


Excess tearing may cause a sensation of watery eyes or result in tears falling down the cheek (epiphora).
Pathophysiology of Tearing
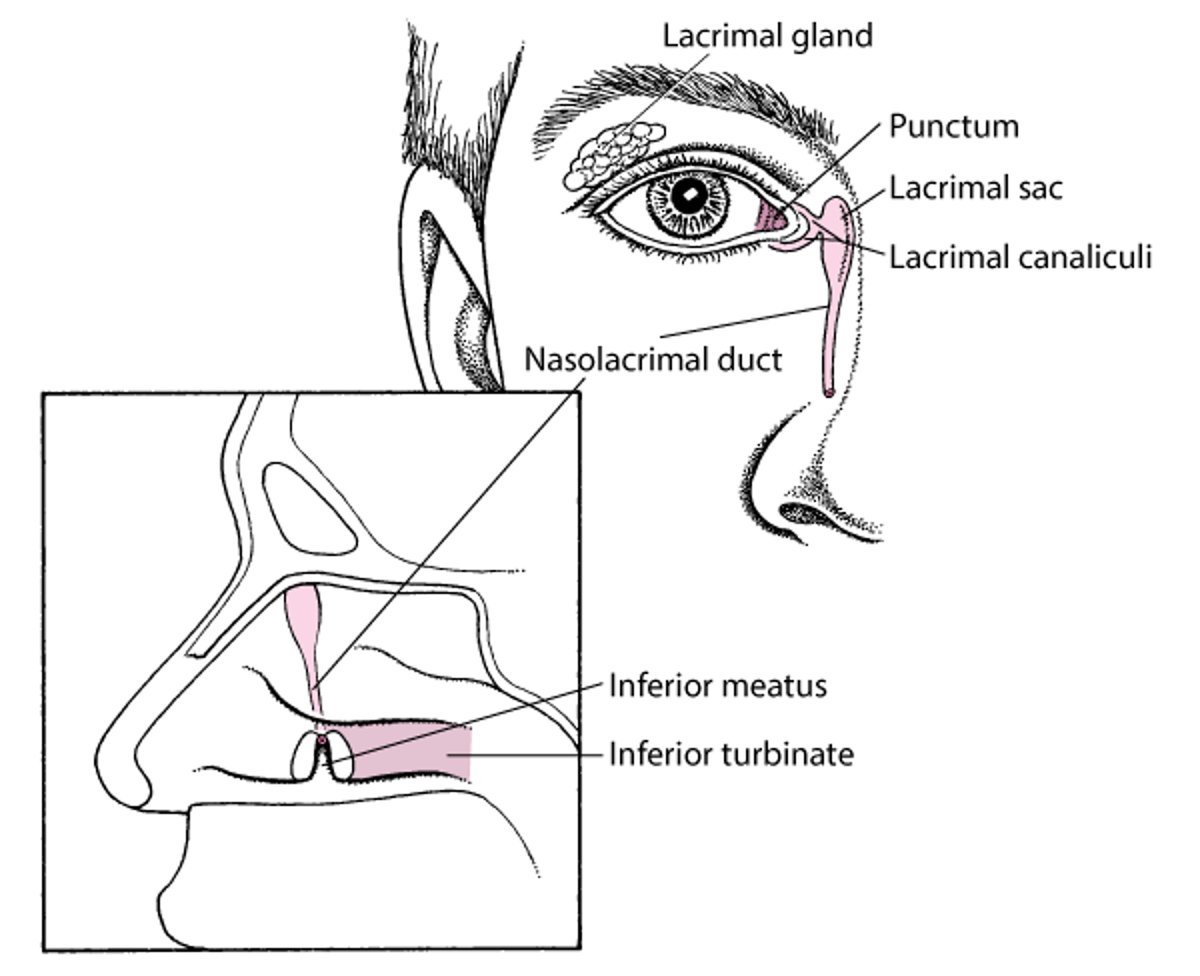
Tears are produced in the lacrimal gland and drain through the upper and lower puncta into the canaliculi and then into the lacrimal sac and nasolacrimal duct (see figure Anatomy of the Lacrimal System). Obstruction of tear drainage can lead to stasis and infection. Recurrent infection of the lacrimal sac (dacryocystitis) can sometimes spread, potentially leading to orbital cellulitis.
Anatomy of the Nasolacrimal System

Etiology of Tearing
Overall, the most common causes of tearing are
Upper respiratory infection
Allergic rhinitis
Tearing can be caused by increased tear production or decreased nasolacrimal drainage. In many patients, the cause of tearing can be multifactorial.
Increased tear production
The most common causes are
Upper respiratory infection
Dry eyes (reflex tearing produced in response to dryness of the ocular surface)
Any disorder causing conjunctival or corneal irritation can increase tear production (see table Some Causes of Tearing). However, most patients with corneal disorders that cause excess tearing (eg, corneal abrasion, corneal ulcer, corneal foreign body, keratitis) or with primary angle-closure glaucoma or anterior uveitis present with eye symptoms other than tearing (eg, eye pain, redness). Most people who have been crying do not present for evaluation of tearing.
Decreased nasolacrimal drainage
The most common causes are
Idiopathic age-related nasolacrimal duct stenosis
Nasolacrimal drainage system obstruction may be caused by strictures, tumors, or foreign bodies (eg, stones, often associated with subclinical infection by Actinomyces). Obstruction can also be a congenital malformation. Many disorders and medications can cause stricture or obstruction of nasolacrimal drainage.
Some Causes of Tearing
Cause | Suggestive Findings |
|---|---|
Disorders causing excess tear production | |
Dry eyes with reflex tearing | Worse on cold or windy days or with exposure to cigarette smoke or dry heat Intermittent foreign body sensation In patients with a disorder known to cause dry eyes (eg, blepharitis) |
Ocular surface irritation (eg, allergic conjunctivitis, corneal abrasion or erosion or ulcer, foreign body, hordeolum, infectious conjunctivitis, irritant chemicals, keratitis, trichiasis, irritation with punctate lesions due to paresis of blink muscles as in facial nerve palsy) | Grittiness Redness In patients with corneal lesions, pain, constant foreign body sensation, and photophobia |
Itching Possibly papillae on tarsal conjunctiva | |
Nasal irritation and inflammation (eg, allergic rhinitis, upper respiratory infection) | Rhinorrhea, sneezing, nasal congestion |
Disorders causing nasolacrimal drainage obstruction | |
Symptoms that begin shortly after age 2 weeks | |
Idiopathic age-related nasolacrimal duct stenosis | Usually normal examination except for evidence of obstruction |
Nasal pain Often swelling, redness, and warmth over the lacrimal sac and, with palpation, tenderness and expression of pus | |
Tumors | Hard mass in the nasolacrimal duct system, particularly in older adults |
Other causes of nasolacrimal drainage stricture or obstruction | Often risk factors (eg, burns, injuries, certain medications) Often no characteristic examination findings other than obstruction |
Disorders causing decreased drainage without obstruction | |
Misalignment between tear film and puncta (eg, ectropion, entropion) | Usually visible on examination |
Other causes of nasolacrimal drainage stricture or obstruction include
Burns
Chemotherapy drugs
Eye drops (particularly echothiophate iodide, epinephrine, and pilocarpine)
Infection, including canaliculitis (eg, caused by Staphylococcus aureus, Actinomyces, Streptococcus, Pseudomonas, herpes zoster virus, herpes simplex conjunctivitis, infectious mononucleosis, human papillomavirus, Ascaris, leprosy, tuberculosis)
Inflammatory disorders (sarcoidosis, granulomatosis with polyangiitis)
Injuries (eg, nasoethmoid fractures; nasal, orbital, or endoscopic sinus surgery)
Obstruction of nasal outlet despite an intact nasolacrimal system (eg, upper respiratory infection, allergic rhinitis, sinusitis)
Radiation therapy
Evaluation of Tearing
History
History of present illness addresses the duration, onset, and severity of symptoms, including whether tears drip down the cheek (true epiphora). The effects of weather, environmental humidity, and cigarette smoke are ascertained.
Review of symptoms should seek symptoms of possible causes, including itching, rhinorrhea, or sneezing, particularly when occurring perennially or after exposure to specific potential allergens (allergic reaction); eye irritation or pain (blepharitis, corneal abrasion, irritant chemicals); and pain near the medial canthus (dacryocystitis). Other symptoms are of lower yield but should be sought; they include positional headache, purulent rhinorrhea, nocturnal cough, and fever (sinusitis, granulomatosis with polyangiitis); rash (Stevens-Johnson syndrome); cough, dyspnea, and chest pain (sarcoidosis); and epistaxis, hemoptysis, polyarthralgias, and myalgias (granulomatosis with polyangiitis).
Past medical history asks about known disorders that can cause tearing, including granulomatosis with polyangiitis, sarcoidosis, and cancer treated with chemotherapy medications; disorders that cause dry eyes (eg, rheumatoid arthritis, sarcoidosis, Sjögren syndrome); and medications, such as echothiophate, epinephrine, and pilocarpine. Previous ocular and nasal history, including infections, injuries, surgical procedures, and radiation exposure, is ascertained.
Physical examination
Examination focuses on the eye and surrounding structures.
The face is inspected; asymmetry suggests congenital or acquired obstruction of nasolacrimal duct drainage. When available, a slit lamp should be used to examine the eyes. The conjunctivae and corneas are inspected for lesions, including punctate spots, and redness. The cornea is stained with fluorescein and examined. The lids are everted to detect hidden foreign bodies. The eyelids, including the lacrimal puncta, are closely inspected for foreign bodies, blepharitis, hordeola, ectropion, entropion, and trichiasis. The lacrimal sac (near the medial canthus) is palpated for warmth, tenderness, and swelling. Any swellings are palpated for consistency and to see whether pus is expressed.
The nose is examined for congestion, purulence, and bleeding.
Red flags
The following findings are of particular concern:
Repeated, unexplained episodes of tearing
Hard mass in or near the nasolacrimal drainage structures
Interpretation of findings
Findings that suggest obstruction of nasolacrimal drainage include:
Tears running down the cheek (true epiphora)
Absence of a different specific cause
For a list of common causes that may be evident from the Ophthalmic evaluation, see table Some Causes of Tearing.
Testing
Testing is often unnecessary because the cause is usually evident from the examination.
Schirmer test with a large amount of wetting (eg, > 25 mm) suggests an evaporative dry eye as the etiology of tearing. Schirmer test with very little wetting (< 5.5 mm) suggests an aqueous tear-deficient dry eye. Usually, Schirmer test is done by an ophthalmologist to ensure it is done and interpreted correctly.
Probing and saline irrigation of the lacrimal drainage system can help detect anatomic obstruction of drainage, as well as stenosis due to complete obstruction of the nasolacrimal drainage system. Irrigation is done with and without fluorescein dye. Reflux through the opposite punctum (eg, the eye's upper punctum if the lower punctum was irrigated) or canaliculus signals fixed obstruction; reflux and nasal drainage signify stenosis. This test is considered adjunctive and is done by ophthalmologists.
Imaging tests and procedures (dacryocystography, CT, nasal endoscopy) are sometimes useful to delineate abnormal anatomy when surgery is being considered or occasionally to detect an abscess. Recurrent infectious dacryocystitis can progress to more serious disorders such as orbital cellulitis.
Treatment of Tearing
Underlying disorders (eg, allergies, foreign bodies, conjunctivitis) are treated.
The use of artificial tears paradoxically lessens reflex tearing when dry eyes or corneal epithelial defects are the cause.
Congenital nasolacrimal duct obstruction often resolves spontaneously. In patients < 1 year, manual compression of the lacrimal sac 4 or 5 times a day may relieve the distal obstruction. After 1 year, the nasolacrimal duct may need probing with the patient under general anesthesia. If obstruction is recurrent, a temporary drainage tube may be inserted.
In acquired nasolacrimal duct obstruction, irrigation of the nasolacrimal duct may be therapeutic when underlying disorders do not respond to treatment. As a last resort, a passage between the lacrimal sac and the nasal cavity can be created surgically (dacryocystorhinostomy).
In cases of punctal or canalicular stenosis, dilation is usually curative. If canalicular stenosis is severe and bothersome, a surgical procedure that places a glass tube leading from the caruncle into the nasal cavity can be considered.
Geriatrics Essentials: Tearing
Idiopathic age-related nasolacrimal duct stenosis is the most common cause of unexplained epiphora in older patients; however, tumors should also be considered.
Key Points
If tears do not run down the cheek, dry eyes is often the cause.
If tears run down the cheek, obstruction of nasolacrimal drainage is likely.
Testing (dacryocystography, CT, nasal endoscopy) is often unnecessary but may be needed when surgery is being considered or occasionally to detect an abscess.







