resuscitation more difficult.
For comatose children resuscitated from in-hospital and out-of-hospital cardiac arrest, American Heart Association and American Association of Pediatrics guidelines advise therapeutic hypothermia (32 to 36° C) or normothermia (36 to 37.5° C—2, 3 ). Fever should be treated aggressively.
Airway and ventilation
Upper airway anatomy in children differs from that of adults. The head is large with a small face, mandible, and external nares, and the neck is relatively short. The tongue is large relative to the mouth, and the larynx lies higher in the neck and is angled more anteriorly. The epiglottis is long, and the narrowest portion of the trachea is inferior to the vocal cords at the cricoid ring, allowing the use of uncuffed endotracheal tubes. In younger children, a straight laryngoscope blade generally allows better visualization of the vocal cords than a curved blade because the larynx is more anterior and the epiglottis is more floppy and redundant. Available evidence does not support improved patient outcomes in infants and children who have out-of-hospital cardiac arrest with the use of advanced airway interventions as compared to bag-valve-mask ventilation (4).
If only a single rescuer is present and if there is no advanced airway in place in infants and children undergoing resuscitation, the recommended compression:ventilation ratio is 30:2 ; if more than one rescuer is present, the ratio is 15:2. This recommendation is in contrast to that for adults where the compression:ventilation ratio is always 30:2 and is independent of the number of rescuers.
With an advanced airway in place, the 2020 International Liaison Committee on Resuscitation (ILCOR) guidelines for pediatric cardiac arrest resuscitation advise a ventilation rate of 20 to 30 breaths per minute (with the faster rate in infants) (3). However, this revised recommendation is based on a study of hospitalized patients and remains controversial in prehospital care (5). Many researchers of pediatric prehospital care continue to advise a ventilation rate of 10-breaths per minute.

Defibrillation
In asystole, atropine and pacing are not used.In asystole, atropine and pacing are not used.
Ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT) occur in approximately 15 to 20% of pediatric cardiac arrests (6). Vasopressin is not indicated. When defibrillation is used, the absolute energy dose is less than that for adults; waveform can be biphasic (preferred) or monophasic. For either waveform, the recommended energy dose is 2 joules/kg for the first shock, increasing to 4 joules/kg for subsequent attempts (if necessary—). Vasopressin is not indicated. When defibrillation is used, the absolute energy dose is less than that for adults; waveform can be biphasic (preferred) or monophasic. For either waveform, the recommended energy dose is 2 joules/kg for the first shock, increasing to 4 joules/kg for subsequent attempts (if necessary—see defibrillation in adults). The maximum recommended dose is 10 joules/kg or the maximum adult dose (200 joules for a biphasic defibrillator and 360 joules for a monophasic defibrillator).
Automated external defibrillators (AEDs) with adult cables may be used for children, but an AED with pediatric cables (maximum biphasic shock of 50 joules) is preferred for pediatric patients up to 8 years of age. Current guidelines recommend manual defibrillation if possible for pediatric patients, but an AED (with or without pediatric cables) can be used if a manual defibrillator is not immediately available (3). For pad placement, see defibrillation in adults.
Treatment references
1. Topjian AA, Raymond TT, Atkins D, et al: Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 142(16_suppl_2):S469–S523, 2020. doi:10.1161/CIR.0000000000000901
2. Granfeldt A, Holmberg MJ, Nolan JP, Soar J, Andersen LW; International Liaison Committee on Resuscitation (ILCOR) Advanced Life Support Task Force: Targeted temperature management in adult cardiac arrest: Systematic review and meta-analysis. Resuscitation 167:160–172, 2021. doi:10.1016/j.resuscitation.2021.08.040
3. Maconochie IK, Aickin R, Hazinski MF, et al: Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 156:A120–A155, 2020. doi:10.1016/j.resuscitation.2020.09.013
4. Jarvis JL, Panchal AR, Lyng JW, et al: Evidence-Based Guideline for Prehospital Airway Management. Prehosp Emerg Care 28(4):545–557, 2024. doi:10.1080/10903127.2023.2281363
5. Sutton RM, Reeder RW, Landis WP, et al: Ventilation Rates and Pediatric In-Hospital Cardiac Arrest Survival Outcomes. Crit Care Med 47(11):1627–1636, 2019. doi:10.1097/CCM.0000000000003898
6. López-Herce J, García C, Domínguez P, et al: Characteristics and outcome of cardiorespiratory arrest in children. Resuscitation 63(3):311–320, 2004. doi:10.1016/j.resuscitation.2004.06.008
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association 2020 CPR and ECC Guidelines: These guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) are based on the most recent review of resuscitation science, protocols, and education.







