


Uveitis is defined as inflammation of the uveal tract—the iris, ciliary body, and choroid. However, the retina and fluid within the anterior chamber and vitreous are often involved as well. About half of cases are idiopathic; identifiable causes include trauma, infection, and systemic diseases, many of which are autoimmune. Symptoms include decreased vision, ocular ache, redness, photophobia, and floaters. Although uveitis is identified clinically, identifying the cause typically requires testing. Treatment depends on the cause but typically includes topical, locally injected, or systemic corticosteroids with a topical cycloplegic-mydriatic medication. Noncorticosteroid immunosuppressive medications may be used in severe and refractory noninfectious cases.

Uveitis is inflammation of the uveal tract (see figure Cross Section of the Eye). Uveitis is classified anatomically as (1)
Anterior uveitis: Localized primarily to the anterior segment of the eye, includes iritis (inflammation in the anterior chamber alone) and iridocyclitis (inflammation in the anterior chamber and anterior vitreous)
Intermediate uveitis: Localized to the vitreous cavity and/or pars plana (part of the ciliary body that extends posteriorly beyond the junction of the iris and sclera)
Posterior uveitis: Any form of retinitis, choroiditis, or inflammation of the optic disk
Panuveitis: Inflammation involving anterior, intermediate, and posterior structures
Uveitis is also classified by onset (sudden or insidious), duration (limited or persistent), and course (acute, recurrent, or chronic).
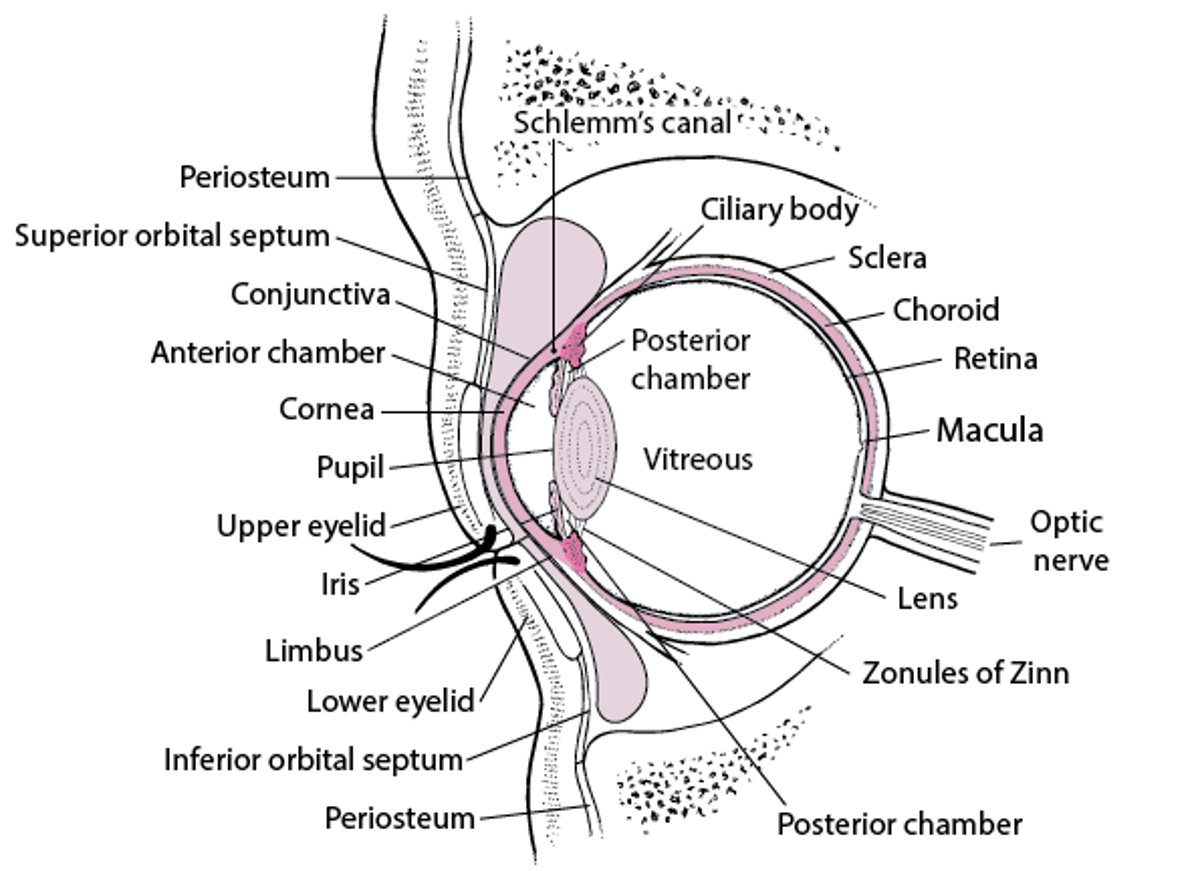
Cross Section of the Eye
The zonules of Zinn keep the lens suspended, and the muscles of the ciliary body focus the lens. The ciliary body also secretes aqueous humor, which fills the anterior and posterior chambers, passes through the pupil into the anterior chamber, and drains primarily via the Schlemm canal. The iris regulates the amount of light entering the eye by adjusting the size of its central opening, the pupil. Visual images are focused on the retina. The conjunctiva covers the eyeball and lines the upper and lower eyelids; it ends at the limbus. The cornea is covered with epithelium that is more sensitive than and differs from the conjunctival epithelium. |

General reference
1. Jabs DA, Nussenblatt RB, Rosenbaum JT, et al: Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol 140(3):509-516, 2005. doi: 10.1016/j.ajo.2005.03.057
Etiology of Uveitis
Causes of anterior uveitis include
Idiopathic or postsurgical (most common cause)
Trauma
Herpesvirus infection (herpes simplex virus [HSV], varicella-zoster virus [VZV], and cytomegalovirus [CMV])
Tubulointerstitial nephritis and uveitis (TINU)
Causes of intermediate uveitis include
Idiopathic (most common)
Tuberculosis (TB)
Lyme disease (in endemic regions)
Causes of posterior uveitis (retinitis) include
Idiopathic (most common)
CMV (in immunocompromised patients)
Causes of panuveitis include
Idiopathic (most common)
Infrequently, systemic medications cause uveitis (usually anterior). Examples are sulfonamides, bisphosphonates (inhibitors of bone resorption), rifabutin, cidofovir, antivascular endothelial growth factor (anti-VEGF) agents, and chemotherapy agents, including checkpoint inhibitors and BRAF/MEK protein kinase inhibitors.Infrequently, systemic medications cause uveitis (usually anterior). Examples are sulfonamides, bisphosphonates (inhibitors of bone resorption), rifabutin, cidofovir, antivascular endothelial growth factor (anti-VEGF) agents, and chemotherapy agents, including checkpoint inhibitors and BRAF/MEK protein kinase inhibitors.
Symptoms and Signs of Uveitis
Symptoms and signs may be subtle and vary depending on the site and severity of inflammation.
Anterior uveitis tends to be the most symptomatic (especially when acute), usually manifesting with
Pain (ocular ache)
Redness
Photophobia
Decreased vision (to a variable degree)
Chronic anterior uveitis may have less dramatic symptoms such as irritation or decreased vision, or symptoms may be absent.
Signs include hyperemia of the conjunctiva adjacent to the cornea (ciliary flush or limbal injection). Slit-lamp findings include keratic precipitates (white blood cell clumps on the inner corneal surface), cells and flare (a haze) in the anterior chamber (aqueous humor), and posterior synechiae. With severe anterior uveitis, white blood cells may layer in the anterior chamber (hypopyon).


Image courtesy of Sunir Garg, MD.
Intermediate uveitis is typically painless and manifests with
Floaters
Decreased vision
The primary sign is cells in the vitreous humor. Aggregates and condensations of inflammatory cells often occur, appearing as "snowballs." Vision may be decreased because of floaters or cystoid macular edema, which results from fluid leakage from blood vessels in the macula. Confluent and condensed vitreous cells and snowballs over the pars plana (part of the ciliary body that extends posteriorly beyond the junction of the iris and sclera) may cause a classic "snowbank" appearance, which can be associated with neovascularization of the retinal periphery (1).

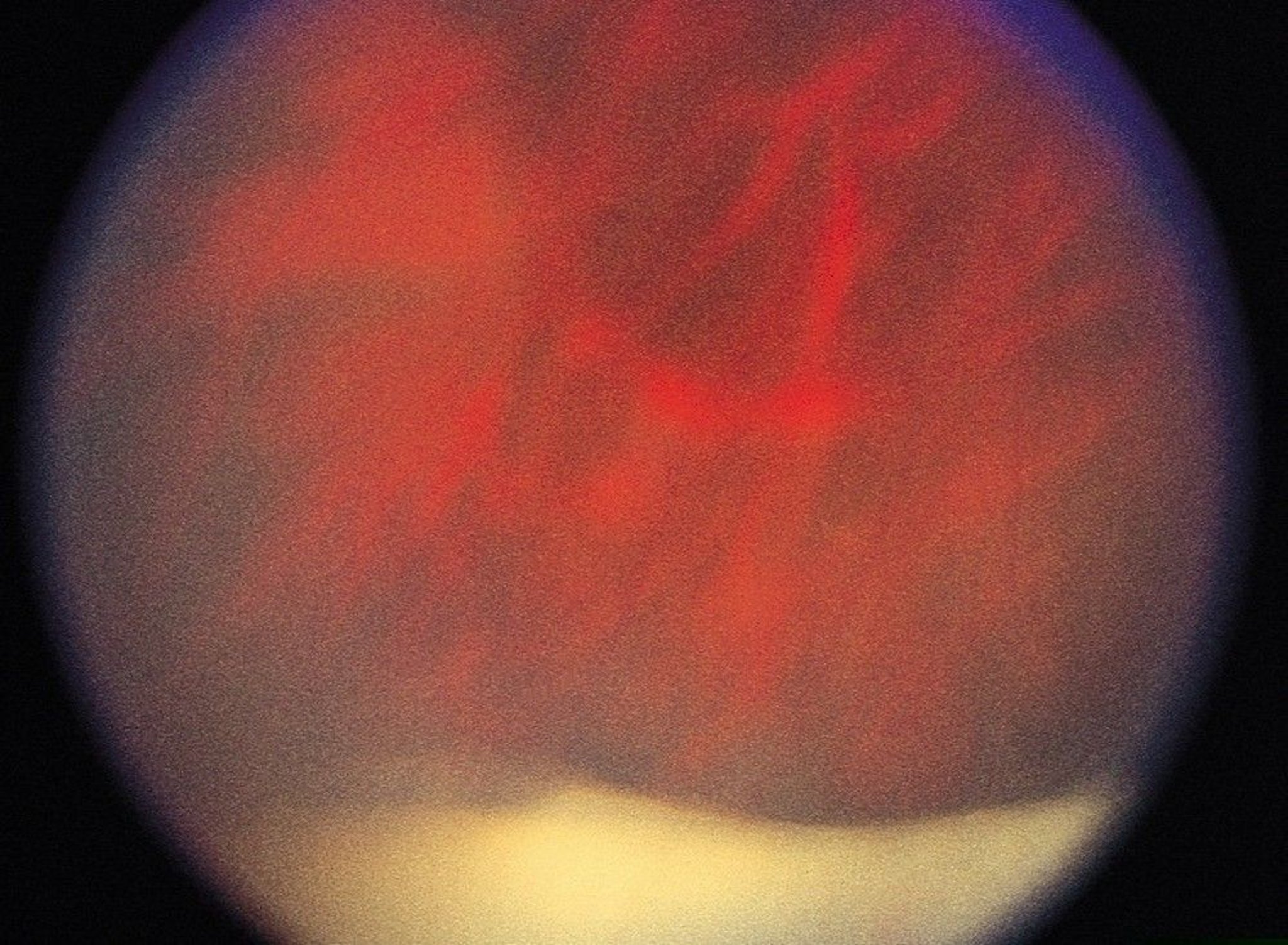
© Springer Science+Business Media
Posterior uveitis may give rise to diverse symptoms but most commonly causes floaters and decreased vision as occurs in intermediate uveitis. Signs include
Cells in the vitreous humor
White or yellow-white lesions in the retina (retinitis), underlying choroid (choroiditis), or both
Retinal vasculitis (with whitening or obliteration of blood vessels)
Optic disk edema
Panuveitis may cause any combination of the previously mentioned symptoms and signs.
Complications
Serious complications of uveitis include profound and irreversible vision loss, especially when uveitis is unrecognized, inadequately treated, or both.
The most frequent complications include
Cataract (secondary to the disease process and/or to corticosteroid treatment)
Cystoid macular edema (the most common cause of decreased vision in patients with uveitis)
Glaucoma (secondary to the disease process and/or to corticosteroid treatment)
Band keratopathy (calcium deposition in a band-like pattern across the cornea)
Neovascularization of the retina, optic nerve, or iris
Hypotony (an intraocular pressure that is too low to support the health of the eye)
Symptoms and signs reference
1. Trusko B, Thorne J, Jabs D, et al: Classification criteria for pars planitis. Am J Ophthalmol 228:268-274, 2021. doi: 10.1016/j.ajo.2021.03.045
Diagnosis of Uveitis
Slit-lamp examination
Ophthalmoscopy after pupil dilation
Uveitis should be suspected in any patient who has ocular ache, redness, photophobia, new onset or changing floaters, or decreased vision. Patients with unilateral anterior uveitis have ocular ache in the affected eye if light is shined in the unaffected eye (true photophobia), which is uncommon in conjunctivitis.
Diagnosis of anterior uveitis is by recognizing cells and flare in the anterior chamber. Cells and flare are seen with a slit lamp and are most evident when using a narrow, intensely bright light focused on the anterior chamber in a dark room. Findings of intermediate and posterior uveitis are most easily seen after dilating the pupil. Indirect ophthalmoscopy (usually done by an ophthalmologist) is more sensitive than direct ophthalmoscopy. (NOTE: If uveitis is suspected, patients should be referred immediately for complete ophthalmologic evaluation.)
Many conditions that cause intraocular inflammation can mimic uveitis and should be considered in the appropriate clinical settings. Such conditions include severe conjunctivitis (eg, epidemic keratoconjunctivitis), severe keratitis (eg, herpetic keratoconjunctivitis, peripheral ulcerative keratitis), and severe scleritis.
Acute angle-closure glaucoma can cause redness and severe pain similar to that of uveitis, which is why it is important to check intraocular pressure at every visit. Uveitis is often (but not always) associated with a low intraocular pressure, whereas pressure is typically high in acute angle-closure glaucoma. Uveitis also can be distinguished from angle-closure glaucoma by the absence of corneal haze and the presence of a deeper anterior chamber.
Other masqueraders include intraocular cancers in the very young (typically retinoblastoma and leukemia) and in older adults (intraocular lymphoma). Much less commonly, retinitis pigmentosa can manifest with mild inflammation, which may be confused with uveitis.
Treatment of Uveitis
Corticosteroids (usually topical) and sometimes other immunosuppressive medications
Cycloplegic-mydriatic medications
Sometimes antimicrobial medications
Sometimes surgical therapy
Treatment of active inflammation usually involves corticosteroids given topically (eg, prednisolone acetate 1% one drop as frequently as every hour while awake for severe inflammation) or by periocular or intraocular injection along with a cycloplegic-mydriatic medication (eg, homatropine 2% or 5% drops or cyclopentolate 0.5% or 1.0% drops, either medication given 2 to 4 times/day depending on severity). Corticosteroid implants are available that can treat both active inflammation in the eye as well as uveitic macular edema. They are not associated with systemic symptoms, but they can accelerate cataract formation as well as cause ocular hypertension (Treatment of active inflammation usually involves corticosteroids given topically (eg, prednisolone acetate 1% one drop as frequently as every hour while awake for severe inflammation) or by periocular or intraocular injection along with a cycloplegic-mydriatic medication (eg, homatropine 2% or 5% drops or cyclopentolate 0.5% or 1.0% drops, either medication given 2 to 4 times/day depending on severity). Corticosteroid implants are available that can treat both active inflammation in the eye as well as uveitic macular edema. They are not associated with systemic symptoms, but they can accelerate cataract formation as well as cause ocular hypertension (1). Antimicrobial drugs are used to treat infectious uveitis.
Particularly severe or chronic cases may require systemic corticosteroids or systemic noncorticosteroid immunosuppressive medications. For example,
Prednisone 1 mg/kg orally once/dayPrednisone 1 mg/kg orally once/day
Systemic noncorticosteroid immunosuppressive medications (eg, methotrexate 15 to 25 mg orally once/week; mycophenolate mofetil 500 mg twice daily for 2 weeks, followed by a maintenance dose of 1 to 1.5 g orally twice daily as tolerated; adalimumab, initial dose of 80 mg, followed by 40 mg subcutaneously every 1 to 2 weeks)Systemic noncorticosteroid immunosuppressive medications (eg, methotrexate 15 to 25 mg orally once/week; mycophenolate mofetil 500 mg twice daily for 2 weeks, followed by a maintenance dose of 1 to 1.5 g orally twice daily as tolerated; adalimumab, initial dose of 80 mg, followed by 40 mg subcutaneously every 1 to 2 weeks)
Infliximab 5 to 10 mg/kg IV every 4 weeksInfliximab 5 to 10 mg/kg IV every 4 weeks
Additional treatment for severe or chronic cases may require laser phototherapy, cryotherapy applied transsclerally to the retinal periphery, or surgical removal of the vitreous (vitrectomy) (2–4).
Treatment references
1. Vieira RF, Ferreira A, Menéres P, et al: Efficacy and safety of intravitreal and periocular injection of corticosteroids in noninfectious uveitis: A systematic review. Surv Ophthalmol 67(4):991-1013, 2022. doi: 10.1016/j.survophthal.2021.12.002
2. Jaffe GJ, Dick AD, Brézin AP, et al: Adalimumab in patients with active noninfectious uveitis. : Adalimumab in patients with active noninfectious uveitis.N Engl J Med 375(10):932-943, 2016. doi: 10.1056/NEJMoa1509852
3. Lee J, Koreishi AF, Zumpf KB, et al: Success of weekly adalimumab in refractory ocular inflammatory disease. : Success of weekly adalimumab in refractory ocular inflammatory disease.Ophthalmology S0161-6420(20)30333-X, 2020. doi: 10.1016/j.ophtha.2020.04.009
4. Kruh JN, Yang P, Suelves AM, et al: Infliximab for the treatment of refractory noninfectious uveitis: A study of 88 patients with long-term follow-up. : Infliximab for the treatment of refractory noninfectious uveitis: A study of 88 patients with long-term follow-up.Ophthalmology 121(1):358-364, 2014. doi: 10.1016/j.ophtha.2013.07.019
Key Points
Inflammation of the uveal tract (uveitis) can affect the anterior segment (including the iris), intermediate uveal tract (including the vitreous), or posterior uvea (including the choroid, retina, and optic nerve).
Most cases are idiopathic, but known causes include infections, trauma, and autoimmune disorders.
Findings in acute anterior uveitis include aching eye pain, true photophobia, redness closely surrounding the cornea (ciliary flush), and, on slit-lamp examination, cells and flare.
Chronic anterior uveitis may have less dramatic symptoms and present with eye irritation or decreased vision.
Intermediate and posterior uveitis tend to cause less pain and eye redness but more floaters and decreased vision.
Diagnosis is confirmed by slit-lamp examination and ophthalmoscopic examination (often indirect) after pupillary dilation.
Treatment should be managed by an ophthalmologist and often includes corticosteroids and a cycloplegic-mydriatic medication along with treatment of any specific cause.







