


- How To Cleanse, Irrigate, Debride, and Dress Wounds
- How To Repair a Laceration With Simple Interrupted Sutures
- How To Do Plastic Surgical Repair With Buried Deep Dermal Sutures
- How To Repair a Laceration With Glue
- How To Repair a Laceration With Horizontal Mattress Sutures
- How To Repair a Laceration With Stapling
- How To Repair a Laceration With a Subcuticular Running Suture
- How To Repair a Laceration With Vertical Mattress Sutures
Placed intradermally, the subcuticular running-type suture is used for cosmetic closure of a straight, clean laceration under no tension, typically of the face or neck and using absorbable suture.
Topic Resources

Indications for Subcuticular Running Sutures
There are several indications for using subcuticular sutures:
Cosmetic wound closure, for clean, straight lacerations ≤ 6 cm long and under no tension
Patients prone to keloid formation
Problematic suture removal (eg, wounds beneath casts)
Young children (who may be frightened and unable to cooperate with suture removal and in whom scar formation with percutaneous sutures is more likely than in older patients)
Patients unlikely to follow up on time for suture removal
Contraindications to Subcuticular Running Sutures
Absolute contraindications
None
Relative contraindications
Wounds that are irregular or have ragged edges
Wounds under marked tension
Wounds > 6 cm in length
Sometimes, excision and undermining techniques can render a ragged wound suitable for continuous subcuticular closure. However, generalists may prefer to not modify an irregular wound but, rather, close it using simple interrupted sutures, which often provides an aesthetically acceptable result and preserves more tissue for a future cosmetic revision, if needed.
Sutures of any type may be contraindicated for wounds that are contaminated, relatively old, or that would be at higher risk of infection if closed by sutures, such as small bites to hands or feet, puncture wounds, or high-velocity missile wounds.
Wounds involving deep structures (eg, nerves, blood vessels, ducts, joints, tendons, bones) may require specialized techniques or referral to a surgical specialist, as should those covering large areas or involving the face or hands.
Complications of Subcuticular Running Sutures
Wound dehiscence, infection, fibrosis
Equipment for Subcuticular Running Sutures
Wound hygiene and closure techniques need not be sterile procedures. Although instruments that touch the wound (eg, forceps, needles, suture) must be sterile, clean nonsterile gloves as well as clean but not sterile water may be used in immunocompetent patients. Some operators prefer the better fit and better barrier protection of sterile gloves.
Clean procedure, barrier protection
Face mask and safety glasses (or a face shield), head caps, gowns, gloves
Sterile drapes, towels (for wound debridement and suturing)
Antiseptic solution such as chlorhexidine or povidone-iodineAntiseptic solution such as chlorhexidine or povidone-iodine
A standard suture tray including local anesthesia
4-0 or 5-0 suture: absorbable (eg, polyglycolic acid, polydioxanone [PDS], polyglactin) or nonabsorbable monofilament (eg, nylon or polypropylene)
Nonocclusive dressing
Antibiotic ointment
Additional Considerations for Subcuticular Running Sutures
Buried dermal sutures (deep dermal sutures) may be necessary for dermal and subcutaneous apposition in deeper wounds before placing a continuous subcuticular suture.
The absorbable synthetic monofilament suture polydioxanone [PDS] is designed for subcuticular closure and may pass through tissues as easily as nonabsorbable monofilament sutures.
Absorbable subcuticular sutures do not appear to provoke more inflammation than monofilament nylon (nonabsorbable) percutaneous running sutures.
Relevant Anatomy for Subcuticular Running Sutures
The subcutis or hypodermis refers to the subcutaneous layer of tissue lying beneath the dermal layer. However, subcuticular sutures are placed intradermally. The epidermis and dermis are grossly indistinguishable, and intradermal sutures are typically placed 1 to 2 mm deep to the skin surface. The upper subcutis may be distinguished from the dermis by the decreased resistance to needle insertion in the loose subcutaneous tissue.
Minimizing tension on the epidermal layer (and aligning and everting the wound edges) are key to achieving the best wound result.
Consider whether lacerations are subject to dynamic skin tension before closure (see figure Representative Minimal Skin Tension Lines).
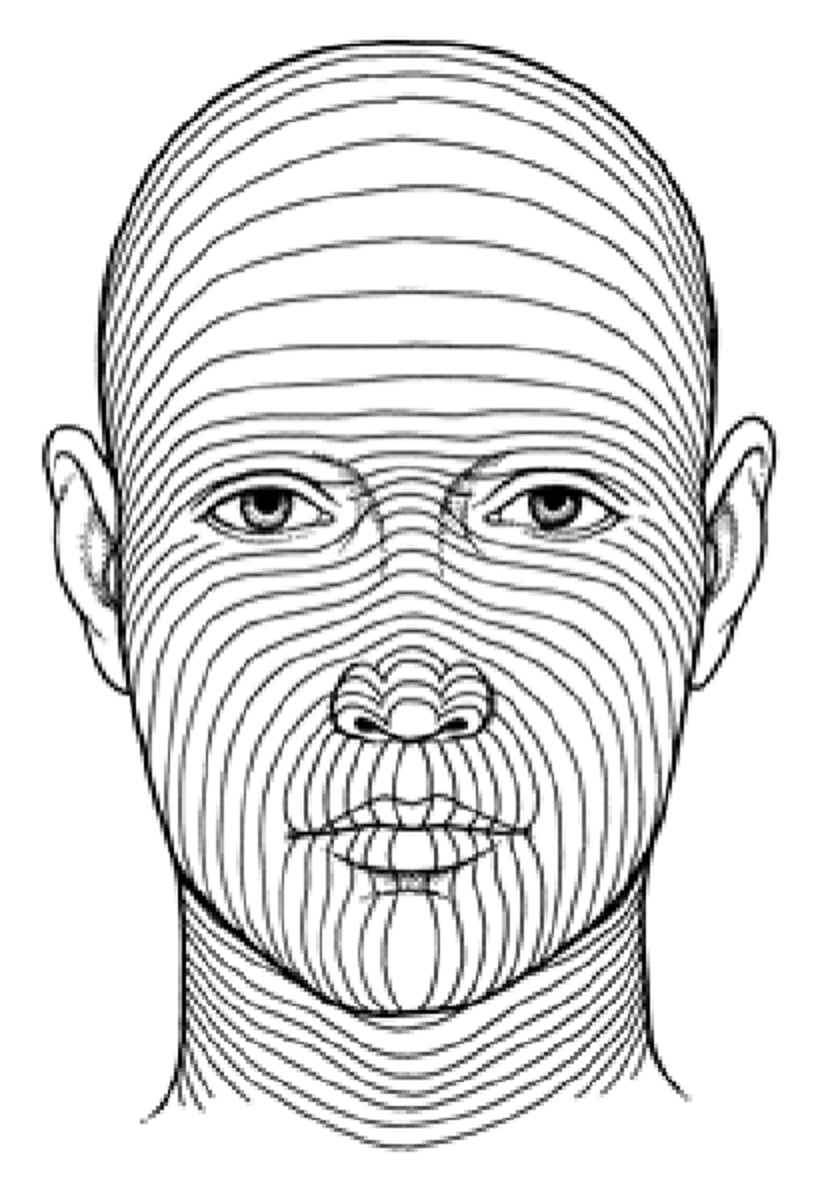
Representative Minimal Skin Tension Lines
Direction of force is along each line. Cuts perpendicular to these lines are thus under greatest tension and most likely to widen. |

Positioning for Subcuticular Running Sutures
Position the patient comfortably reclined or supine.
Adjust the stretcher height so that you will be comfortable either sitting or standing at the bedside.
The laceration should be well lit, preferably with an overhead procedure light.
Step-by-Step Description of Subcuticular Running Sutures
(See How To Cleanse, Irrigate, Debride, and Dress Wounds for step-by-step descriptions of wound preparation, anesthesia, and dressing; see How To Repair a Laceration With Simple Interrupted Sutures for instructions on how to handle the instruments, work with needles, and tie a surgeon's knot using instruments.)
Cleanse, anesthetize, irrigate, and debride the wound as necessary.
Place a sterile fenestrated drape over the wound. Place additional drapes nearby as needed to provide a large enough sterile work area.
Approximate the subcutaneous layer as necessary, using interrupted sutures (eg, buried intradermal [deep dermal] sutures).
For closures that will require suture removal
Place a dermal or subcutaneous suture about 1 to 2 cm away from one end of the wound and secure it with a knot. Use the needle attached to the suture to place the subcuticular sutures.
Place subcuticular sutures 1 to 2 mm deep to the skin surface.
Take similar-sized and small bites horizontally, alternating between sides of the wound and on the same plane for the full length of the laceration. Place each successive bite about 1 to 2 mm behind the exit point from the opposite side of the wound so that when the wound is closed, the entrance and exit points on either side are not directly apposed.
Pull the suture taut and tie a knot with a tail and a loop of suture about 1 to 2 cm from the end of the wound.
If needed to precisely align the laceration’s edges, place a fine (eg, 6-0) running skin suture on the surface, in addition to the subcuticular suture. At one end of the laceration tie a simple suture with a knot but leave the needle and suture attached. Evert the skin edges along the length of the laceration if possible. Advance the needle, taking small bites at a 45-degree angle to the long axis of the laceration (perpendicular to the skin) for the complete length of the laceration. After the final bite, extend a loop of suture from the wound and use this loop as one end of the suture for the final tie.
For closures that will not require suture removal
Place and secure a dermal or subcuticular suture at one end of the laceration with a knot.
Place subcuticular sutures as described above from one end of the laceration to the other.
Pull the sutures taut, then tie a knot with a tail and loop of suture.
Bury this final knot by inserting the needle into deeper tissue and exit with the needle several millimeters from the edge of the wound. Pull on the end of the needle so the knot disappears into the wound.
Aftercare for Subcuticular Running Sutures
Dress the wound (see Lacerations and How To Cleanse, Irrigate, Debride, and Dress Wounds).
Splint joints whose movement will cause wound tension (eg, an elbow splint for a dorsal elbow laceration).
Instruct the patient to keep the dressing dry and in place and to return in 2 days for a wound check.
Instruct the patient to return if signs of infection develop (eg, increased pain, swelling, redness, fever, proximally spreading red streaks [infectious lymphangiitis]).
Instruct the patient when to return for suture removal, which is generally based on the wound site: 3 to 5 days for the face, 6 to 10 days for the scalp and trunk, 10 to 14 days for the arms and legs, and 14 days for wounds overlying joints. Early suture removal risks wound dehiscence; however, to decrease scarring and cross-hatching of facial sutures, half of the suture line (ie, every other suture) may be removed on day 3 and the remainder are removed on day 5.
Tips and Tricks for Subcuticular Running Sutures
If the subcuticular technique is used exclusively to approximate the skin surface, apply skin tape (or apply surface sutures) to correct surface unevenness and to provide more accurate apposition of the epidermis.







