

Herpes simplex viruses (human herpesviruses types 1 and 2) commonly cause recurrent infection affecting the skin, mouth, lips, eyes, and genitals. Common severe infections include encephalitis, meningitis, neonatal herpes, and, in patients who are immunocompromised, disseminated infection. Mucocutaneous infections cause clusters of small painful vesicles on an erythematous base. Diagnosis is primarily clinical; laboratory confirmation by culture, polymerase chain reaction, direct immunofluorescence, or serologic testing can be done. Treatment is symptomatic; antiviral therapy with acyclovir, valacyclovir, or famciclovir is helpful for severe infections and, if begun early, for recurrent or primary infections.
Eight types of herpesviruses infect humans, 2 of which are herpes simplex viruses (HSV). Both types of herpes simplex virus, HSV-1 and HSV-2, can cause oral or genital infection, although either can cause infection in any location. Most often, HSV-1 causes gingivostomatitis, herpes labialis, herpes gladiatorum (which is caused by skin-to-skin contact and is associated with sports such as wrestling and rugby), and herpes keratitis. HSV-2 usually causes genital lesions. (See Overview of Herpesvirus Infections.)
HSV infections are among the most prevalent infections worldwide. In 1 meta-analysis of global pooled data, 67% of the global population aged 0 to 49 (3.75 billion people) were infected with HSV-1 in 2016 (1). Prevalences were identified by detection of type-specific immunoglobulin G antibodies and varied by age, sex, and region. In the same study, incident infections decreased with age, while prevalence accumulated with age due to lifelong infection and seropositivity. In 1 United States–based meta-analysis that evaluated prevalence, the pooled mean seroprevalence was 63.5% among adults and 38% among children in the general population (2).
Transmission of HSV results from close contact with a person who is actively shedding virus. Viral shedding occurs from lesions but can occur even when lesions are not apparent.
After the initial infection, HSV remains dormant in nerve ganglia, from which it can periodically reactivate, causing symptoms. Recurrent herpetic eruptions are precipitated by
Overexposure to sunlight
Febrile illnesses
Physical or emotional stress
Immunosuppression
Hormonal changes (such as those related to menstruation)
Unknown stimuli
Generally, recurrent eruptions are less severe and occur less frequently over time.
General references
1. James C, Harfouche M, Welton NJ, et al. Herpes simplex virus: global infection prevalence and incidence estimates, 2016. Bull World Health Organ. 2020;98(5):315-329. doi:10.2471/BLT.19.237149
2. Ageeb RA, Harfouche M, Chemaitelly H, Abu-Raddad LJ. Epidemiology of herpes simplex virus type 1 in the United States: Systematic review, meta-analyses, and meta-regressions. iScience. 2024;27(9):110652. Published 2024 Aug 5. doi:10.1016/j.isci.2024.110652
Diseases Caused by Herpes Simplex Virus
Diseases include
Mucocutaneous infection (most common), including orofacial and genital herpes
Ocular infection (including herpes keratitis)
Central nervous system (CNS) infection
HSV rarely causes fulminant hepatitis in the absence of cutaneous lesions.
In patients with HIV infection, herpetic infections can be particularly severe. Progressive and persistent esophagitis, colitis, perianal ulcers, pneumonia, encephalitis, and meningitis may occur.
HSV outbreaks may be followed by erythema multiforme, possibly caused by an immune reaction to the virus.
Eczema herpeticum is a complication of HSV infection in which severe herpetic disease develops in skin regions with eczema.
Mucocutaneous herpes simplex infection
Lesions may appear anywhere on the skin or mucosa but are most frequent in the following locations:
Mouth or lips (perioral infection)
Genitals
Conjunctiva and cornea
Generally, after a prodromal period (typically < 24 hours in recurrent HSV-1) of tingling, discomfort, or itching, clusters of small, tense vesicles appear on an erythematous base (1). Clusters vary in size from 0.5 to 1.5 cm but may coalesce. Clustered vesicles are a hallmark of HSV infection and can also occur in varicella zoster (VZV) infection. Lesions on the nose, ears, eyes, fingers, or genitals may be particularly painful.
Vesicles typically persist for a few days, then rupture and dry, forming a thin, yellowish crust.
Healing generally occurs within 2 to 3 weeks after onset in primary infection or within 8 to 10 days in recurrent infection (1). Lesions usually heal completely, but recurrent lesions at the same site may cause atrophy and scarring. Skin lesions can develop secondary bacterial infection. In patients with weakened cell-mediated immunity due to HIV infection or other conditions, prolonged or progressive lesions may persist for weeks or longer. Localized infections can disseminate, particularly—and often dramatically—in patients who are immunocompromised.
Acute herpetic gingivostomatitis usually results from primary infection with HSV-1, typically in children. Herpetic pharyngitis can occur in adults as well as children. Through oral-genital contact, the cause can be either HSV-1 or HSV-2. Intraoral ulceration usually indicates primary infection, while labial lesions without intraoral ulcerations suggest recurrence. Intraoral and gingival vesicles rupture, usually within several hours to 1 or 2 days, to form ulcers (1). Fever and pain often occur. Difficulty eating and drinking may lead to dehydration. After resolution, the virus resides dormant in the trigeminal ganglion.
Herpes labialis typically develops as recurrent ulcers (cold sores) on the vermilion border of the lip or, much less commonly, as ulcerations of the mucosa of the hard palate (in immunocompromised patients).


This photo is a close-up of a herpes simplex virus type 1 (HSV-1) lesion on the lower lip that shows clusters of vesicles on an erythematous base.
CDC


These ulcerative lesions on the soft palate are caused by herpes simplex virus type 1 (HSV-1).
Image courtesy of Robert E. Sumpter via the Public Health Image Library of the Centers for Disease Control and Prevention.
Genital herpes is a common viral sexually transmitted infection that can be caused by HSV-1 or HSV-2.
Herpes simplex keratitis
Herpes simplex keratitis (HSV infection of the corneal epithelium) causes pain, tearing, photophobia, and corneal ulcers that often have a branching pattern.
Herpetic whitlow

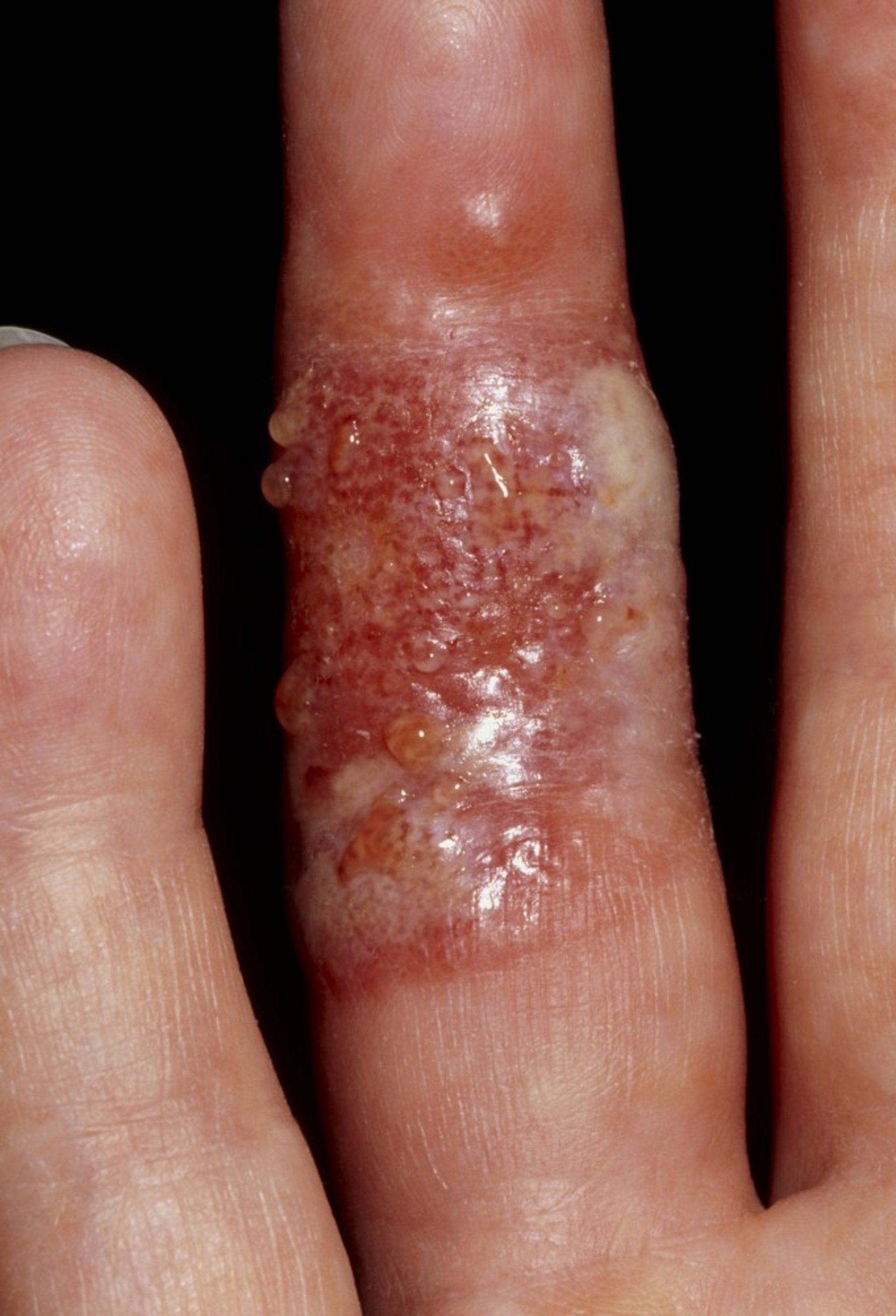
This photo shows blisters (herpetic whitlow) on the fingers of a patient due to herpes simplex virus type 1 (HSV-1) infection.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Herpetic whitlow, a swollen, painful, erythematous lesion of the finger, results from inoculation of HSV through the skin and is most common among health care professionals (eg, dentists). It can also occur with thumb-sucking and nail biting, especially in children (2). The condition is self-limiting, typically resolving clinically in a few weeks.
Herpes simplex CNS infection
Herpes encephalitis occurs sporadically and may be severe. Multiple early seizures are characteristic.
Viral meningitis may result from HSV-2. It is usually self-limited.
Lumbosacral myeloradiculitis, typically caused by HSV-2, can occur during primary infection or reactivation of HSV-2 infection and can result in urinary retention or obstipation.
Neonatal herpes simplex
Neonatal HSV infection develops in neonates, including those whose mothers have no suggestion of current or past herpes infection. It is most commonly transmitted during birth through contact with vaginal secretions containing HSV and can involve HSV-1 or HSV-2.
Neonatal HSV infection usually develops between the first and fourth week of life, causing mucocutaneous vesicles (often due to HSV-1) or central nervous system involvement (often due to HSV-2) (3). It causes major morbidity and mortality.
Etiology of herpes simplex virus references
1. Whitley RJ, Roizman B. Herpes simplex virus infections. Lancet. 2001;357(9267):1513-1518. doi:10.1016/S0140-6736(00)04638-9
2. Szinnai G, Schaad UB, Heininger U. Multiple herpetic whitlow lesions in a 4-year-old girl: case report and review of the literature. Eur J Pediatr. 2001;160(9):528-533. doi:10.1007/s004310100800
3. Kropp RY, Wong T, Cormier L, et al. Neonatal herpes simplex virus infections in Canada: results of a 3-year national prospective study. Pediatrics. 2006;117(6):1955-1962. doi:10.1542/peds.2005-1778
Diagnosis of Herpes Simplex Virus
Primarily history and physical examination
Sometimes laboratory confirmation
Polymerase chain reaction (PCR) of cerebrospinal fluid (CSF) and MRI for HSV encephalitis
The diagnosis of HSV infection is often clinical, based on the presence of characteristic lesions (1).
Clusters of vesicles or ulcers on an erythematous base are unusual in genital ulcers other than those due to HSV infection.
Laboratory confirmation can be helpful, especially if infection is severe, the patient is immunocompromised or pregnant, or lesions are atypical. A Tzanck test (a superficial scraping from the base of a freshly ruptured vesicle stained with Wright-Giemsa stain) can be done and often reveals multinucleate giant cells in HSV or VZV infection; however, it is limited by low sensitivity.
Definitive diagnosis is with culture, PCR, and antigen detection. Fluid and material should be obtained from the base of a vesicle or of a freshly ulcerated lesion. Nucleic acid amplification tests (NAATs), such as PCR performed on a swab from the lesion base, are the most sensitive and specific diagnostic method. In regions where it is available, PCR is considered the gold standard for detecting HSV DNA in skin, mucosa, blood, or CSF with generally higher sensitivity than cultures (2, 3). HSV can sometimes be identified using direct immunofluorescence assay of scrapings of lesions. Viral culture and direct immunofluorescence assays testing are less sensitive, especially for older or healing lesions. Routine serology is not recommended for acute diagnosis but can help determine prior exposure.
PCR of CSF and MRI are especially useful in the diagnosis of HSV encephalitis.
HSV should be distinguished from herpes zoster, which rarely recurs and usually causes more severe pain and larger groups of lesions that are distributed along a dermatome and typically do not cross the midline.
If herpes infections recur frequently, do not resolve, or do not respond to antivirals as expected, immunocompromise, possibly due to HIV infection, should be suspected.
(See also Diagnosis of Genital Herpes).
Diagnosis references
1. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-e52. doi:10.1093/cid/ciu444
2. Dominguez SR, Pretty K, Hengartner R, Robinson CC. Comparison of Herpes Simplex Virus PCR with Culture for Virus Detection in Multisource Surface Swab Specimens from Neonates. J Clin Microbiol. 2018;56(10):e00632-18. Published 2018 Sep 25. doi:10.1128/JCM.00632-18
3. Aliabadi N, Jamalidoust M, Asaei S, Namayandeh M, Ziyaeyan M. Diagnosing of herpes simplex virus infections in suspected patients using real-time PCR. Jundishapur J Microbiol. 2015;8(2):e16727. Published 2015 Feb 20. doi:10.5812/jjm.16727
Treatment of Herpes Simplex Virus
Usually acyclovir, valacyclovir, or famciclovirUsually acyclovir, valacyclovir, or famciclovir
Sometimes topical acyclovir, penciclovir, or docosanol Sometimes topical acyclovir, penciclovir, or docosanol
For keratitis, topical trifluridine (typically in consultation with an ophthalmologist)For keratitis, topical trifluridine (typically in consultation with an ophthalmologist)
For infections in immunocompromised patients, CNS infections, or neonatal herpes, IV acyclovirFor infections in immunocompromised patients, CNS infections, or neonatal herpes, IV acyclovir
The treatment for mucocutaneous infection involves both topical and systemic antiviral therapies, with the choice guided by severity of infection, patient risk factors (eg, immunocompromise), and lesion location. Treating primary HSV infection with medications, even if done early, does not prevent the possibility of recurrence (because of the capacity for HSV to remain latent or dormant) (1).
Mucocutaneous herpes simplex infection
Isolated cutaneous infections in immunocompetent people can often go untreated without consequence.
For immunocompetent patients with recurrent, mild localized lesions (1), topical agents such as acyclovir cream (applied 5 times daily for 4 days) can reduce duration of lesions and local symptoms if initiated early, but oral antivirals are generally at least as effective and are administered less frequently. For primary mucocutaneous infection, oral antivirals such as acyclovir, valacyclovir, or famciclovir can be used for therapy.), topical agents such as acyclovir cream (applied 5 times daily for 4 days) can reduce duration of lesions and local symptoms if initiated early, but oral antivirals are generally at least as effective and are administered less frequently. For primary mucocutaneous infection, oral antivirals such as acyclovir, valacyclovir, or famciclovir can be used for therapy.
Gingivostomatitis and pharyngitis may additionally require symptom relief with topical anesthetics (eg, dyclonine, benzocaine, viscous lidocaine). (NOTE: Lidocaine must not be swallowed because it anesthetizes the oropharynx, the hypopharynx, and possibly the epiglottis. Children must be watched for signs of aspiration.) Severe cases can be treated with oral acyclovir, valacyclovir, or famciclovir.may additionally require symptom relief with topical anesthetics (eg, dyclonine, benzocaine, viscous lidocaine). (NOTE: Lidocaine must not be swallowed because it anesthetizes the oropharynx, the hypopharynx, and possibly the epiglottis. Children must be watched for signs of aspiration.) Severe cases can be treated with oral acyclovir, valacyclovir, or famciclovir.
Herpes labialis responds to oral and topical acyclovir or topical penciclovir. For milder lesions, the duration of a recurrent eruption may be decreased by almost a day by applying penciclovir 1% cream every 2 hours while awake for 4 days, beginning during the prodrome or when the first lesion appears. Docosanol 10% cream may be effective when used 5 times a day. Docosanol is an alcohol that inhibits virus fusion with the host cell. Toxicity appears to be minimal. responds to oral and topical acyclovir or topical penciclovir. For milder lesions, the duration of a recurrent eruption may be decreased by almost a day by applying penciclovir 1% cream every 2 hours while awake for 4 days, beginning during the prodrome or when the first lesion appears. Docosanol 10% cream may be effective when used 5 times a day. Docosanol is an alcohol that inhibits virus fusion with the host cell. Toxicity appears to be minimal.
For recurrent or severe herpes labialis, famciclovir 1500 mg as 1 dose or valacyclovir 2 g orally every 12 hours for 1 day can be used. Oral therapy with antivirals (acyclovir, famciclovir, or valacyclovir) can speed resolution of lesions (For recurrent or severe herpes labialis, famciclovir 1500 mg as 1 dose or valacyclovir 2 g orally every 12 hours for 1 day can be used. Oral therapy with antivirals (acyclovir, famciclovir, or valacyclovir) can speed resolution of lesions (2).
Herpetic whitlow heals in 2 to 3 weeks without treatment. Topical acyclovir has not been shown to be effective. Oral or IV acyclovir can be used in immunosuppressed patients and those with severe infection.heals in 2 to 3 weeks without treatment. Topical acyclovir has not been shown to be effective. Oral or IV acyclovir can be used in immunosuppressed patients and those with severe infection.
Secondary bacterial infections are treated with topical antibiotics (eg, mupirocin) or, if severe, with systemic antibiotics (eg, penicillinase-resistant beta-lactams) (Secondary bacterial infections are treated with topical antibiotics (eg, mupirocin) or, if severe, with systemic antibiotics (eg, penicillinase-resistant beta-lactams) (1). Systemic analgesics may help reduce inflammation and associated pain.
Infection with acyclovir-resistant HSV is rare and occurs almost exclusively in patients who are immunocompromised. Acyclovir-resistant strains are resistant to penciclovir, famciclovir, and valacyclovir. Foscarnet may be effective for acyclovir-resistant infections.Infection with acyclovir-resistant HSV is rare and occurs almost exclusively in patients who are immunocompromised. Acyclovir-resistant strains are resistant to penciclovir, famciclovir, and valacyclovir. Foscarnet may be effective for acyclovir-resistant infections.
For some immunocompromised patients or those with severe, extensive, or disseminated disease, intravenous acyclovir is the standard initial therapy, which, depending on severity, can sometimes be followed by oral antivirals once lesions begin to regress, continuing until healing is complete (For some immunocompromised patients or those with severe, extensive, or disseminated disease, intravenous acyclovir is the standard initial therapy, which, depending on severity, can sometimes be followed by oral antivirals once lesions begin to regress, continuing until healing is complete (3).
(See also Diagnosis of Genital Herpes).
Pearls & Pitfalls
|
Herpes simplex keratitis
Treatment of herpes simplex keratitis involves topical antivirals, such as trifluridine, and should be supervised by an ophthalmologist.involves topical antivirals, such as trifluridine, and should be supervised by an ophthalmologist.
Neonatal herpes simplex
IV acyclovir should be used for therapy. (See also IV acyclovir should be used for therapy. (See alsoTreatment of Neonatal HSV Infection .)
Herpes simplex CNS infection
Encephalitis is treated with IV acyclovir. Treatment for 14 to 21 days is preferred to prevent potential relapse (Encephalitis is treated with IV acyclovir. Treatment for 14 to 21 days is preferred to prevent potential relapse (4).
Viral meningitis is usually treated with IV acyclovir (Viral meningitis is usually treated with IV acyclovir (5). Acyclovir is generally very well tolerated. However, adverse effects can include phlebitis, renal dysfunction, and, rarely, neurotoxicity (lethargy, confusion, seizures, coma; usually in the setting of renal insufficiency).). Acyclovir is generally very well tolerated. However, adverse effects can include phlebitis, renal dysfunction, and, rarely, neurotoxicity (lethargy, confusion, seizures, coma; usually in the setting of renal insufficiency).
Treatment references
1. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-e52. doi:10.1093/cid/ciu444
2. Mancini A, Inchingolo AM, Marinelli G, et al. Topical and Systemic Therapeutic Approaches in the Treatment of Oral Herpes Simplex Virus Infection: A Systematic Review. Int J Mol Sci. 2025;26(17):8490. Published 2025 Sep 1. doi:10.3390/ijms26178490
3. Balfour HH Jr. Antiviral drugs. N Engl J Med. 1999;340(16):1255-1268. doi:10.1056/NEJM199904223401608
4. Sili U, Kaya A, Mert A; HSV Encephalitis Study Group. Herpes simplex virus encephalitis: clinical manifestations, diagnosis and outcome in 106 adult patients. J Clin Virol. 2014;60(2):112-118. doi:10.1016/j.jcv.2014.03.010
5. Noska A, Kyrillos R, Hansen G, Hirigoyen D, Williams DN. The role of antiviral therapy in immunocompromised patients with herpes simplex virus meningitis. Clin Infect Dis. 2015;60(2):237-242. doi:10.1093/cid/ciu772
Key Points
HSV usually causes mucocutaneous infection but sometimes causes keratitis, and serious CNS infection can occur in neonates and in adults.
After initial infection, HSV remains dormant in nerve ganglia, from which it can periodically reactivate, causing symptoms.
Diagnose mucocutaneous infections clinically, but do viral culture, PCR, or antigen detection if patients are neonates, immunocompromised, or pregnant or have a CNS infection or severe disease.
For mucocutaneous infections, consider oral acyclovir, valacyclovir, or famciclovir; for herpes labialis, an alternative is topical penciclovir or docosanol.For mucocutaneous infections, consider oral acyclovir, valacyclovir, or famciclovir; for herpes labialis, an alternative is topical penciclovir or docosanol.
Give IV acyclovir to patients with serious infections.Give IV acyclovir to patients with serious infections.
Drug Information for the Topic





