


Epistaxis is nose bleeding. Bleeding can range from a trickle to a strong flow, and the consequences can range from a minor annoyance to life-threatening hemorrhage.
Pathophysiology of Epistaxis
Most nasal bleeding is anterior, originating from a plexus of vessels in the anteroinferior septum (Kiesselbach area).
Less common but more serious are posterior nosebleeds, which originate in the posterior septum overlying the vomer bone or laterally on the inferior or middle turbinate. Posterior nosebleeds tend to occur in patients who have preexisting atherosclerotic vessels or bleeding disorders and have had nasal or sinus surgery.
Etiology of Epistaxis
The most common causes of epistaxis are
Local trauma (eg, nose blowing and picking)
Drying of the nasal mucosa
There are a number of less common causes (see table Some Causes of Epistaxis). Hypertension may contribute to the persistence of a nosebleed that has already begun but is unlikely to be the sole etiology.
Some Causes of Epistaxis
Cause* | Suggestive Findings | Diagnostic Approach† |
|---|---|---|
Common | ||
Drying of the mucosa (eg, in cold weather) | Usually visibly dry during examination | Clinical examination alone |
Local trauma (eg, nose blowing, picking, blunt impact) | Apparent by history | Clinical examination alone |
Less common | ||
Usually in older patients | Clinical examination alone | |
History of prior epistaxis or other bleeding sites, such as gingiva | CBC with platelet count, PT/PTT | |
Foreign bodies (mainly in children) | Often recurrent epistaxis with a malodorous discharge from one nostril | Clinical examination alone |
Local infections (eg, vestibulitis, rhinitis) | Crusting in the nasal vestibule, often with local pain and dry mucosa | Clinical examination alone |
Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome) | Telangiectasias on the face, lips, oral and nasal mucosa, and tips of the fingers and toes Positive family history | Clinical examination alone |
Visible during examination | Clinical examination alone | |
Systemic disorders (eg, AIDS, liver disease) | Presence of known disease Mucosal erosions and hypertrophy | Clinical examination alone |
Tumor (benign or malignant) of the nasopharynx or paranasal sinuses | Mass seen within the nose or nasopharynx Bulging of the lateral nasal wall | CT |
* Epistaxis of any cause is more common among patients with bleeding disorders (eg, thrombocytopenia, liver disease, coagulopathies) and with anticoagulant use. In such patients, bleeding is also often more severe and difficult to treat. | ||
† Clinical examination is always done but is mentioned in this column only when that can be the sole means of diagnosis. | ||
CBC = complete blood count; CT = computed tomography; PT/PTT = prothrombin time/partial thromboplastin time. | ||
Evaluation of Epistaxis
History
History of present illness should try to determine which side began bleeding first; although major epistaxis quickly involves both nares, most patients can localize the initial flow to one side, which focuses the physical examination. Also, the duration of bleeding should be established, as well as any triggers (eg, sneezing, nose blowing, picking) and attempts by the patient to stop the bleeding. Melena may occur, and swallowed blood is a gastric irritant, so patients may also report vomiting blood. Important associated symptoms before onset include symptoms of an upper respiratory infection (URI), sensation of nasal obstruction, and nasal or facial pain. The time and number of previous nosebleeds and their resolution should be identified.
Review of systems should ask about excessive bleeding (particularly related to toothbrushing, phlebotomy, or minor trauma), easy bruising; bloody or tarry stools, hemoptysis, and blood in urine..
Past medical history
Physical examination
Vital signs should be reviewed for indications of intravascular volume depletion (tachycardia, hypotension) and marked hypertension. With active bleeding, treatment takes place simultaneously with evaluation.
During active bleeding, inspection is difficult, so attempts are first made to stop the bleeding as described below. The nose is then examined using a nasal speculum and a bright head lamp or head mirror, which leaves one hand free to manipulate suction or an instrument.
Anterior bleeding sites are usually apparent on direct examination. If no site is apparent and there have been only 1 or 2 minor nosebleeds, further examination is not needed. If bleeding is severe or recurrent and no site is seen, fiberoptic endoscopy may be necessary.
The general examination should look for signs of bleeding disorders, including petechiae, purpura, and perioral and oral mucosal telangiectasias as well as any intranasal masses.
Red flags
In patients with epistaxis, the following findings are of particular concern:
Signs of hypovolemia or hemorrhagic shock
Anticoagulant use
Cutaneous signs of a bleeding disorder
Bleeding not stopped by direct pressure or vasoconstrictor-soaked pledgets
Multiple recurrences of epistaxis, particularly with no clear cause
Interpretation of findings
Many cases of epistaxis have a clear-cut trigger (particularly nose blowing or picking), as suggested by findings (see table Some Causes of Epistaxis).
Testing
To diagnose epistaxis, routine laboratory testing is not required. If patients have symptoms or signs of a bleeding disorder and severe or recurrent epistaxis, a complete blood count (CBC), prothrombin time (PT), and partial thromboplastin time (PTT) should be done.
CT may be done if a foreign body, a tumor, or sinusitis is suspected.
Treatment of Epistaxis
Presumptive treatment for actively bleeding patients is that for anterior bleeding. The need for blood replacement is determined by the hemoglobin level, symptoms of anemia, and vital signs. Any identified bleeding disorders are treated.
Anterior epistaxis
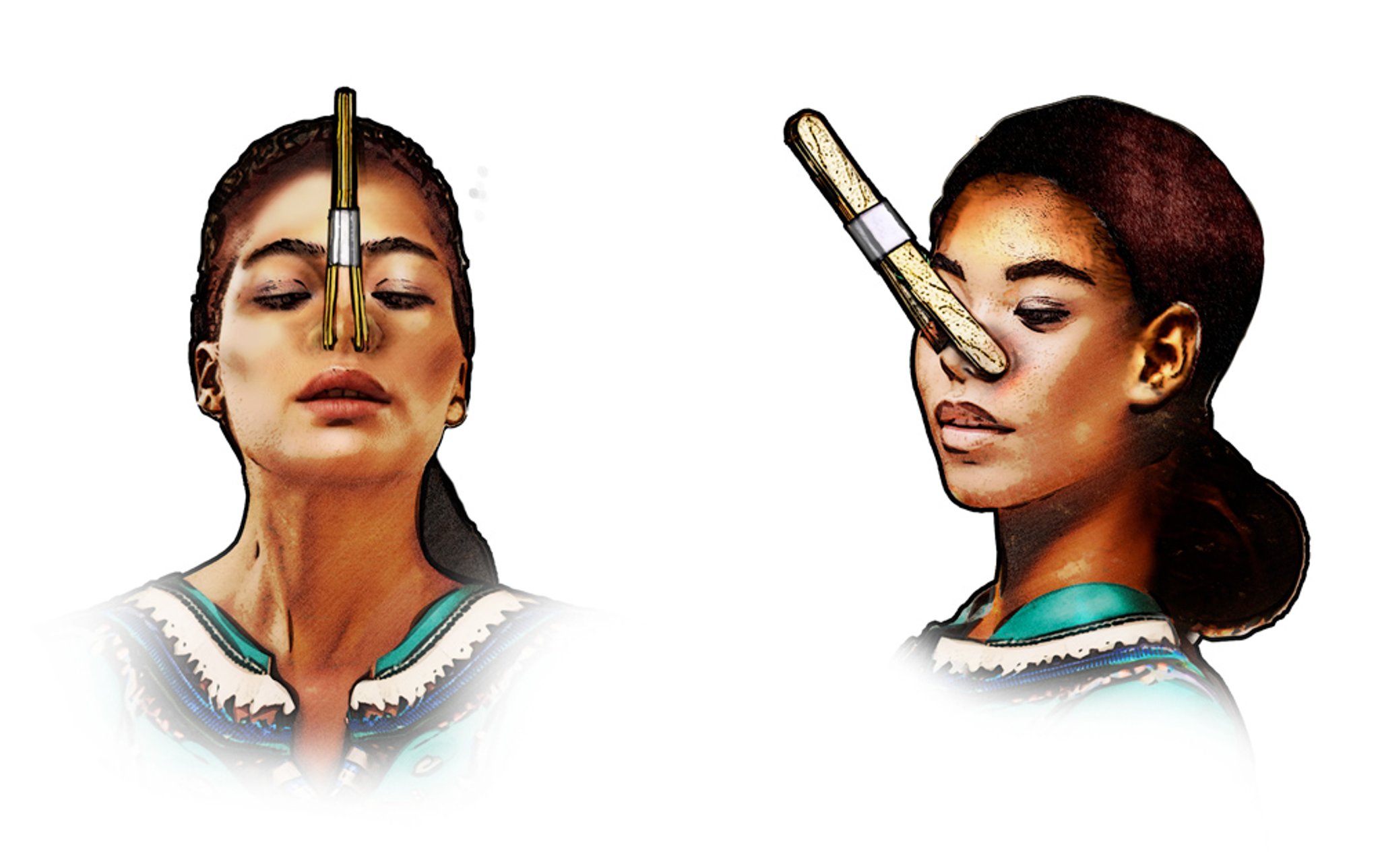
Bleeding can usually be controlled by pinching the nasal alae together for 10 minutes while the patient sits upright (if possible). The patient or a clinician can pinch the nose manually to compress the plexus of vessels in the anterior interior septum. Alternatively, a commercially available nasal clip can be used to pinch the nose. If a nasal clip is not available, a makeshift nasal clip can be fashioned from 4 tongue depressors taped together. Two tongue depressors are then positioned on each side of the nose to pinch the nasal alae.

Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
As another alternative, an anterior nasal pack consisting of 1 cm (1/2 inch) petrolatum gauze may be inserted; up to 175 cm (72 inch) of gauze may be required. This procedure is painful, and analgesics are usually needed; it should be done only when other methods are ineffective or unavailable.
Posterior epistaxis
Posterior bleeding may be difficult to control. Commercial nasal balloons are quick and convenient; a gauze posterior pack is effective but more difficult to position. Both are very uncomfortable; IV sedation and analgesia may be needed, and hospitalization is required.
Commercial balloons are inserted according to the instructions accompanying the product.
On occasion, the internal maxillary artery and its branches must be ligated to control the bleeding. The arteries may be ligated with clips using endoscopic or microscopic guidance and a surgical approach through the maxillary sinus (internal maxillary) or transnasal endoscopic approach (sphenopalatine). Alternatively, angiographic embolization may be done by a skilled radiologist. These procedures, if done in a timely manner, may shorten hospital stay.
Bleeding disorders
In hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome), a split-thickness skin graft (septal dermatoplasty) reduces the number of nosebleeds and allows the anemia to be corrected. Laser (Nd:YAG) photocoagulation can be done in the operating room. Selective embolization is also very effective, particularly if patients cannot tolerate general anesthesia or if surgical intervention has not been successful. New endoscopic sinus devices have made transnasal surgery more effective.
Key Points
Most nosebleeds are anterior and stop with direct pressure.
Screening (by history and physical examination) for bleeding disorders is important.







