



Hypertensive arteriolar nephrosclerosis is a progressive kidney disease caused by chronic, poorly controlled hypertension. Symptoms and signs of chronic kidney disease may develop (eg, anorexia, nausea, vomiting, pruritus, somnolence or confusion), as may signs of end-organ damage secondary to hypertension. Diagnosis is primarily clinical, supported by ultrasound and routine laboratory test findings. Treatment is strict blood pressure control and support of kidney function.
Topic Resources

Hypertensive arteriolar nephrosclerosis results when chronic hypertension damages small blood vessels, glomeruli, and tubulointerstitial tissues. As a result, progressive chronic kidney disease develops.
Hypertensive arteriolar nephrosclerosis progresses to kidney failure (formerly called end-stage renal disease) (1) in only a small percentage of patients. However, because chronic hypertension and hypertensive nephrosclerosis are common, hypertensive arteriolar nephrosclerosis is one of the most common diagnoses in patients with kidney failure. It is often described as benign to distinguish it from malignant arteriolar nephrosclerosis, which is rapidly progressed to end organ damage.
Risk factors include
Older age
Poorly controlled hypertension
Other kidney disorders (eg, diabetic nephropathy)
Black people are at increased risk; it is unclear if the risk is increased because poorly treated hypertension is more common among Black people or because they are more genetically susceptible to hypertension-induced kidney damage (2).
General references
1. Levey AS, Eckardt KU, Dorman NM, et al: Nomenclature for kidney function and disease: Executive summary and glossary from a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Res Clin Pract 39(2):151–161, 2020. doi:10.23876/j.krcp.20.393
2. Rahman M, Douglas JG, Wright JT Jr. Pathophysiology and treatment implications of hypertension in the African-American population. Endocrinol Metab Clin North Am 1997;26(1):125-144. doi:10.1016/s0889-8529(05)70237-1
Symptoms and Signs of Hypertensive Arteriolar Nephrosclerosis
Symptoms and signs of chronic kidney disease, such as anorexia, nausea, vomiting, pruritus, somnolence or confusion, weight loss, and an unpleasant taste in the mouth, may develop. Signs of hypertension-related end-organ damage may occur in the vasculature of the eyes and in the skin, central nervous system, and periphery.
Diagnosis of Hypertensive Arteriolar Nephrosclerosis
History of hypertension
Blood tests indicating kidney failure
Signs of hypertensive end-organ damage
No other cause of chronic kidney disease
The diagnosis may be suspected when routine blood tests indicate deteriorating kidney function (eg, elevated creatinine and blood urea nitrogen [BUN], hyperphosphatemia) in a patient with hypertension. Diagnosis is usually inferred because of the history and evidence of hypertension-related end-organ damage (eg, retinal changes, left ventricular hypertrophy) on physical examination. Hypertension should be present before onset of proteinuria and kidney failure, and there should be no other clinically suspected cause of kidney failure.
Urine testing should not suggest other causes of kidney failure (eg, glomerulonephritis, hypertensive emergency). On urinalysis, there should be few cells or casts in the sediment, and protein excretion is usually < 1 g/day (it is occasionally higher and in the nephrotic range).

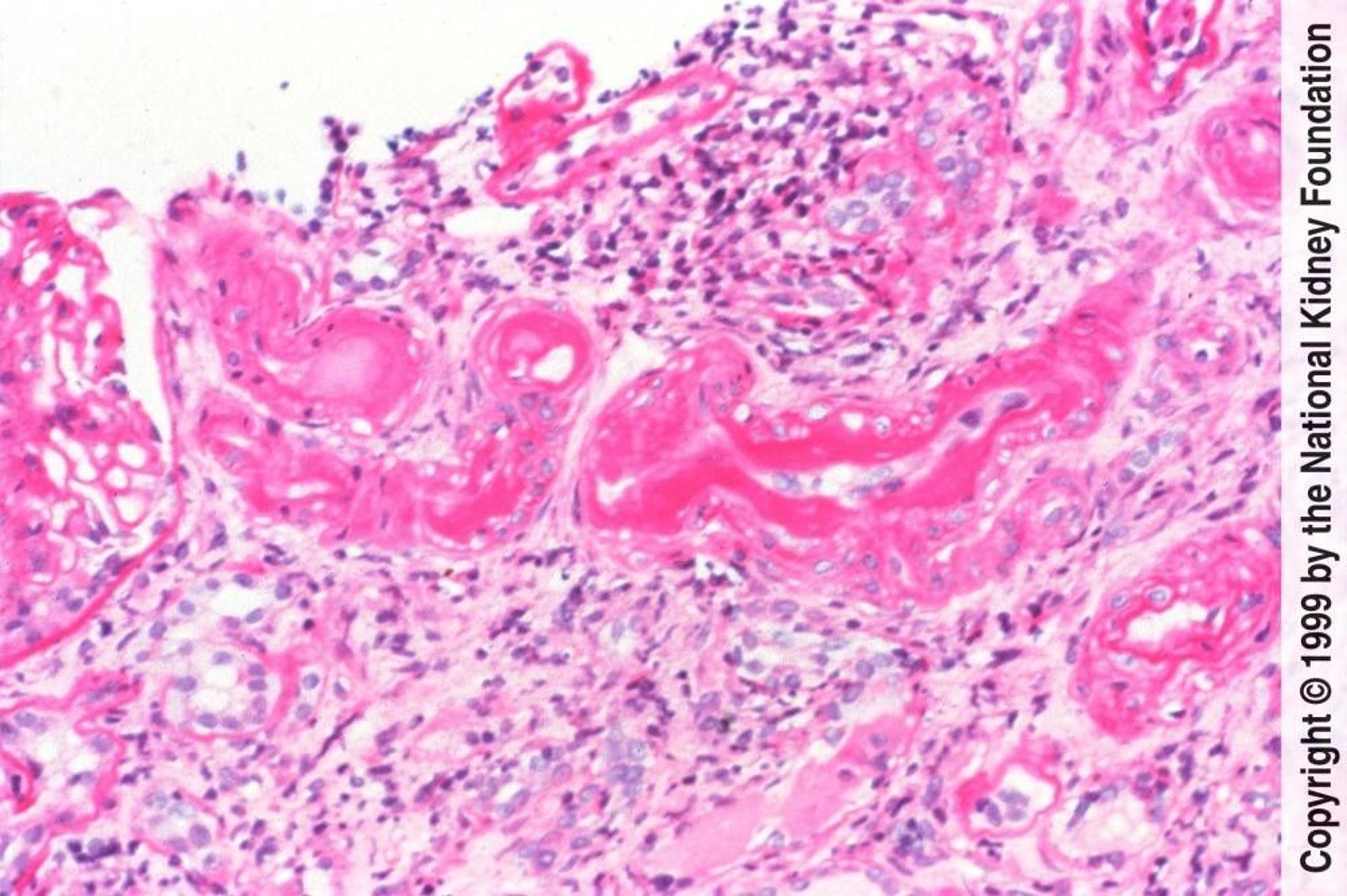
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Ultrasound should be done to exclude other causes of kidney failure. It may show that kidney size is reduced. Renal biopsy is done only if the diagnosis remains unclear.
Treatment of Hypertensive Arteriolar Nephrosclerosis
Antihypertensive medications
Treatment involves strict blood pressure control, with antihypertensives when necessary. The current recommendation of blood pressure goal is 120 to 130/< 80 mm Hg for most patients (1, 2). Most experts suggest using an angiotensin II receptor blocker (ARB) or an angiotensin-converting enzyme (ACE) inhibitor for patients who have proteinuria. Calcium channel blockers and thiazide diuretics can also be used as first-line medications; most patients require combination therapy for blood pressure control. Weight loss, exercise, and salt and water restriction also help control blood pressure. Chronic kidney disease should be managed as appropriate.
Treatment references
1. Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group: KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int 99(3S):S1-S87, 2021. doi: 10.1016/j.kint.2020.11.003
2. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018;138(17):e484-e594. doi:10.1161/CIR.0000000000000596
Prognosis for Hypertensive Arteriolar Nephrosclerosis
Prognosis usually depends on adequacy of blood pressure control and degree of kidney failure.
Key Points
Chronic hypertension can cause hypertensive arteriolar nephrosclerosis, resulting in chronic kidney disease and, infrequently, kidney failure.
Suspect the diagnosis if chronic hypertension precedes onset of chronic kidney disease.
Perform ultrasound to check for other causes of kidney failure.
Treat most patients with an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker, and possibly other medications, to control medications.







