


(See also Nonatheromatous Arteriosclerosis.)
Atherosclerosis is the most common form of arteriosclerosis, which is a general term for several disorders that cause thickening and loss of elasticity in the arterial wall. Atherosclerosis is also the most serious and clinically relevant form of arteriosclerosis because it causes coronary artery disease and cerebrovascular disease. Nonatheromatous forms of arteriosclerosis include arteriolosclerosis and Mönckeberg arteriosclerosis.
Atherosclerosis can affect all large and medium-sized arteries, including the coronary, carotid, and cerebral arteries; the aorta; its branches; and major arteries of the extremities. It is the leading cause of morbidity and mortality in the US and in most developed countries. Age-related mortality attributable to atherosclerosis has been decreasing, but in 2019, cardiovascular disease, primarily coronary and cerebrovascular atherosclerosis still caused about 18 million deaths worldwide (> 30% of all deaths [1]). In the US, about 558,000 people died of cardiovascular disease in 2019 (2). Atherosclerosis is rapidly increasing in prevalence in low and middle income countries, and as people live longer, incidence will increase. Atherosclerosis is the leading cause of death worldwide.

BSIP VEM/SCIENCE PHOTO LIBRARY
General references
1. Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2019. Geneva, World Health Organization, 2020.
2. Virani SS, Alonso A, Aparicio HJ, et al: Heart Disease and Stroke Statistics–2021 Update: A Report From the American Heart Association. Circulation 143(8):e254–e743, 2021. doi: 10.1161/CIR.0000000000000950
Pathophysiology of Atherosclerosis
The fatty streak is the earliest visible lesion of atherosclerosis; it is an accumulation of lipid-laden foam cells in the intimal layer of the artery.
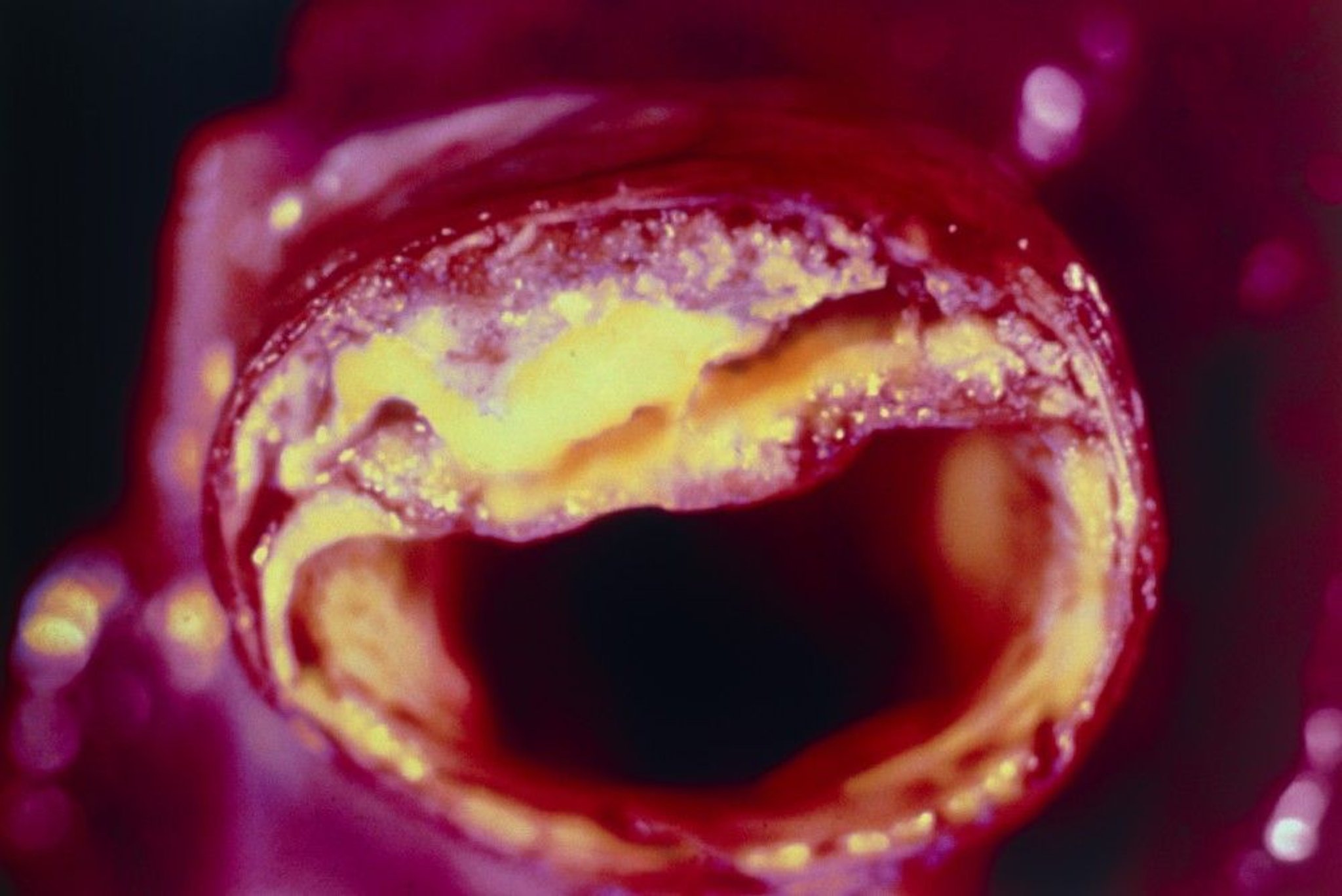
The atherosclerotic plaque is the hallmark of atherosclerosis; it is an evolution of the fatty streak and has 3 major components:
Lipids
Inflammatory and smooth muscle cells
A connective tissue matrix that may contain thrombi in various stages of organization and calcium deposits
Atherosclerotic plaque formation
All stages of atherosclerosis—from initiation and growth to complication of the plaque (eg, myocardial infarction, stroke) —are considered an inflammatory response to injury mediated by specific cytokines. Endothelial injury is thought to have a primary initiating or inciting role.
Nonlaminar or turbulent blood flow (eg, at branch points in the arterial tree) leads to endothelial dysfunction and inhibits endothelial production of nitric oxide, a potent vasodilator and anti-inflammatory molecule. Such blood flow also stimulates endothelial cells to produce adhesion molecules, which recruit and bind inflammatory cells. Nonlaminar or turbulent blood flow (eg, at branch points in the arterial tree) leads to endothelial dysfunction and inhibits endothelial production of nitric oxide, a potent vasodilator and anti-inflammatory molecule. Such blood flow also stimulates endothelial cells to produce adhesion molecules, which recruit and bind inflammatory cells.
Risk factors for atherosclerosis (eg, dyslipidemia, diabetes, cigarette smoking, hypertension), oxidative stressors (eg, superoxide radicals), angiotensin II, and systemic infection and inflammation also inhibit nitric oxide production and stimulate production of adhesion molecules, proinflammatory cytokines, chemotactic proteins, and vasoconstrictors; exact mechanisms are unknown. The net effect is endothelial binding of monocytes and T cells, migration of these cells to the subendothelial space, and initiation and perpetuation of a local vascular inflammatory response. ), oxidative stressors (eg, superoxide radicals), angiotensin II, and systemic infection and inflammation also inhibit nitric oxide production and stimulate production of adhesion molecules, proinflammatory cytokines, chemotactic proteins, and vasoconstrictors; exact mechanisms are unknown. The net effect is endothelial binding of monocytes and T cells, migration of these cells to the subendothelial space, and initiation and perpetuation of a local vascular inflammatory response.
Monocytes in the subendothelium transform into macrophages. Lipids in the blood, particularly low-density lipoprotein (LDL) cholesterol and very-low-density lipoprotein (VLDL) cholesterol, also bind to endothelial cells and are oxidized in the subendothelium. Uptake of oxidized lipids and macrophage transformation into lipid-laden foam cells result in the typical early atherosclerotic lesions called fatty streaks. Degraded erythrocyte membranes that result from rupture of vasa vasorum and intraplaque hemorrhage may be an important additional source of lipids within plaques.
Macrophages elaborate proinflammatory cytokines that recruit smooth muscle cell migration from the media and that further attract and stimulate growth of macrophages. Various factors promote smooth muscle cell replication and increase production of dense extracellular matrix. The result is a subendothelial fibrous plaque with a fibrous cap, made of intimal smooth muscle cells surrounded by connective tissue and intracellular and extracellular lipids. A process similar to bone formation causes calcification within the plaque.
A link between infection and atherosclerosis has been observed, specifically an association between serologic evidence of certain infections (eg, Chlamydia pneumoniae, cytomegalovirus) and coronary artery disease (CAD). Putative mechanisms include indirect effects of chronic inflammation in the bloodstream, cross-reactive antibodies, and inflammatory effects of infectious pathogens on the arterial wall. However, evidence in favor of such a link is conflicting, and infection likely plays a minor role in atherosclerosis.
Plaque stability and rupture
Atherosclerotic plaques may be stable or unstable.
Stable plaques regress, remain static, or grow slowly over several decades until they may cause stenosis or occlusion.
Unstable plaques are vulnerable to spontaneous erosion, fissure, or rupture, causing acute thrombosis, occlusion, and infarction long before they cause hemodynamically significant stenosis. Most clinical events result from unstable plaques, which are often not hemodynamically significant on angiography; thus, plaque stabilization may be a way to reduce morbidity and mortality.
The strength of the fibrous cap and its resistance to rupture depend on the relative balance of collagen deposition and degradation. Plaque rupture involves secretion of metalloproteinases, cathepsins, and collagenases by activated macrophages in the plaque. These enzymes digest the fibrous cap, particularly at the edges, causing the cap to thin and ultimately rupture. T cells in the plaque contribute by secreting cytokines. Cytokines inhibit smooth muscle cells from synthesizing and depositing collagen, which normally reinforces the plaque.
Once the plaque ruptures, plaque contents are exposed to circulating blood, triggering thrombosis; macrophages also stimulate thrombosis because they contain tissue factor, which promotes thrombin generation in vivo. One of 5 outcomes may occur: Once the plaque ruptures, plaque contents are exposed to circulating blood, triggering thrombosis; macrophages also stimulate thrombosis because they contain tissue factor, which promotes thrombin generation in vivo. One of 5 outcomes may occur:
The resultant thrombus may organize and be incorporated into the plaque, changing the plaque’s shape and causing its rapid growth.
The thrombus may rapidly occlude the vascular lumen and precipitate an acute ischemic event.
The thrombus may embolize.
The plaque may fill with blood, balloon out, and immediately occlude the artery.
Plaque contents (rather than thrombus) may embolize, occluding vessels downstream.
Plaque stability depends on multiple factors, including plaque composition (relative proportion of lipids, inflammatory cells, smooth muscle cells, connective tissue, and thrombus), wall stress (cap fatigue), size and location of the core, and configuration of the plaque in relation to blood flow. By contributing to rapid growth and lipid deposition, intraplaque hemorrhage may play an important role in transforming stable into unstable plaques.
In general, unstable coronary artery plaques have a high macrophage content, a thick lipid core, and a thin fibrous cap; they narrow the vessel lumen by < 50% and tend to rupture unpredictably. Unstable carotid artery plaques have the same composition but typically cause problems through severe stenosis and occlusion or deposition of platelet thrombi, which embolize rather than rupture. Low-risk plaques have a thicker cap and contain fewer lipids; they often narrow the vessel lumen by > 50% and may produce predictable exercise-induced stable angina.
Clinical consequences of plaque rupture in coronary arteries depend not only on that anatomical location of the plaque anatomy but also on relative balance of procoagulant and anticoagulant activity in the blood and on the vulnerability of the myocardium to arrhythmias.
Risk Factors for Atherosclerosis
There are numerous risk factors for atherosclerosis (1—see table Risk Factors for Atherosclerosis). Certain factors tend to cluster as the metabolic syndrome. This syndrome includes abdominal obesity, atherogenic dyslipidemia, hypertension, insulin resistance, a prothrombotic state, and a proinflammatory state in sedentary patients. Insulin resistance is not synonymous with the metabolic syndrome but may be key in its etiology.
Risk Factors for Atherosclerosis
Status | Risk Factor |
|---|---|
Nonmodifiable | Age Family history of premature atherosclerosis* Male sex |
Modifiable, established | Certain dyslipidemias (eg, increased apolipoprotein B particles) Tobacco smoking |
Modifiable, under study or emerging | Alcohol intake (other than moderate) Chlamydia pneumoniae infection High apolipoprotein B (apoB) level High C-reactive protein (CRP) level High level of small, dense LDL High lipoprotein (a) level Hyperinsulinemia Hypertriglyceridemia Low intake of fruits and vegetables Obesity or the metabolic syndrome Prothrombotic states (eg, hyperfibrinogenemia, high plasminogen activator inhibitor level) Prothrombotic states (eg, hyperfibrinogenemia, high plasminogen activator inhibitor level) Psychosocial factors (eg, type A personality, depression, anxiety, work characteristics, socioeconomic status) Radiation therapy to thorax Renal insufficiency Sedentary lifestyle† |
* Atherosclerosis is premature when it occurs in a male 1st-degree relative before age 55 and in a female 1st-degree relative before age 65. | |
† How much this factor contributes independent of other frequently associated risk factors (eg, diabetes, dyslipidemia) is unclear. | |
CRP = C-reactive protein, HDL = high-density lipoprotein cholesterol, LDL = low-density lipoprotein cholesterol. | |
Dyslipidemia (high total, high LDL, or low high-density lipoprotein [HDL] cholesterol), hypertension, and diabetes promote atherosclerosis by amplifying or augmenting endothelial dysfunction and inflammatory pathways in vascular endothelium.
In dyslipidemia, subendothelial uptake and oxidation of LDL increases; oxidized lipids stimulate production of adhesion molecules and inflammatory cytokines and may be antigenic, inciting a T cell–mediated immune response and inflammation in the arterial wall. Although HDL was previously believed to protect against atherosclerosis via reverse cholesterol transport and by transporting antioxidant enzymes, which can break down and neutralize oxidized lipids, evidence from randomized trials and genetics suggests a much less important role for HDL in atherogenesis. The role of hypertriglyceridemia in atherogenesis is complex, although it may have a small independent effect (2). The main determinant for risk of atherogenic cardiovascular disease is the concentration of atherogenic lipoproteins, which is best reflected by the apolipoprotein B (apoB) concentration (or by the non-HDL-C concentration, if apoB is unavailable).
Hypertension may lead to vascular inflammation via angiotensin II–mediated mechanisms. Angiotensin II stimulates endothelial cells, vascular smooth muscle cells, and macrophages to produce proatherogenic mediators, including proinflammatory cytokines, superoxide anions, prothrombotic factors, growth factors, and lectin-like oxidized LDL receptors.may lead to vascular inflammation via angiotensin II–mediated mechanisms. Angiotensin II stimulates endothelial cells, vascular smooth muscle cells, and macrophages to produce proatherogenic mediators, including proinflammatory cytokines, superoxide anions, prothrombotic factors, growth factors, and lectin-like oxidized LDL receptors.
Diabetes leads to the formation of advanced glycation end products, which increase the production of proinflammatory cytokines from endothelial cells. Oxidative stress and reactive oxygen radicals, generated in diabetes, directly injure the endothelium and promote atherogenesis.
Chronic kidney disease promotes development of atherosclerosis via several pathways, including worsening hypertension and insulin resistance; decreased apolipoprotein A-I levels; and increased lipoprotein(a), homocysteine, fibrinogen, and C-reactive protein levels.
Prothrombotic states (see Overview of Thrombotic Disorders) increase likelihood of atherothrombosis.
Tobacco smoke contains nicotine and other chemicals that are toxic to vascular endothelium. Smoking, including passive smoking, increases platelet reactivity (possibly promoting platelet thrombosis) and plasma fibrinogen levels and hematocrit (increasing blood viscosity). Smoking increases LDL and decreases HDL; it also promotes vasoconstriction, which is particularly dangerous in arteries already narrowed by atherosclerosis. HDL increases rapidly within 1 month of smoking cessation.
Lipoprotein (a) [Lp(a)] is pro-atherogenic and is an independent risk factor for cardiovascular disease, including myocardial infarction, stroke, and aortic valve stenosis (3, 4). It has a structure similar to LDL, but it also has a hydrophilic apolipoprotein(a) component that is covalently bound to a hydrophobic apolipoprotein B100 (5). Lp(a) levels are genetically determined and remain fairly stable throughout life. Lp(a) levels above 50 mg/dL are considered pathogenic.
Apolipoprotein (B) (apoB) is a particle with two isoforms: apoB-100, which is synthesized in the liver, and apoB-46, which is synthesized in the intestine. ApoB-100 is able to bind the LDL receptor and is responsible for cholesterol transport. It is also responsible for transport of oxidized phospholipids and has proinflammatory properties. Presence of the apoB particle within the arterial wall is thought to be the initiating event for the development of atherosclerotic lesions.
A high level of small, dense LDL, characteristic of diabetes, is highly atherogenic. Mechanisms may include increased susceptibility to oxidation and nonspecific endothelial binding.
A high C-reactive protein (CRP) level does not reliably predict extent of atherosclerosis but can predict increased likelihood of ischemic events. In the absence of other inflammatory disorders, elevated levels may indicate increased risk of atherosclerotic plaque rupture, ongoing ulceration or thrombosis, or increased activity of lymphocytes and macrophages. CRP itself does not appear to have a direct role in atherogenesis.
Heart transplantation is often followed by accelerated coronary atherosclerosis, which is likely related to immune-mediated endothelial injury. Accelerated coronary atherosclerosis is also observed after thoracic radiation therapy and is likely the result of radiation-induced endothelial injury.
C. pneumoniae infection or other infections (eg, viral, Helicobacter pylori) may cause endothelial dysfunction through direct infection, exposure to endotoxin, or stimulation of systemic or subendothelial inflammation.
Several common and rare genetic variants (eg, near 9p21, LPA and LDLR gene)have been robustly associated with atherosclerosis and cardiovascular events. Although each variant has a small effect individually, genetic risk scores that sum the total number of risk variants have been shown to strongly associate with more advanced atherosclerosis as well as both primary and recurrent cardiovascular events
Patients with hyperhomocysteinemia (eg, due to folate deficiency or a genetic metabolic defect) have an increased risk of atherosclerosis. However, because of results from randomized trials of homocysteine lowering therapies that fail to show a decrease in atherosclerotic disease, as well as evidence from Mendelian randomization trials, it is no longer thought that hyperhomocysteinemia itself causes atherosclerosis. The reason for the association between elevated homocysteine levels and atherosclerosis is unclear.
Documented vascular disease
The presence of atherosclerotic disease in one vascular territory increases the likelihood of disease in other vascular territories. Patients with noncoronary atherosclerotic vascular disease have cardiac event rates comparable to those of patients with known CAD, and they are now considered to have a CAD risk equivalent and should be treated as aggressively.
Risk factor references
1. Yusuf S, Hawken S, Ounpuu S, et al: Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 364: 937–952, 2004.
2. White J, Swedlow DI, Preiss D, et al: Association of lipid fractions with risks for coronary artery disease and diabetes. JAMA Cardiol 1: 692–699, 2016.
3. Emerging risk factors collaboration, Eroquo S, Kaptoge S, Perry PL, et al: Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA 302: 412–423, 2009.
4. Thanassoulis, G, Campbell CY, Owens DS, et al for the CHARGE Extracoronary Calcium Working Group: Genetic associations with valvular calcification and aortic stenosis. N Engl J Med 368: 503–512, 2013.
5. Nordestgaard BG, Chapman MJ, Ray K, et al and the European Atherosclerosis Society Consensus Panel: Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J 31: 2844–2853, 2010.
Symptoms and Signs of Atherosclerosis
Atherosclerosis is initially asymptomatic, often for decades. Symptoms and signs develop when lesions impede blood flow. Transient ischemic symptoms (eg, stable exertional angina, transient ischemic attacks, intermittent claudication) may develop when stable plaques grow and reduce the arterial lumen by > 70%. Vasoconstriction can change a lesion that does not limit blood flow into a severe or complete stenosis.
Symptoms of unstable angina or myocardial infarction, ischemic stroke, or rest pain in the limbs may develop when unstable plaques rupture and acutely occlude a major artery, with superimposition of thrombosis or embolism. Atherosclerosis may also cause sudden death without preceding stable or unstable angina pectoris.
Atherosclerotic involvement of the arterial wall can lead to aneurysms and arterial dissection, which can manifest as pain, a pulsatile mass, absent pulses, or sudden death.
Diagnosis of Atherosclerosis
Approach to diagnosis of atherosclerosis depends on the presence or absence of symptoms.
Symptomatic patients
Patients with symptoms and signs of ischemia are evaluated for the amount and location of vascular occlusion by various invasive and noninvasive tests, depending on the organ involved (see elsewhere in THE MANUAL). Such patients also should be evaluated for atherosclerosis risk factors by using
History and physical examination
Fasting lipid profile
Plasma glucose and glycosylated hemoglobin (HbA1C) levels
Patients with documented disease at one site (eg, peripheral arteries) should be evaluated for disease at other sites (eg, coronary and carotid arteries).
Noninvasive imaging techniques that can assess plaque morphology and characteristics include
Three-dimensional vascular ultrasonography, which can be used to assess plaque in the carotid and other arteries
Computed tomography (CT) angiography, which is used clinically to identify significant lesions in the coronary arteries
Magnetic resonance (MR) angiography, which is used sometimes to image large arteries (eg, aorta)
Invasive catheter-based tests are also used. These include
Intravascular ultrasonography, which uses an ultrasound transducer on the tip of a catheter to produce images of the arterial lumen and wall
Angioscopy, which uses special fiberoptic catheters that can directly visualize the arterial surface
Plaque thermography, which is used to detect the increased temperature in plaques with active inflammation
Optical coherence tomography, which uses infrared laser light for imaging
Elastography, which is used to identify soft, lipid-rich plaques
Immunoscintigraphy is a noninvasive alternative that uses radioactive tracers that localize in vulnerable plaque. Positron emission tomography (PET) imaging of the vasculature is another emerging approach to assess vulnerable plaque.
Because not all atherosclerotic plaques have similar risk, various imaging technologies (eg, positron emission tomography) are being studied as a way to identify plaques especially vulnerable to rupture; however, these techniques are not yet used clinically.


© Springer Science+Business Media
In addition to the fasting lipid profile and plasma glucose and hemoglobin A1C measurements, some clinicians measure serum markers of inflammation. High-sensitivity C-reactive protein levels ≥ 3.1 mg/L (≥ 29.5 nmol/L) are highly predictive of cardiovascular events.
Asymptomatic patients (screening)
In patients with risk factors for atherosclerosis but no symptoms or signs of ischemia, the role of additional testing beyond the lipid profile is unclear. Although imaging studies such as carotid ultrasonography to measure intimal medial thickness and other studies that can detect atherosclerotic plaque are being studied, they do not reliably improve prediction of ischemic events over assessment of risk factors or established prediction tools and are not recommended. An exception is CT imaging for coronary artery calcium (ie, to obtain a calcium score), for which there is more robust evidence for risk reclassification; it may be useful for refining risk estimates and for deciding on statin therapy in select patients (eg, those with intermediate risk, family history of premature cardiovascular disease).
Most guidelines recommend lipid profile screening in patients with any of the following characteristics:
Men ≥ 40 years
Women ≥ 40 years and post-menopausal women
Family history of familial hypercholesterolemia or premature cardiovascular disease (ie, age of onset < 55 years in male 1st degree relative, or < 65 years in female 1st degree relative)
Type 2 diabetes
Hypertension
Metabolic syndrome
Chronic kidney disease (estimated glomerular filtration rate [eGFR] ≤ 60 mL/minute/1.73 m2 or albumin-to-creatinine ratio [ACR] ≥ 3 mg/mmol)or albumin-to-creatinine ratio [ACR] ≥ 3 mg/mmol)
Current cigarette smoking
Chronic inflammatory conditions
HIV infection
History of hypertensive disorder of pregnancy (preeclampsia or eclampsia)
Currently, the American Heart Association (AHA) recommends using the pooled cohort risk assessment equations (see Downloadable AHA Risk Calculator) to estimate lifetime and 10-year risk of atherosclerotic cardiovascular disease. This calculator has replaced previous risk calculation tools (eg, Framingham score). The new risk calculator is based on sex, age, race, total and HDL cholesterol levels, systolic blood pressure (and whether blood pressure is being treated), diabetes, and smoking status (1). The European Cardiovascular Society (ESC) and the European Atherosclerosis Society (EAS) 2016 guideline suggests using the Systemic Coronary Risk Estimation (SCORE), which calculates risk based on age, gender, smoking, systolic blood pressure, and total cholesterol, to estimate the 10-year risk of the first fatal atherosclerotic event (2). For patients deemed at intermediate risk, lipoprotein(a) measurement has been suggested to help refine classification (3, 4).

Urinary albuminuria (> 30 mg albumin/24 hours) is a marker for renal disorders and their progression, as well as a strong predictor of cardiovascular and noncardiovascular morbidity and mortality; however, the direct relationship between albuminuria and atherosclerosis has not been established.30 mg albumin/24 hours) is a marker for renal disorders and their progression, as well as a strong predictor of cardiovascular and noncardiovascular morbidity and mortality; however, the direct relationship between albuminuria and atherosclerosis has not been established.
Diagnosis references
1. Arnett DK, Blumenthal RS, Albert MA, et al: 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 74:1376–1414, 2019.
2. Catapano AL, Graham I, De Backe G, et al: 2016 ESC/EAS guidelines for the management of dyslipidaemias: The task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) developed with the special contribution of the European Association for Cardiovascular Prevention and Rehabilitation (EACPR). Eur Heart J 37: 2999–3058, 2016. doi:10.1093/eurheartj/ehw272
3. Pearson GJ, Thanassoulis G, Anderson TJ, et al: 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Can J Cardiol 37:1129–1150, 2021.
4. Willeit P, Kiechl S, Kronenberg F, et al: Discrimination and net reclassification of cardiovascular risk with lipoprotein(a): prospective 15-year outcomes in the Bruneck Study. J Am Coll Cardiol 64: 851–860, 2014. doi: 10.1016/j.jacc.2014.03.061
Treatment of Atherosclerosis
Lifestyle changes (diet, smoking, physical activity)
Drug treatment of diagnosed risk factors
Antiplatelet drugs
Statins, possibly angiotensin-converting enzyme (ACE) inhibitors, beta-blockers
Treatment involves aggressive modification of risk factors to slow progression and induce regression of existing plaques. Lowering LDL cholesterol to below a certain target is no longer recommended, and "the lower the better" approach is currently favored.
Lifestyle changes include diet modification, smoking cessation, and regular participation in physical activity. Drugs to treat dyslipidemia, hypertension, and diabetes are often required. These lifestyle changes and drugs directly or indirectly improve endothelial function, reduce inflammation, and improve clinical outcome. Statins can decrease atherosclerosis-related morbidity and mortality even when serum cholesterol is normal or slightly high. Antiplatelet drugs help all patients with atherosclerosis. Patients with coronary artery disease may benefit additionally from ACE inhibitors and beta-blockers.
Diet
Several changes are beneficial:
Less saturated fat
No trans fats
Fewer refined carbohydrates
More fruits and vegetables
More fiber
Moderate (if any) alcohol
Substantial decreases in saturated fat and refined and processed carbohydrates and increases in carbohydrates with fiber (eg, fruits, vegetables) are recommended. These dietary changes are a prerequisite for lipid control and weight reduction and are essential for all patients. Calorie intake should be limited to keep weight within the normal range.
Small decreases in fat intake do not appear to lessen or stabilize atherosclerosis. Effective change requires limiting fat intake to 20 g a day, consisting of 6 to 10 g of polyunsaturated fat with omega-6 (linoleic acid) and omega-3 (eicosapentaenoic acid, docosahexaenoic acid) fatty acids in equal proportion, ≤ 2 g of saturated fat, and the rest as monounsaturated fat. Trans fats, which are highly atherogenic, should be avoided.
Increasing carbohydrates to compensate for decreasing saturated fats in the diet increases plasma triglyceride levels and reduces HDL levels. Thus, any caloric deficiency should be made up with proteins and unsaturated fats rather than simple carbohydrates. Excessive fat and refined sugar intake should be avoided, especially in people at risk of diabetes, although sugar intake has not been directly related to cardiovascular risk. Instead, consumption of complex carbohydrates (eg, vegetables, whole grains) is encouraged.
Fruits and vegetables (5 daily servings) seem to decrease risk of coronary atherosclerosis, but whether this effect is due to phytochemicals or to a proportional decrease in saturated fat intake and increase in fiber and vitamin intake is unclear. Phytochemicals called flavonoids (in red and purple grapes, red wine, black teas, and dark beers) appear especially protective; high concentrations in red wine may help explain why incidence of coronary atherosclerosis in the French is relatively low, even though they use more tobacco and consume more fat than Americans do. But no clinical data indicate that eating flavonoid-rich foods or using supplements instead of foods prevents atherosclerosis.
Increased fiber intake decreases total cholesterol and may have a beneficial effect on glucose and insulin levels. Daily intake of at least 5 to 10 g of soluble fiber (eg, oat bran, beans, soy products, psyllium) is recommended; this amount decreases LDL by about 5%. Insoluble fiber (eg, cellulose, lignin) does not appear to affect cholesterol but may confer additional health benefits (eg, reduced risk of colon cancer, possibly by stimulating bowel movement or reducing contact time with dietary carcinogens). However, excessive fiber interferes with the absorption of certain minerals and vitamins. In general, foods rich in phytochemicals and vitamins are also rich in fiber.levels. Daily intake of at least 5 to 10 g of soluble fiber (eg, oat bran, beans, soy products, psyllium) is recommended; this amount decreases LDL by about 5%. Insoluble fiber (eg, cellulose, lignin) does not appear to affect cholesterol but may confer additional health benefits (eg, reduced risk of colon cancer, possibly by stimulating bowel movement or reducing contact time with dietary carcinogens). However, excessive fiber interferes with the absorption of certain minerals and vitamins. In general, foods rich in phytochemicals and vitamins are also rich in fiber.
Alcohol increases HDL and has poorly defined antithrombotic, antioxidant, and anti-inflammatory properties. These effects appear to be the same for wine, beer, and hard liquor, and occur at moderate levels of consumption; about 30 mL of ethanol (1 oz, contained in about 2 average servings of typical alcoholic beverages) 5 to 6 times a week protects against coronary atherosclerosis. However, at higher doses, alcohol can cause significant health problems. Thus, the relationship between alcohol and total mortality rate is J-shaped; mortality rate is lowest for men who consume < 14 drinks a week and women who consume < 9 drinks a week. People who consume greater amounts of alcohol should cut back. However, clinicians are hesitant to recommend that nondrinkers begin consuming alcohol based on any apparent protective effect.
There is little evidence that dietary supplementation with vitamins, phytochemicals, and trace minerals reduces risk of atherosclerosis. The one exception is fish oil supplements. Although alternative medicines and health foods are becoming more popular, and some may have minor effects on blood pressure or cholesterol, these treatments are not always proven safe or effective and may have negative interactions with proven drugs. Levels of coenzyme Q10, which is necessary for the basic functioning of cells, tend to decrease with age and may be low in patients with certain heart and other chronic diseases; thus, coenzyme Q10 supplementation has been used or recommended, but its therapeutic benefit remains controversial.
Physical activity
Regular physical activity (eg, 30 to 45 minutes of walking, running, swimming, or cycling 3 to 5 times a week) reduces incidence of some risk factors (hypertension, dyslipidemia, diabetes), coronary artery disease (eg, myocardial infarction), and death attributable to atherosclerosis in patients with and without previous ischemic events. Whether the association is causal or merely indicates that healthier people are more likely to exercise regularly is unclear.
Optimal intensity, duration, frequency, and type of exercise have not been established, but most evidence suggests an inverse linear relationship between aerobic physical activity and risk. Walking regularly increases the distance patients with peripheral vascular disease can walk without pain.
An exercise program that involves aerobic exercise has a clear role in preventing atherosclerosis and promoting weight loss. Before starting a new exercise program, older people and people who have risk factors for atherosclerosis or who have had recent ischemic events should be evaluated by a physician. Evaluation includes history, physical examination, and assessment of risk factor control.
Antiplatelet drugs
Oral antiplatelet drugs are essential because most complications result from plaque fissure or rupture, leading to platelet activation and thrombosis. The following are used:
AspirinAspirin
Thienopyridine drugs such as clopidogrel, prasugrel, and ticagrelorThienopyridine drugs such as clopidogrel, prasugrel, and ticagrelor
Aspirin is most widely used but, despite its proven benefits, remains underused. It is indicated for secondary prevention and may be considered for primary prevention of coronary atherosclerosis in patients at very high risk (eg, patients with diabetes with or without atherosclerosis, patients with Aspirin is most widely used but, despite its proven benefits, remains underused. It is indicated for secondary prevention and may be considered for primary prevention of coronary atherosclerosis in patients at very high risk (eg, patients with diabetes with or without atherosclerosis, patients with≥ 20% risk of cardiac events within 10 years in whom bleeding risk is not prohibitive, and patients at intermediate risk who have a 10 to 20% risk of cardiac events within 10 years and have low risk of bleeding). Recent evidence suggests that the net-benefit of aspirin in primary prevention is questionable, especially in lower risk individuals, and that careful selection of patients is needed based on patient preferences and after considering the potential risks and benefits of aspirin for each individual (ie, potential harm in patients > 70 years or patients at higher risk for bleeding). in primary prevention is questionable, especially in lower risk individuals, and that careful selection of patients is needed based on patient preferences and after considering the potential risks and benefits of aspirin for each individual (ie, potential harm in patients > 70 years or patients at higher risk for bleeding).
Optimal dose and duration are unknown, but aspirin 81 to 325 mg orally once a day indefinitely is commonly used for primary and secondary prevention. However, 81 mg is preferred because this dose may minimize the risk of bleeding, particularly when Optimal dose and duration are unknown, but aspirin 81 to 325 mg orally once a day indefinitely is commonly used for primary and secondary prevention. However, 81 mg is preferred because this dose may minimize the risk of bleeding, particularly whenaspirin is used in combination with other antithrombotic drugs. In about 10 to 20% of patients taking aspirin for secondary prevention, ischemic events recur. The reason may be aspirin resistance; assays to detect lack of thromboxane suppression (indicated by elevated urinary 11-dehydrothromboxane B2) are being studied for clinical use.
Some evidence suggests that ibuprofen can interfere with Some evidence suggests that ibuprofen can interfere withaspirin’s antithrombotic effect, so other nonsteroidal anti-inflammatory drugs (NSAIDs) are recommended for patients taking aspirin for prevention. However, all NSAIDs, some more than others, including cyclooxygenase 2 (COX-2) selective inhibitors, appear to increase cardiovascular risks.
Clopidogrel (usually 75 mg orally once a day) is substituted for Clopidogrel (usually 75 mg orally once a day) is substituted foraspirin when ischemic events recur in patients taking aspirin and in patients intolerant of aspirin. Clopidogrel in combination with aspirin is effective in treating acute ST-segment and non-ST-segment elevation myocardial infarction; the combination is also given for 12 months after percutaneous intervention (PCI) to reduce risk of recurrent ischemic events. Resistance to clopidogrel also occurs. Prasugrel and ticagrelor are newer and more effective drugs than also occurs. Prasugrel and ticagrelor are newer and more effective drugs thanclopidogrel for coronary disease prevention in select patient groups.
Ticlopidine is no longer widely used because it causes severe neutropenia in 1% of users and has severe GI adverse effects.
Statins
Statins primarily lower LDL cholesterol. Other potential beneficial effects include enhanced endothelial nitric oxide production, stabilization of atherosclerotic plaques, reduced lipid accumulation in the arterial wall, and regression of plaques. Statins are recommended as preventive therapy in 4 groups of patients (Statins primarily lower LDL cholesterol. Other potential beneficial effects include enhanced endothelial nitric oxide production, stabilization of atherosclerotic plaques, reduced lipid accumulation in the arterial wall, and regression of plaques. Statins are recommended as preventive therapy in 4 groups of patients (1), comprised of those with any of the following:
Clinical atherosclerotic cardiovascular disease
LDL cholesterol ≥ 190 mg/dL (≥ 4.92 mmol/L)
Age 40 to 75 years, with diabetes and LDL cholesterol 70 to 189 mg/dL (1.81 to 4.90 mmol/L)
Age 40 to 75 years, with LDL cholesterol 70 to 189 mg/dL, and estimated 10-year risk of arteriosclerotic cardiovascular disease ≥ 7.5%
There is also support for the use of statins in patients with other risk factors, including family history of premature arteriosclerotic cardiovascular disease (ie, age of onset < 55 in male 1st degree relative, or < 65 in female 1st degree relative), high-sensitivity C-reactive protein ≥ 2 mg/L (19.05 nmol/L), coronary artery calcium score ≥ 300 Agatston units (or ≥ 75th percentile for the patient's demographic), ankle-brachial blood pressure index < 0.9, or chronic kidney disease not treated with dialysis or kidney transplantation.
Statin treatment is classified as high, moderate, or low intensity and is given based on treatment group and age (see table Statins for ASCVD Prevention). Specific LDL cholesterol targets are no longer recommended to guide lipid-lowering therapy. Instead, response to therapy is determined by whether LDL cholesterol levels decrease as expected based on therapy intensity (ie, patients receiving high-intensity therapy should have a ≥ 50% decrease in LDL cholesterol).
Other drugs
Angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers, ezetimibe, and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have anti-inflammatory properties that reduce risk of atherosclerosis independent of their effects on blood pressure and lipid, and glucose levels. The receptor blockers, ezetimibe, and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have anti-inflammatory properties that reduce risk of atherosclerosis independent of their effects on blood pressure and lipid, and glucose levels. Thefactor Xa inhibitor rivaroxaban also decreases risk of cardiovascular events although the mechanism of this effect is unknown.inhibitor rivaroxaban also decreases risk of cardiovascular events although the mechanism of this effect is unknown.
ACE inhibitors and angiotensin II receptor blockers inhibit the contributions of angiotensin to endothelial dysfunction and inflammation.
Ezetimibe also lowers LDL cholesterol by blocking the uptake of cholesterol from the small intestine via inhibition of the Niemann-Pick C1-like 1 protein. Ezetimibe also lowers LDL cholesterol by blocking the uptake of cholesterol from the small intestine via inhibition of the Niemann-Pick C1-like 1 protein.Ezetimibe, added to standard statin therapy, has been shown to reduce cardiovascular events in patients with prior cardiovascular event and LDL cholesterol > 70 mg/dL (1.8 mmol/L).
PCSK9 inhibitors are monoclonal antibodies that keep PCSK9 from attaching to LDL receptors, leading to increased recycling of these receptors to the plasma membrane leading to further clearance of plasma LDL cholesterol to the liver. LDL cholesterol is lowered by 40 to 70%. Long-term clinical trials have shown reduction in atherosclerosis and cardiovascular events. These drugs are most useful in patients with familial hypercholesterolemia, patients with prior cardiovascular events whose LDL is not at goal despite maximal medical therapy with statins, and patients who require lipid lowering but have documented objective evidence of statin intolerance.
The factor Xa inhibitor rivaroxaban at a dose of 2.5 mg orally twice a day decreases risk of cardiovascular events (cardiovascular death, stroke, or myocardial infarction) in patients with stable atherosclerotic vascular disease when added to aspirin 100 mg daily. The risk of major bleeding was higher in patients on inhibitor rivaroxaban at a dose of 2.5 mg orally twice a day decreases risk of cardiovascular events (cardiovascular death, stroke, or myocardial infarction) in patients with stable atherosclerotic vascular disease when added to aspirin 100 mg daily. The risk of major bleeding was higher in patients onrivaroxaban and aspirin than in patients on aspirin alone (than in patients on aspirin alone (2).
Icosapent ethyl, a highly purified form of eicosapentaoic acid, a key omega-3 fatty acid, has been shown to reduce cardiovascular events, in addition to statins, in patients with prior cardiovascular disease and elevated triglycerides. The mechanism appears multifactorial (eg reduced inflammation, reduced platelet reactivity, direct anti-atherogenic effects). Icosapent ethyl, a highly purified form of eicosapentaoic acid, a key omega-3 fatty acid, has been shown to reduce cardiovascular events, in addition to statins, in patients with prior cardiovascular disease and elevated triglycerides. The mechanism appears multifactorial (eg reduced inflammation, reduced platelet reactivity, direct anti-atherogenic effects).
Thiazolidinediones may control expression of proinflammatory genes, although studies suggest that they increase the risk of coronary events.
Folate (folic acid) 0.8 mg orally twice a day has been previously used to treat hyperhomocysteinemia but does not appear to reduce the risk of acute coronary events. Vitamins B6 and B12 also lower homocysteine levels, but current data do not justify their use alone or in combination with folate.Folate (folic acid) 0.8 mg orally twice a day has been previously used to treat hyperhomocysteinemia but does not appear to reduce the risk of acute coronary events. Vitamins B6 and B12 also lower homocysteine levels, but current data do not justify their use alone or in combination with folate.
Macrolide and other antibiotics given to treat chronic occult C. pneumoniae infections (and thereby suppress inflammation and theoretically alter the course and manifestations of atherosclerosis) have not been shown useful.
RNA-based therapies, a new class of drugs block production of key proteins at the mRNA level, often in hepatocytes. Inclisiran (blocks PCSK9), pelacarsen (blocks LPA), olpasiran (blocks LPA), and volanesorsen (blocks apoC3) are examples of these drugs that are currently being evaluated in randomized trials of cardiovascular prevention. RNA-based therapies, a new class of drugs block production of key proteins at the mRNA level, often in hepatocytes. Inclisiran (blocks PCSK9), pelacarsen (blocks LPA), olpasiran (blocks LPA), and volanesorsen (blocks apoC3) are examples of these drugs that are currently being evaluated in randomized trials of cardiovascular prevention.
Treatment references
1. Grundy SM, Stone NJ, Bailey AL, et al: 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 139(25):e1082–e143, 2019.
2. Eikelboom JW, Connolly SJ, Bosch J, et al: Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 377:1319–1330, 2017. doi: 10.1056/NEJMoa1709118
Key Points
Risk factors for atherosclerosis include dyslipidemia, diabetes, hypertension, obesity, sedentary lifestyle, cigarette smoking, family history, and psychosocial factors.
Unstable plaques often cause < 50% stenosis, yet are more prone to rupture and cause acute thrombosis or embolic phenomena than are larger, stable plaques.
In asymptomatic patients, imaging tests to detect atherosclerosis probably do not help predict ischemic events better than standard assessment of risk factors.
Stopping smoking, exercising, eating a diet low in saturated fat and refined carbohydrates and high in fiber and possibly consuming omega-3 fatty acids and moderate amounts of alcohol help in prevention and treatment.
Antiplatelet drugs and, depending on patient factors, statins and/or angiotensin-converting enzyme (ACE) inhibitors also are helpful.





