



Rheumatoid arthritis is a chronic systemic autoimmune disease that primarily involves the joints. Rheumatoid arthritis causes damage mediated by cytokines, chemokines, and metalloproteases. Characteristically, peripheral joints (eg, wrists, metacarpophalangeal joints) are symmetrically inflamed, leading to progressive destruction of articular structures, usually accompanied by systemic symptoms. Diagnosis is based on specific clinical, laboratory, and imaging features. Treatment involves disease-modifying antirheumatic drugs (DMARDs), physical measures, and sometimes surgery. DMARDs can reduce symptoms and slow disease progression.
Topic Resources







")
")



Rheumatoid arthritis affects approximately 0.5% of the population (1). Women are affected 2 to 3 times more often than men (2). Onset may be at any age, most often between 35 years and 50 years, but can be during childhood (see Juvenile Idiopathic Arthritis) or old age.
General references
1. Almutairi KB, Nossent JC, Preen DB, Keen HI, Inderjeeth CA: The prevalence of rheumatoid arthritis: a systematic review of population-based studies. J Rheumatol 48(5):669-676, 2021. doi:10.3899/jrheum.200367
2. Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE: Is the incidence of rheumatoid arthritis rising?: results from Olmsted County, Minnesota, 1955-2007. Arthritis Rheum. 2010;62(6):1576-1582. doi:10.1002/art.27425
Etiology of Rheumatoid Arthritis
Although rheumatoid arthritis involves autoimmune reactions, the precise cause is unknown; many factors may contribute. A genetic predisposition has been identified and, in White populations, localized to a shared epitope in the HLA-DRB1 locus of class II histocompatibility antigens (1). Unknown or unconfirmed environmental factors (eg, viral infections, cigarette smoking) are thought to play a role in triggering and maintaining joint inflammation.
Risk factors for rheumatoid arthritis include the following:
Smoking
Obesity
Sex hormones
Medications (eg, immune checkpoint inhibitors)
Changes in microbiome of the gut, mouth, and lung (2)
Periodontal disease (periodontitis) (3)
Etiology references
1. Dedmon LE: The genetics of rheumatoid arthritis. Rheumatology (Oxford) 59(10):2661-2670, 2020. doi:10.1093/rheumatology/keaa232
2. Block KE, Zheng Z, Dent AL, et al: Gut microbiota regulates K/BxN autoimmune arthritis through follicular helper T but not Th17 cells. J Immunol 196(4):1550-7, 2016. doi: 10.4049/jimmunol.1501904
3. Wegner N, Wait R, Sroka A, et al: Peptidylarginine deiminase from Porphyromonas gingivalis citrullinates human fibrinogen and α-enolase: implications for autoimmunity in rheumatoid arthritis. Arthritis Rheum 62(9):2662-72, 2010. doi: 10.1002/art.27552
Pathophysiology of Rheumatoid Arthritis
Prominent immunologic abnormalities include immune complexes produced by synovial lining cells and in inflamed blood vessels. Plasma cells produce antibodies (eg, rheumatoid factor [RF], anticyclic citrullinated peptide [anti-CCP] antibody) that contribute to these complexes, but destructive arthritis can occur in their absence. Macrophages also migrate to diseased synovium in early disease; increased macrophage-derived lining cells are prominent along with vessel inflammation. Lymphocytes that infiltrate the synovial tissue are primarily CD4+ T cells. Macrophages and lymphocytes produce pro-inflammatory cytokines and chemokines (eg, tumor necrosis factor [TNF]-alpha, granulocyte-macrophage colony-stimulating factor [GM-CSF], various interleukins, interferon-gamma) in the synovium. Released inflammatory mediators and various enzymes contribute to the systemic and joint manifestations of rheumatoid arthritis, including cartilage and bone destruction (1).
In seropositive rheumatoid arthritis, accumulating evidence suggests that anti-CCP antibodies appear long before any signs of inflammation (2). Additionally, anti-carbamylated protein (anti-CarP) antibodies (3) predict more radiologic progression in anti-CCP–negative rheumatoid arthritis patients. Progression to rheumatoid arthritis in the preclinical phase depends on autoantibody epitope spreading in which there are immune responses to released self-antigens with subsequent increased inflammation (4).
In chronically affected joints, the normally thin synovium proliferates, thickens, and develops many villous folds. The synovial lining cells produce various materials, including collagenase and stromelysin, which contribute to cartilage destruction, and interleukin-1 (IL-1) and TNF-alpha, which stimulate cartilage destruction, osteoclast-mediated bone absorption, synovial inflammation, and prostaglandins (which potentiate inflammation). Fibrin deposition, fibrosis, and necrosis are also present. Hyperplastic synovial tissue (pannus) invades local structures and releases inflammatory mediators, which erode cartilage, subchondral bone, articular capsule, and ligaments. Polymorphonuclear leukocytes on average make up approximately 60% of white blood cells in the synovial fluid.In chronically affected joints, the normally thin synovium proliferates, thickens, and develops many villous folds. The synovial lining cells produce various materials, including collagenase and stromelysin, which contribute to cartilage destruction, and interleukin-1 (IL-1) and TNF-alpha, which stimulate cartilage destruction, osteoclast-mediated bone absorption, synovial inflammation, and prostaglandins (which potentiate inflammation). Fibrin deposition, fibrosis, and necrosis are also present. Hyperplastic synovial tissue (pannus) invades local structures and releases inflammatory mediators, which erode cartilage, subchondral bone, articular capsule, and ligaments. Polymorphonuclear leukocytes on average make up approximately 60% of white blood cells in the synovial fluid.
Subcutaneous rheumatoid nodules develop in up to 30% of patients with rheumatoid arthritis, although the prevalence appears to be declining (5). They are granulomas consisting of a central necrotic area surrounded by palisaded histiocytic macrophages, all enveloped by lymphocytes, plasma cells, and fibroblasts. Nodules can also develop in visceral organs such as lungs.
Pathophysiology references
1. Gravallese EM, Firestein GS: Rheumatoid Arthritis - Common Origins, Divergent Mechanisms. N Engl J Med 388(6):529-542, 2023. doi:10.1056/NEJMra2103726
2. Rantapaa-Dahlqvist S, de Jong BA, Berglin E, et al: Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheum 48:2741–2749, 2003. doi: 10.1002/art.11223
3. Brink M, Verheul MK, Rönnelid J, et al: Anti-carbamylated protein antibodies in the pre-symptomatic phase of rheumatoid arthritis, their relationship with multiple anti-citrulline peptide antibodies and association with radiological damage. Arthritis Res Ther 17:25, 2015. doi: 10.1186/s13075-015-0536-2
4. Sokolove J, Bromberg R, Deane KD, et al: Autoantibody epitope spreading in the pre-clinical phase predicts progression to rheumatoid arthritis. PLoS ONE 7(5):e35296, 2012. doi: 10.1371/journal.pone.0035296
5. Kimbrough BA, Crowson CS, Davis JM 3rd, et al: Decline in Incidence of Extra-Articular Manifestations of Rheumatoid Arthritis: A Population-Based Cohort Study. Arthritis Care Res (Hoboken). Published online September 10, 2023. doi:10.1002/acr.25231
Symptoms and Signs of Rheumatoid Arthritis
Onset of rheumatoid arthritis is usually insidious, often beginning with systemic and joint symptoms. Systemic symptoms include afternoon fatigue and malaise, anorexia, generalized weakness, and occasionally low-grade fever. Joint symptoms include pain, swelling, and stiffness. Occasionally, the disease begins abruptly, mimicking an acute viral syndrome.
The disease progression and development of structural damage vary. The course is unpredictable in individual patients.
Joint symptoms are characteristically symmetric. Typically, stiffness lasts > 60 minutes after rising in the morning but may occur after any prolonged inactivity (called gelling). Involved joints become tender and swollen, occasionally with erythema, warmth, and limitation of motion. The joints primarily involved include the following:
Wrists and the index (2nd) and middle (3rd) metacarpophalangeal joints (most commonly involved)
Proximal interphalangeal joints
Metatarsophalangeal joints
Shoulders
Elbows
Hips
Knees
Ankles
However, virtually any joint, except the distal interphalangeal (DIP) joints, may be involved. Different patterns of disease presentation include
Monoarthritis of knee, wrist, shoulder, or ankle
Polymyalgia rheumatica–like presentation predominantly with shoulder and hip girdle involvement, especially in older adults
Palindromic rheumatism, characterized by recurrent attacks of arthritis of one to several joints, lasting for hours to days
Joint swelling without chronic joint damage
Robustus rheumatoid arthritis with proliferative and damaging synovitis, but minimal pain
Lower spine involvement is not characteristic of rheumatoid arthritis, but cervical spine inflammation can result in instability, which can become an emergency.
In peripheral joints, synovial thickening and swelling are often detectable. Joints are often held in flexion to minimize pain, which results from joint capsular distention.
Fixed deformities, particularly flexion contractures, may develop rapidly; ulnar deviation of the fingers with an ulnar slippage of the extensor tendons off the metacarpophalangeal joints is typical, as are swan-neck deformities and boutonnière deformities. Joint instability due to stretching of the joint capsule can also occur. Carpal tunnel syndrome can result from wrist synovitis compressing the median nerve. Popliteal (Baker) cysts can develop, causing calf swelling and tenderness suggestive of deep venous thrombosis.
Cervical spine involvement is common in longstanding active disease and usually presents as pain and stiffness, sometimes with radicular pain or features of myelopathy with hyperreflexia and occipital headache.
Cricoarytenoid joint arthritis can manifest as voice hoarseness and respiratory stridor.


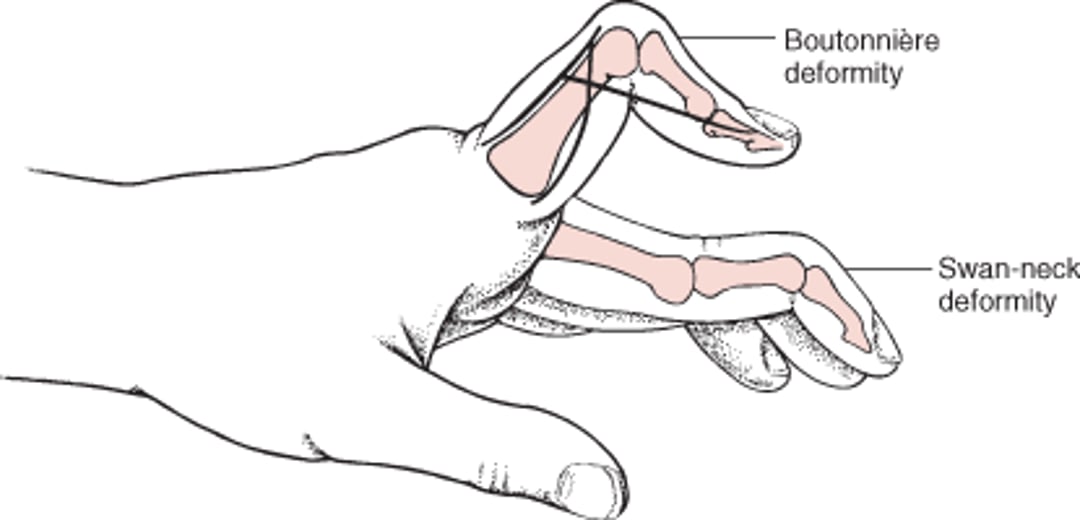
Swan neck deformity is characterized by extension at proximal interphalangeal joint and flexion at distal interphalangeal joint.
SCIENCE PHOTO LIBRARY


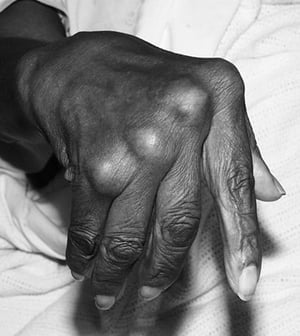
There are multiple boutonnière deformities of the fingers and thumbs in this patient with advanced rheumatoid arthritis. Boutonnière deformity is characterized by flexion at the proximal interphalangeal joint and hyperextension at the distal interphalangeal joint. There also are multiple rheumatoid nodules over the knuckles and interphalangeal joints.
By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.

This image of a patient with long-standing rheumatoid arthritis shows synovitis of the metacarpophalangeal joints with an ulnar drift of the digits.
By permission of the publisher. From Mabrey J: Current Orthopedic Diagnosis and Treatment. Edited by JD Heckman, RC Schenck, and A Agarwal. Philadelphia, Current Medicine, 2002.
Swan neck deformity is characterized by extension at proximal interphalangeal joint and flexion at distal interphalangeal joint.
SCIENCE PHOTO LIBRARY
There are multiple boutonnière deformities of the fingers and thumbs in this patient with advanced rheumatoid arthritis. Boutonnière deformity is characterized by flexion at the proximal interphalangeal joint and hyperextension at the distal interphalangeal joint. There also are multiple rheumatoid nodules over the knuckles and interphalangeal joints.
By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
This image of a patient with long-standing rheumatoid arthritis shows synovitis of the metacarpophalangeal joints with an ulnar drift of the digits.
By permission of the publisher. From Mabrey J: Current Orthopedic Diagnosis and Treatment. Edited by JD Heckman, RC Schenck, and A Agarwal. Philadelphia, Current Medicine, 2002.
Boutonnière and Swan-Neck Deformities

Extra-articular manifestations
Subcutaneous rheumatoid nodules are not usually an early sign but eventually develop in up to 30% of patients, usually at sites of pressure and chronic irritation (eg, the extensor surface of the forearm, metacarpophalangeal joints, soles of feet) (1). Paradoxically, rheumatoid nodule formation can increase (accelerated nodulosis) in patients taking methotrexate, despite suppressing joint inflammation. Visceral nodules (eg, pulmonary) are usually asymptomatic and may occur in severe rheumatoid arthritis. Pulmonary nodules of rheumatoid arthritis cannot be distinguished from pulmonary nodules of other etiology without biopsy.). Paradoxically, rheumatoid nodule formation can increase (accelerated nodulosis) in patients taking methotrexate, despite suppressing joint inflammation. Visceral nodules (eg, pulmonary) are usually asymptomatic and may occur in severe rheumatoid arthritis. Pulmonary nodules of rheumatoid arthritis cannot be distinguished from pulmonary nodules of other etiology without biopsy.
Other extra-articular complications include vasculitis causing leg ulcers, digital ischemia, or multiple mononeuropathy (mononeuritis multiplex); pleural or pericardial effusions;obliterative bronchiolitis; interstitial lung disease; pericarditis; myocarditis; lymphadenopathy; Felty syndrome; Sjögren syndrome; scleromalacia; and episcleritis.
Involvement of the cervical spine, generally in patients with longstanding destructive disease, can cause atlantoaxial subluxation and spinal cord compression; subluxation may worsen with extension of the neck (eg, during endotracheal intubation). Importantly, cervical spine instability is usually asymptomatic.


Image courtesy of Kinanah Yaseen, MD.
Patients with rheumatoid arthritis are at increased risk for early coronary artery disease, metabolic bone disease such as osteopenia and osteoporosis, and various cancers (lung, lymphoproliferative disorders, and nonmelanoma skin cancers), which may be related to underlying, uncontrolled systemic inflammatory processes (2).

Subcutaneous rheumatoid nodules (arrow) commonly form over pressure points as in this patient with olecranon bursitis. The nodules may be within subcutaneous tissue overlying the bursae or may be subperiosteal to the extensor surface of the ulna.
By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.

This photo shows rheumatoid nodules on the sole of the foot in a patient with rheumatoid arthritis. Rheumatoid nodules are often associated with surrounding fluid in a pressure-exacerbated "pseudobursa."
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This photo shows a rheumatoid nodule over the metacarpal joint of a patient with rheumatoid arthritis.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Subcutaneous rheumatoid nodules (arrow) commonly form over pressure points as in this patient with olecranon bursitis. The nodules may be within subcutaneous tissue overlying the bursae or may be subperiosteal to the extensor surface of the ulna.
By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
This photo shows rheumatoid nodules on the sole of the foot in a patient with rheumatoid arthritis. Rheumatoid nodules are often associated with surrounding fluid in a pressure-exacerbated "pseudobursa."
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This photo shows a rheumatoid nodule over the metacarpal joint of a patient with rheumatoid arthritis.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Symptoms and signs references
1. Kimbrough BA, Crowson CS, Davis JM 3rd, et al: Decline in Incidence of Extra-Articular Manifestations of Rheumatoid Arthritis: A Population-Based Cohort Study. Arthritis Care Res (Hoboken). Published online September 10, 2023. doi:10.1002/acr.25231
2. Figus FA, Piga M, Azzolin I, McConnell R, Iagnocco A: Rheumatoid arthritis: extra-articular manifestations and comorbidities. Autoimmun Rev 20(4):102776, 2021. doi:10.1016/j.autrev.2021.102776
Diagnosis of Rheumatoid Arthritis
Clinical criteria
Serum rheumatoid factor (RF), anticyclic citrullinated peptide (anti-CCP), and erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP)
Imaging (radiographs, ultrasound, or MRI)
Rheumatoid arthritis should be suspected in patients with polyarticular, symmetric arthritis, particularly if the wrists and 2nd and 3rd metacarpophalangeal joints are involved. Classification criteria serve as a guide to diagnose rheumatoid arthritis and are helpful in defining standardized treatment populations for study purposes. Criteria include laboratory test results for RF, anti-CCP, and ESR or CRP (see table Classification Criteria for Rheumatoid Arthritis). However, diagnosis requires documented joint inflammation and should not be based on laboratory testing alone.
Other causes of symmetric polyarthritis, particularly hepatitis C, must be excluded. Obtaining baseline radiographs of affected joints should be considered to help document progression of disease (erosive changes, joint space narrowing) over time. In patients who have prominent lumbar symptoms, alternative diagnoses should be investigated.
Classification Criteria for Rheumatoid Arthritis
Finding | Score |
|---|---|
Criteria for evaluation:
Classification criteria for rheumatoid arthritis is a score-based algorithm. Scores for categories A‒D are added; a score ≥ 6 (highest possible total 10) is needed to classify a patient as having definite rheumatoid arthritis.a | |
A. Joint involvementb | |
1 large jointc | 0 |
2‒10 large joints | 1 |
1‒3 small jointsd (with or without involvement of large joints) | 2 |
4‒10 small joints (with or without involvement of large joints) | 3 |
>10 jointse (at least 1 small joint) | 5 |
B. Serology (at least 1 test result is needed for classification) | |
Negative RF and negative anti-CCP | 0 |
Low-positivef RF or low-positive anti-CCP | 2 |
High-positiveg RF or high-positive anti-CCP | 3 |
C. Acute-phase reactants (at least 1 test result is needed for classification) | |
Normal CRP and normal erythrocyte sedimentation rate | 0 |
Abnormal CRP or abnormal erythrocyte sedimentation rate | 1 |
D. Duration of symptoms (based on patient's report) | |
< 6 weeks | 0 |
≥ 6 weeks | 1 |
a Patients with a score of < 6 can be reassessed; they may meet the criteria for rheumatoid arthritis cumulatively over time. | |
b Distal interphalangeal joints, first carpometacarpal joints, and first metatarsophalangeal joints are excluded from assessment. | |
c Large joints are the shoulders, elbows, hips, knees, and ankles. | |
d Small joints are the metacarpophalangeal joints, proximal interphalangeal joints, 2nd‒5th metatarsophalangeal joints, thumb interphalangeal joints, and wrists. | |
e These joints may include other joints not specifically listed elsewhere (eg, temporomandibular, acromioclavicular, sternoclavicular). | |
f Low positive indicates levels between 1 and 3 times the upper limit of normal. | |
g High positive indicates levels at least 3 times the upper limit of normal. | |
Anti-CCP = anticitrullinated protein antibody; CRP = C-reactive protein; RF = rheumatoid factor. | |
Adapted from Aletaha D, Neogi T, Silman AJ, et al: 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 62 (9):2569–2581, 2010. | |
RFs, antibodies to human gamma-globulin, are present in approximately 70% of patients with rheumatoid arthritis (1). However, RF, often in low titers (levels can vary between laboratories), occurs in patients with other diseases, including
Other systemic rheumatic diseases (eg, Sjögren syndrome, systemic lupus erythematosus)
Granulomatous diseases
Chronic infections (eg, viral hepatitis, bacterial endocarditis, tuberculosis)
Cancers
Low RF titers can also occur in 3% of the general population and 20% of older adults (2). Very high RF titers can occur in patients with hepatitis C infection and sometimes in patients with other chronic infections. An RF titer measured by latex agglutination of > 1:80 or a positive anti-CCP test supports the diagnosis of rheumatoid arthritis in the appropriate clinical context, but other causes must be excluded.
Anti-CCP antibodies have high specificity (90%) and sensitivity (approximately 77 to 86%) for rheumatoid arthritis and, like RF, predict a worse prognosis. RF and anti-CCP values do not fluctuate with disease activity. Anti-CCP antibodies are notably absent in patients with hepatitis C who may have a positive RF titer and joint swelling related to the viral infection.


By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.


Image courtesy of Kinanah Yaseen, MD.
Radiographs show only soft-tissue swelling during the first months of disease. Subsequently, periarticular osteoporosis, joint space (articular cartilage) narrowing, and marginal erosions may become visible. Erosions often develop within the first year but may occur any time. Ultrasonography can detect synovial thickening and bone erosions. Synovitis and tenosynovitis can also be identified with ultrasonography using power Doppler. MRI is the most sensitive and detects earlier articular inflammation and erosions. In addition, abnormal subchondral bone signals (eg, bone marrow lesions, bone marrow edema) around the knee suggest progressive disease.
If rheumatoid arthritis is diagnosed, additional tests help detect complications and unexpected abnormalities. Complete blood count with differential should be obtained. A normochromic (or slightly hypochromic)-normocytic anemia occurs in up to 60% (3); hemoglobin is usually > 10 g/dL (100 g/L). If hemoglobin is ≤ 10 g/dL (100 g/L), superimposed iron deficiency or other causes of anemia should be considered. Neutropenia occurs in 1 to 2% of cases, often with splenomegaly (Felty syndrome). Acute-phase reactants (eg, thrombocytosis, elevated ESR, elevated CRP) reflect disease activity. A mild polyclonal hypergammaglobulinemia often occurs. ESR and CRP are elevated in the majority of patients with active disease.
Validated measures of disease activity include the Rheumatoid Arthritis Disease Activity Score DAS-28 and Rheumatoid Arthritis Clinical Disease Activity Index.
Synovial fluid examination is necessary with any acute effusion to rule out other disorders and differentiate rheumatoid arthritis from other inflammatory arthritides (eg, septic and crystal-induced arthritis). In rheumatoid arthritis, during active joint inflammation, synovial fluid is turbid, yellow, and sterile, and usually has white blood cell counts 10,000 to 50,000/mcL (10 ×109/L to 50 ×109/L); polymorphonuclear leukocytes typically predominate, but > 50% may be lymphocytes and other mononuclear cells. Crystals are absent.

Differential diagnosis
Many disorders can simulate rheumatoid arthritis:
Chronic crystal-induced arthritis (especially CPPD)
Sarcoidosis (rarely causes a polyarticular arthritis)
Infectious causes such as hepatitis C, parvovirus B19, alpha virus, Lyme disease, and Whipple disease
Some patients with crystal-induced arthritis, especially calcium pyrophosphate arthritis, may meet criteria for rheumatoid arthritis; however, synovial fluid examination should clarify the diagnosis. The presence of crystals makes rheumatoid arthritis unlikely, although calcium pyrophosphate crystal disease and rheumatoid arthritis may coexist in the same patient. Joint involvement and subcutaneous nodules can result from SLE, gout, cholesterol, and amyloidosis as well as rheumatoid arthritis; aspiration or biopsy of the nodules may occasionally be needed.
SLE usually can be distinguished if there are skin lesions on light-exposed areas, hair loss, oral and nasal mucosal lesions, absence of joint erosions in even long-standing arthritis, joint fluid that often has white blood cell counts < 2000/mcL (2 × 109/L) (predominantly mononuclear cells), antibodies to double-stranded DNA, renal disease, and low serum complement levels. In contrast to rheumatoid arthritis, swan neck and ulnar deviation deformities in SLE (Jaccoud arthropathy) often lack marked synovial proliferation and are usually reducible.
Arthritis similar to rheumatoid arthritis can also occur in other rheumatic disorders (eg, polyarteritis, systemic sclerosis, dermatomyositis, or polymyositis), or there can be features of more than one disease, which suggests an overlap syndrome.
Sarcoidosis, Whipple disease, multicentric reticulohistiocytosis, and other systemic diseases may involve joints; other clinical features and tissue biopsy sometimes help differentiate these conditions. Acute rheumatic fever has a migratory pattern of joint involvement and evidence of antecedent streptococcal infection (culture or changing antistreptolysin O titer); in contrast, rheumatoid arthritis tends to involve joints in an additive and persistent manner over time.
Reactive arthritis can be differentiated by antecedent gastrointestinal or genitourinary symptoms; asymmetric involvement of predominantly large joints or with a diffusely swollen (sausage) digit (dactylitis) and pain at the Achilles insertion of the heel and sacroiliac joints; conjunctivitis; iritis; painless buccal ulcers; balanitis circinata; or keratoderma blennorrhagicum on the soles and elsewhere.
Psoriatic arthritis tends to be asymmetric and is not usually associated with RF, but clinical differentiation may be difficult in the absence of nail or skin lesions. Distal interphalangeal joint involvement and severely mutilating arthritis (arthritis mutilans) is strongly suggestive, as is the presence of dactylitis. Psoriatic arthritis may involve the sacroiliac joints and lower spine. Distinguishing between psoriatic arthritis and rheumatoid arthritis is important because response to some specific drugs differs.
Ankylosing spondylitis may be differentiated by spinal and axial joint involvement, absence of subcutaneous nodules, and a negative RF test. The HLA-B27 allele is present in 90% of White patients with ankylosing spondylitis.
Osteoarthritis can be differentiated by the joints involved; the absence of rheumatoid nodules, systemic manifestations, or high titer of RF or anti-CCP; and by synovial fluid white blood cell counts < 2000/mcL (2 × 109/L). Osteoarthritis of the hands most typically involves the distal interphalangeal (DIP) joints, bases of the thumbs, and proximal interphalangeal (PIP) joints. Osteoarthritis may involve the metacarpophalangeal joints, but usually less so than the other joints, and typically spares the ulnar styloid area and wrist. Rheumatoid arthritis does not affect the DIP joints.
Diagnosis references
1. Nishimura K, Sugiyama D, Kogata Y, et al: Meta-analysis: diagnostic accuracy of anti-cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Ann Intern Med 146(11):797-808, 2007. doi:10.7326/0003-4819-146-11-200706050-00008
2. Ingegnoli F, Castelli R, Gualtierotti R: Rheumatoid factors: clinical applications. Dis Markers. 2013;35(6):727-734. doi:10.1155/2013/726598
3. Wilson A, Yu HT, Goodnough LT, Nissenson AR. Prevalence and outcomes of anemia in rheumatoid arthritis: a systematic review of the literature. Am J Med. 2004;116 Suppl 7A:50S-57S. doi:10.1016/j.amjmed.2003.12.012
Nonpharmacologic Treatment of Rheumatoid Arthritis
Lifestyle measures (eg, smoking cessation, balanced nutrition, quality sleep)
Physical measures (eg, joint splinting)
Sometimes surgery
Nonpharmacologic treatment of rheumatoid arthritis involves a balance of rest and exercise, adequate nutrition, physical measures, and sometimes surgery. Early diagnosis and treatment in rheumatoid arthritis predict improved outcomes. A treat-to-target approach to achieve full disease remission or minimal disease activity has been recommended by the American College of Rheumatology (ACR) (1) and European League Against Rheumatism (EULAR) (2).
(See also Pharmacologic Therapy for Rheumatoid Arthritis.)
Lifestyle measures
Lifestyle measures measure play an important role in disease management, and detailed recommendations have been provided by the ACR (3) and EULAR (4). These measures include regular exercise, maintaining a healthy diet, achieving and maintaining a healthy weight, moderate alcohol consumption, smoking cessation, and worksite modifications if needed for active work participation. Quality sleep should also be encouraged, because poor sleep may exacerbate pain.
A nutritious diet, such as the "Mediterranean diet" which is high in fruits and vegetables and low in processed food, is encouraged. In addition to the cardiovascular benefits of the Mediterranean diet, limited observational data suggest that it also has beneficial effects on pain in patients with rheumatoid arthritis. Some patients have food-associated exacerbations (5); however, no specific foods have reproducibly been shown to exacerbate or lessen the symptoms of rheumatoid arthritis. Substituting omega-3 fatty acids (in fish oils) for dietary omega-6 fatty acids (in meats) partially relieves symptoms in some patients, which are thought to act by transiently decreasing production of inflammatory prostaglandins and possibly by modifying the gut microbiome.
Food and diet misinformation targeting rheumatoid arthritis patients is common, and patients should be directed to reliable sources of information.
Physical measures
Joint splinting may relieve severe symptoms of pain or compressive neuropathies. Cold may be applied to reduce joint pain and swelling. Orthopedic or athletic shoes with good heel and arch support are frequently helpful; metatarsal supports placed posteriorly (proximal) to painful metatarsophalangeal joints decrease the pain of weight bearing. Molded shoes may be needed for severe deformities. Occupational therapy and self-help devices enable many patients with debilitating rheumatoid arthritis to perform activities of daily living.
Exercise should proceed as tolerated. During acute inflammation, passive range-of-motion exercise helps prevent flexion contractures. Heat therapy can be applied to help alleviate stiffness. Range-of-motion exercises done in warm water are helpful because heat improves muscle function by reducing stiffness and muscle spasm. However, contractures can be prevented and muscle strength can be restored more successfully after inflammation begins to subside; active exercise (including walking and specific exercises for involved joints) to restore muscle mass and preserve range of joint motion are recommended. Flexion contractures may require intensive exercise, casting, or immobilization (eg, splinting) in progressively more stretched-open positions. Paraffin baths can warm digits and facilitate finger exercise.
Massage by trained therapists, traction, and deep heat treatment with diathermy or ultrasonography may be transiently useful adjuncts to pharmacologic therapy.
Surgery
Surgery may be considered if pharmacologic therapy is unsuccessful. Surgery must always be considered in terms of the total disease burden and patient expectations. For example, deformed hands and arms limit crutch use during rehabilitation; seriously affected knees and feet limit benefit from hip surgery. Reasonable objectives for each patient must be determined, and function must be considered; straightening ulnar-deviated fingers may not improve hand function. Surgery is preferably performed during periods of disease quiescence or low disease activity, but may need to be done during active disease.
Arthroplasty with prosthetic joint replacement is indicated if damage severely limits function; total hip and knee replacement outcomes are generally favorable (6, 7). Prosthetic hips and knees may limit vigorous activity (eg, competitive athletics). Excision of subluxed painful metatarsophalangeal joints may greatly aid walking. Thumb fusions may provide stability for pinch function. Neck fusion may be needed for significant C1-2 subluxation with severe pain or potential for spinal cord compression. Arthroscopic or open synovectomy can relieve joint inflammation but only temporarily unless disease activity can be controlled. Withholding some immunosuppressive medications (not necessarily methotrexate) at the time of arthroplasty should be considered to limit the risk of infection (). Prosthetic hips and knees may limit vigorous activity (eg, competitive athletics). Excision of subluxed painful metatarsophalangeal joints may greatly aid walking. Thumb fusions may provide stability for pinch function. Neck fusion may be needed for significant C1-2 subluxation with severe pain or potential for spinal cord compression. Arthroscopic or open synovectomy can relieve joint inflammation but only temporarily unless disease activity can be controlled. Withholding some immunosuppressive medications (not necessarily methotrexate) at the time of arthroplasty should be considered to limit the risk of infection (8). Even low-dose prednisone (< 7.5 mg a day) may increase infectious risk.). Even low-dose prednisone (< 7.5 mg a day) may increase infectious risk.
Nonpharmacologic treatment references
1. Fraenkel L, Bathon JM, England BR, et al: 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol 73(7):1108-1123, 2021. doi:10.1002/art.41752
2. Smolen JS, Landewé RBM, Bijlsma JWJ, et al: EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis 79(6):685-699, 2020. doi:10.1136/annrheumdis-2019-216655
3. England BR, Smith BJ, Baker NA, et al: 2022 American College of Rheumatology Guideline for Exercise, Rehabilitation, Diet, and Additional Integrative Interventions for Rheumatoid Arthritis. Arthritis Rheumatol 75(8):1299-1311, 2023. doi:10.1002/art.42507
4. Gwinnutt JM, Wieczorek M, Balanescu A, et al: 2021 EULAR recommendations regarding lifestyle behaviours and work participation to prevent progression of rheumatic and musculoskeletal diseases. Ann Rheum Dis 82(1):48-56, 2023. doi:10.1136/annrheumdis-2021-222020
5. Tedeschi SK, Frits M, Cui J, et al: Diet and Rheumatoid Arthritis Symptoms: Survey Results From a Rheumatoid Arthritis Registry. Arthritis Care Res (Hoboken). 2017;69(12):1920-1925. doi:10.1002/acr.23225
6. Zhang Y, Chu SS, Liu K, Huang Q, Wang Y: Outcomes in patients with rheumatoid versus osteoarthritis for total hip arthroplasty: a meta-analysis and systematic review. Semin Arthritis Rheum 56:152061, 2022. doi:10.1016/j.semarthrit.2022.152061
7. Burn E, Edwards CJ, Murray DW, et al: The effect of rheumatoid arthritis on patient-reported outcomes following knee and hip replacement: evidence from routinely collected data. Rheumatology (Oxford) 58(6):1016-1024, 2019. doi:10.1093/rheumatology/key409
8. Goodman SM, Springer B, Guyatt G, et al: 2017 American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication in Patients With Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty. Arthritis Rheumatol 69(8):1538-1551, 2017. doi:10.1002/art.40149
Pharmacologic Therapy for Rheumatoid Arthritis
The goal is to reduce inflammation to prevent erosions, progressive deformity, and loss of joint function. A treat-to-target approach to achieve full disease remission or minimal disease activity has been suggested (1, 2). Disease-modifying antirheumatic drugs (DMARDs) have been shown to improve outcomes and are indicated for all patients. DMARDs can be broadly characterized into 3 types:
Conventional synthetic DMARDs (eg, methotrexate, sulfasalazine, leflunomide)Conventional synthetic DMARDs (eg, methotrexate, sulfasalazine, leflunomide)
Biologic DMARDs (eg, tumor necrosis factor [TNF] inhibitors, interleukin [IL]-6, abatacept)Biologic DMARDs (eg, tumor necrosis factor [TNF] inhibitors, interleukin [IL]-6, abatacept)
Targeted synthetic DMARDs (eg, tofacitinib, upadacitinib)Targeted synthetic DMARDs (eg, tofacitinib, upadacitinib)
The optimal medication regimen for any particular patient is unknown. The choice of agents often depends on various factors, including disease activity, comorbidities, cost, and response to previous therapies. In many instances, combinations of DMARDs are used (eg, methotrexate plus a TNF inhibitor; methotrexate plus abatacept). In general, biologic agents are not given in combination with each other due to increased frequency of infections. The following is an example of initial therapy:The optimal medication regimen for any particular patient is unknown. The choice of agents often depends on various factors, including disease activity, comorbidities, cost, and response to previous therapies. In many instances, combinations of DMARDs are used (eg, methotrexate plus a TNF inhibitor; methotrexate plus abatacept). In general, biologic agents are not given in combination with each other due to increased frequency of infections. The following is an example of initial therapy:
Methotrexate 10 to 15 mg orally once a week (with folic acid 1 mg orally once/day) is given.Methotrexate 10 to 15 mg orally once a week (with folic acid 1 mg orally once/day) is given.
If tolerated and not adequate, the dosage of weekly methotrexate is increased at 3- to 5-week intervals to a maximum of 25 mg orally or by injection (oral bioavailability decreases above 15 mg if given in a single dose).If tolerated and not adequate, the dosage of weekly methotrexate is increased at 3- to 5-week intervals to a maximum of 25 mg orally or by injection (oral bioavailability decreases above 15 mg if given in a single dose).
If response is not adequate, a biologic agent is usually added. Alternatively, triple therapy with methotrexate, hydroxychloroquine, and sulfasalazine is a cost-effective option, but long-term tolerability is challenging. If response is not adequate, a biologic agent is usually added. Alternatively, triple therapy with methotrexate, hydroxychloroquine, and sulfasalazine is a cost-effective option, but long-term tolerability is challenging.
Leflunomide may be used instead of methotrexate or added to methotrexate with close monitoring of serum transaminase levels and complete blood count.Leflunomide may be used instead of methotrexate or added to methotrexate with close monitoring of serum transaminase levels and complete blood count.
Methotrexate and leflunomide (and some other medications) must be avoided if pregnancy is anticipated.Methotrexate and leflunomide (and some other medications) must be avoided if pregnancy is anticipated.
Nonsteroidal anti-inflammatory drugs (NSAIDs) may be used for analgesia, but they do not prevent erosions or disease progression and may slightly increase cardiovascular risk; therefore, their use should be limited. Low-dose systemic corticosteroids (prednisone Nonsteroidal anti-inflammatory drugs (NSAIDs) may be used for analgesia, but they do not prevent erosions or disease progression and may slightly increase cardiovascular risk; therefore, their use should be limited. Low-dose systemic corticosteroids (prednisone< 7.5 mg once a day) may be added to control severe polyarticular symptoms, usually with the objective of replacement with a DMARD. Intra-articular corticosteroids can control severe monarticular or even oligoarticular symptoms but with chronic use may have adverse metabolic and structural cartilage effects. Studies indicate infectious and metabolic adverse effects from even low-dose chronic corticosteroid use; thus limitation of use is a treatment priority (3).
Conventional synthetic DMARDs
(See table Medications Used to Treat Rheumatoid Arthritis for adverse effects of other medications used to treat rheumatoid arthritis.)
Conventional synthetic (nonbiologic) DMARDs slow the progression of rheumatoid arthritis and are indicated for nearly all patients with rheumatoid arthritis. They differ from each other chemically and pharmacologically. Many take weeks or months to have an effect. Many conventional synthetic DMARDs result in evidence of decreased damage on imaging studies, presumably reflecting decreased disease activity (4). Patients should be fully apprised of the risks of these medications and monitored closely for evidence of toxicity.
Medications Used to Treat Rheumatoid Arthritis
Medication | Adverse Effects |
|---|---|
Conventional synthetic disease-modifying antirheumatic drugs (DMARDs) | |
HydroxychloroquineHydroxychloroquine | Dermatitis, may be photosensitive Rarely, myopathy or cardiomyopathy Corneal opacity (generally reversible) Rarely, irreversible retinal degeneration |
LeflunomideLeflunomide | Skin reactions Hepatic dysfunction Alopecia Diarrhea Peripheral neuropathy Teratogenicity |
MethotrexateMethotrexate | Liver fibrosis (dose-related, often reversible) Nausea Malaise Bone marrow suppression Stomatitis Rarely, pneumonitis Teratogenicity, abortifacient effect |
Sulfasalazine*Sulfasalazine* | Bone marrow suppression Gastric symptoms Neutropenia (usually on initiation of treatment) Hemolysis Hepatitis Reversible oligospermia |
Corticosteroids, intra-articular injections | |
Methylprednisolone acetateMethylprednisolone acetate Triamcinolone acetonideTriamcinolone acetonide Triamcinolone hexacetonideTriamcinolone hexacetonide | Rarely infection at the injection site Local skin hypopigmentation or atrophy |
Corticosteroids, systemic | |
PrednisonePrednisone PrednisolonePrednisolone | With long-term use:
|
Biologic agents | |
AbataceptAbatacept | Pulmonary toxicity Susceptibility to infection Headache Upper respiratory infection Sore throat Nausea |
RituximabRituximab | During administration:
After administration:
|
Interleukin-6 (IL-6) inhibitors‡ | |
Tocilizumab Tocilizumab SarilumabSarilumab | Potential risk of infection (particularly opportunistic organisms) Neutropenia Thrombocytopenia Gastrointestinal perforation Anaphylaxis Transaminase elevation Dyslipidemia (particularly elevated low-density lipoproteins [LDL]) |
Interleukin-1 (IL-1) receptor inhibitor‡ | |
AnakinraAnakinra | Injection site reactions Risk of infection Neutropenia |
Tumor necrosis factor (TNF) inhibitors‡ | |
AdalimumabAdalimumab Certolizumab pegolCertolizumab pegol EtanerceptEtanercept GolimumabGolimumab InfliximabInfliximab | Potential risk of reactivation of latent infection (particularly tuberculosis, hepatitis B, and fungal infections) Nonmelanoma skin cancers Antinuclear antibodies with or without clinical systemic lupus erythematosus (SLE) Demyelinating neurologic disorders Heart failure worsening |
Janus kinase (JAK) inhibitors | |
BaricitinibBaricitinib TofacitinibTofacitinib Upadacitinib Upadacitinib | Risk of infection, particularly varicella-zoster virus reactivation Nonmelanoma skin cancers Hypercholesterolemia Venous thromboembolism Major adverse cardiovascular events Lung cancer |
* Sulfasalazine is usually given as enteric-coated tablets.* Sulfasalazine is usually given as enteric-coated tablets. † During dosage increases for azathioprine, complete blood count, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) are monitored.† During dosage increases for azathioprine, complete blood count, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) are monitored. ‡ These medications are biologic disease-modifying antirheumatic drugs (DMARDs). § These medications are targeted synthetic DMARDs. | |
When using conventional synthetic DMARDs, the following principles should be considered:
Combinations of DMARDs may be more effective than a single agent. For example, hydroxychloroquine, sulfasalazine, and methotrexate together are more effective than methotrexate alone or the other two together (Combinations of DMARDs may be more effective than a single agent. For example, hydroxychloroquine, sulfasalazine, and methotrexate together are more effective than methotrexate alone or the other two together (5).
Combining a DMARD with a biologic DMARD, such as methotrexate plus a tumor necrosis factor (TNF) inhibitor or a rapidly tapered corticosteroid, may be more effective than using a single DMARD alone.Combining a DMARD with a biologic DMARD, such as methotrexate plus a tumor necrosis factor (TNF) inhibitor or a rapidly tapered corticosteroid, may be more effective than using a single DMARD alone.
MethotrexateMethotrexate is a folate antagonist with immunosuppressive effects at high dose. It is anti-inflammatory at the lower doses used in rheumatoid arthritis. Clinical benefit is usually observed within 6 weeks, but it may take up to 3 months or more. Methotrexate should be used with caution, if at all, in patients with hepatic dysfunction or renal impairment. Frequent alcohol consumption should be avoided. Supplemental folate, typically given as folic acid 1 mg orally once/day, reduces the likelihood of adverse effects. Complete blood count (CBC), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and albumin and creatinine level should be determined about every 8 to 12 weeks. When used early in the course of rheumatoid arthritis, efficacy may be comparable to the biologic agents. Severe relapses of arthritis can occur after withdrawal of methotrexate. Paradoxically, rheumatoid nodules may enlarge with methotrexate therapy. In rheumatoid arthritis patients with stable parenchymal lung disease, methotrexate can be continued with close monitoring of their respiratory status, if the methotrexate is controlling joint inflammation.is a folate antagonist with immunosuppressive effects at high dose. It is anti-inflammatory at the lower doses used in rheumatoid arthritis. Clinical benefit is usually observed within 6 weeks, but it may take up to 3 months or more. Methotrexate should be used with caution, if at all, in patients with hepatic dysfunction or renal impairment. Frequent alcohol consumption should be avoided. Supplemental folate, typically given as folic acid 1 mg orally once/day, reduces the likelihood of adverse effects. Complete blood count (CBC), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and albumin and creatinine level should be determined about every 8 to 12 weeks. When used early in the course of rheumatoid arthritis, efficacy may be comparable to the biologic agents. Severe relapses of arthritis can occur after withdrawal of methotrexate. Paradoxically, rheumatoid nodules may enlarge with methotrexate therapy. In rheumatoid arthritis patients with stable parenchymal lung disease, methotrexate can be continued with close monitoring of their respiratory status, if the methotrexate is controlling joint inflammation.
HydroxychloroquineHydroxychloroquine can also control symptoms of mild rheumatoid arthritis. Funduscopic examination should be done and visual fields should be assessed before and every 12 months during treatment. Hydroxychloroquine should be stopped if no joint improvement occurs after 9 months.can also control symptoms of mild rheumatoid arthritis. Funduscopic examination should be done and visual fields should be assessed before and every 12 months during treatment. Hydroxychloroquine should be stopped if no joint improvement occurs after 9 months.
SulfasalazineSulfasalazine can alleviate symptoms and slow development of joint damage. It is usually given as enteric-coated tablets. Benefit should occur within 3 months. Enteric coating or dose reduction may increase tolerability. Because neutropenia may occur early, CBCs should be obtained after 1 to 2 weeks and then about every 12 weeks during therapy. AST and ALT should be obtained at about 6-month intervals and whenever the dose is increased. In male patients, sulfasalazine may cause reversible oligospermia. can alleviate symptoms and slow development of joint damage. It is usually given as enteric-coated tablets. Benefit should occur within 3 months. Enteric coating or dose reduction may increase tolerability. Because neutropenia may occur early, CBCs should be obtained after 1 to 2 weeks and then about every 12 weeks during therapy. AST and ALT should be obtained at about 6-month intervals and whenever the dose is increased. In male patients, sulfasalazine may cause reversible oligospermia.
LeflunomideLeflunomide interferes with an enzyme involved with pyrimidine metabolism. It is about as effective as methotrexate but is less likely to suppress bone marrow, cause abnormal liver function, or cause pneumonitis. Alopecia and diarrhea are fairly common at the onset of therapy but may resolve with continuation of therapy.interferes with an enzyme involved with pyrimidine metabolism. It is about as effective as methotrexate but is less likely to suppress bone marrow, cause abnormal liver function, or cause pneumonitis. Alopecia and diarrhea are fairly common at the onset of therapy but may resolve with continuation of therapy.
Biologic DMARDs
Tumor necrosis factor inhibitors (eg, adalimumab, etanercept, golimumab, certolizumab pegol, infliximab, and their biosimilars) reduce the progression of erosions and reduce the number of new erosions. Although not all patients respond, many have a prompt, dramatic feeling of well being, sometimes with the first injection. Inflammation is often dramatically reduced. These agents are often added to methotrexate therapy to increase the effect and possibly prevent the development of drug-neutralizing antibodies.(eg, adalimumab, etanercept, golimumab, certolizumab pegol, infliximab, and their biosimilars) reduce the progression of erosions and reduce the number of new erosions. Although not all patients respond, many have a prompt, dramatic feeling of well being, sometimes with the first injection. Inflammation is often dramatically reduced. These agents are often added to methotrexate therapy to increase the effect and possibly prevent the development of drug-neutralizing antibodies.
Safety data suggest treatment with TNF inhibitors may be continued during the first and second trimesters of pregnancy, with most professional societies recommending they be stopped in the third trimester. However, due to its pegylated formulation, certolizumab is a TNF inhibitor that does not cross the placenta and can be continued throughout the pregnancy (6). TNF inhibitors should usually be stopped before major surgery to decrease the risk of perioperative infection (7). TNF inhibitors may predispose to heart failure and thus are relatively contraindicated in stage 3 and stage 4 heart failure. There is a minimal risk of lymphoma in rheumatoid arthritis patients who are being treated with TNF inhibitors. 2015 ACR guidelines conditionally recommended using DMARDs, rituximab, or abatacept instead of TNF inhibitors in patients with history of lymphoma (). TNF inhibitors may predispose to heart failure and thus are relatively contraindicated in stage 3 and stage 4 heart failure. There is a minimal risk of lymphoma in rheumatoid arthritis patients who are being treated with TNF inhibitors. 2015 ACR guidelines conditionally recommended using DMARDs, rituximab, or abatacept instead of TNF inhibitors in patients with history of lymphoma (8). Evidence regarding solid tumors in TNF inhibitors is mixed. Other possible adverse events of TNF inhibitors include injection site reaction, acute and delayed infusion reaction, demyelinating disease, granulomatous diseases such as sarcoidosis, cytopenias (especially neutropenia), cutaneous vasculitis, psoriasis, and rarely antineutrophilic cytoplasmic associated vasculitis. A major concern is the reactivation of mycobacterial or fungal infections.
Biosimilar forms of several TNF inhibitors (and other biologic agents) are commercially available, and additional agents are in development. Biosimilars are highly similar to the reference product in terms of efficacy and toxicity, but they may differ slightly in their molecular structure. (See also U.S. Food and Drug Administration: Biosimilar Product Information and European Medicines Agency: Biosimilars.)
TocilizumabTocilizumab is an interleukin (IL-6) inhibitor and has clinical efficacy in patients who have responded incompletely to other biologic agents. It may be used as monotherapy but can also be given in combination with methotrexate or another conventional synthetic DMARD.is an interleukin (IL-6) inhibitor and has clinical efficacy in patients who have responded incompletely to other biologic agents. It may be used as monotherapy but can also be given in combination with methotrexate or another conventional synthetic DMARD.
SarilumabSarilumab is an IL-6 inhibitor. It is available for adults with moderately to severely active rheumatoid arthritis who have had an inadequate response to or are intolerant of one or more DMARDs.
Abatacept,Abatacept, a soluble fusion cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) immunoglobulin, is indicated for patients with rheumatoid arthritis with an inadequate response to other DMARDs. Abatacept is conditionally recommended over other biologic DMARDs in patients with rheumatoid arthritis and non-tuberculous mycobacterial lung disease.a soluble fusion cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) immunoglobulin, is indicated for patients with rheumatoid arthritis with an inadequate response to other DMARDs. Abatacept is conditionally recommended over other biologic DMARDs in patients with rheumatoid arthritis and non-tuberculous mycobacterial lung disease.
Rituximab Rituximabis an anti-CD 20 antibody that depletes B cells. It can be used in patients refractory to other treatments. Response is often delayed but may last 6 months. The course can be repeated after 6 months. Mild infusion reactions are common, and analgesia, corticosteroids, diphenhydramine, or a combination may need to be given concomitantly. Rituximab therapy has rarely been associated with is an anti-CD 20 antibody that depletes B cells. It can be used in patients refractory to other treatments. Response is often delayed but may last 6 months. The course can be repeated after 6 months. Mild infusion reactions are common, and analgesia, corticosteroids, diphenhydramine, or a combination may need to be given concomitantly. Rituximab therapy has rarely been associated withprogressive multifocal leukoencephalopathy (as have other immunosuppressive agents), mucocutaneous reactions, delayed leukopenia, and hepatitis B reactivation with hepatic necrosis. Patients taking rituximab may have a blunted immune response to the(as have other immunosuppressive agents), mucocutaneous reactions, delayed leukopenia, and hepatitis B reactivation with hepatic necrosis. Patients taking rituximab may have a blunted immune response to the COVID-19 vaccine and have poorer outcomes if infected with SARS-CoV-2. Therefore, rituximab is now generally reserved for patients who did not respond to other biologic DMARDs (including a combined TNF inhibitor and methotrexate) and to those with lymphoproliferative disorders. and have poorer outcomes if infected with SARS-CoV-2. Therefore, rituximab is now generally reserved for patients who did not respond to other biologic DMARDs (including a combined TNF inhibitor and methotrexate) and to those with lymphoproliferative disorders.
Rituximab therapy might be gradually discontinued if the patient has had low disease activity or been in remission for at least 6 months.Rituximab therapy might be gradually discontinued if the patient has had low disease activity or been in remission for at least 6 months.
AnakinraAnakinra is a recombinant interleukin-1 (IL-1) receptor antagonist. IL-1 is heavily involved in the pathogenesis of rheumatoid arthritis. Adverse effects include infection and leukopenia. It is rarely used because it lacks efficacy compared with other biologics and because it is a daily injection.
Although there are some differences among agents, the most serious concern with biologic and targeted synthetic DMARDs is infection, particularly with reactivated tuberculosis. Patients should be screened for tuberculosis with purified protein derivative (PPD) or an interferon-gamma release assay. Pretreatment serologic testing for hepatitis B and C should also be performed prior to treatment with DMARDs. Other serious infections can occur, including sepsis, invasive fungal infections, and infections due to other opportunistic organisms. Patients should be up to date on vaccinations prior to treatment with a biologic agent.
Targeted synthetic DMARDs
Janus kinase (JAK) inhibitors are targeted synthetic agents, also referred to as small molecule agents, that interfere with the communication between cells that coordinate inflammation by inhibiting the enzyme JAK. JAK inhibitors are administered orally and include the following (see also table Medications Used to Treat Rheumatoid Arthritis):
Tofacitinib,Tofacitinib, given with or without concomitant methotrexate to patients who do not respond to methotrexate alone or to other biologic agents.given with or without concomitant methotrexate to patients who do not respond to methotrexate alone or to other biologic agents.
Upadacitinib,Upadacitinib, given to adults with moderately to severely active rheumatoid arthritis who have had an inadequate response or intolerance to methotrexate.
Baricitinib,Baricitinib, indicated for adults with moderately to severely active rheumatoid arthritis who have had an inadequate response to one or more TNF inhibitors.
JAK inhibitors carry an increased incidence of herpes zoster; thus vaccination against zoster is strongly suggested prior to use of these medications. Patients should also be assessed for cardiovascular risk factors given the potential increased risk of major adverse cardiovascular events (MACEs; eg, myocardial infarction, stroke, venous thromboembolism, pulmonary embolism) with JAK inhibitors. A prospective, randomized, open-label study comparing tofacitinib (5 and 10 mg doses) with TNF inhibitors found that, after a median follow-up of 4 years, there was a higher risk of MACEs and cancer with tofacitinib than with TNF inhibitors, especially in patients over age 50 years and with at least 1 risk factor for cardiovascular disease (9). Although the study was limited to tofacitinib, these safety concerns have been applied to all of the JAK inhibitors until more data are available.
Other immunosuppressive agents
Other immunosuppressive agents, including azathioprine or cyclosporine (an immunomodulatory medication), have less efficacy and are rarely used because of an increased risk of toxicity. Thus, they are used only for patients in whom treatment with more traditional DMARDs has failed. Other immunosuppressive agents, including azathioprine or cyclosporine (an immunomodulatory medication), have less efficacy and are rarely used because of an increased risk of toxicity. Thus, they are used only for patients in whom treatment with more traditional DMARDs has failed.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Aspirin is no longer used for rheumatoid arthritis because effective doses are often toxic. Only one NSAID should be given at a time (see table Aspirin is no longer used for rheumatoid arthritis because effective doses are often toxic. Only one NSAID should be given at a time (see tableNSAID Treatment of Rheumatoid Arthritis), although patients may also take aspirin at ≤ 325 mg/day for its antiplatelet cardioprotective effect. Because the maximal response for NSAIDs can take up to 2 weeks, doses should be increased no more frequently than this. Doses of drugs with flexible dosing can be increased until response is maximal or maximum dosage is reached. All NSAIDs treat the symptoms of rheumatoid arthritis and decrease inflammation but do not alter the course of the disease; thus, they are only used adjunctively.
NSAIDs inhibit cyclooxygenase (COX) enzymes and thus decrease production of prostaglandins. Some prostaglandins under COX-1 control have important effects in many parts of the body (ie, they protect gastric mucosa and inhibit platelet adhesiveness). Other prostaglandins are induced by inflammation and are produced by COX-2. Selective COX-2 inhibitors, also called coxibs (eg, celecoxib), seem to have efficacy similar to nonselective NSAIDs and are slightly less likely to cause gastrointestinal toxicity; however, they are not less likely to cause renal toxicity. Celecoxib 200 mg orally once/day has a comparable cardiovascular safety profile to nonselective NSAIDs. It remains unclear whether full-dose celecoxib (200 mg orally 2 times a day ) has cardiovascular risks comparable to the nonselective NSAIDs.NSAIDs inhibit cyclooxygenase (COX) enzymes and thus decrease production of prostaglandins. Some prostaglandins under COX-1 control have important effects in many parts of the body (ie, they protect gastric mucosa and inhibit platelet adhesiveness). Other prostaglandins are induced by inflammation and are produced by COX-2. Selective COX-2 inhibitors, also called coxibs (eg, celecoxib), seem to have efficacy similar to nonselective NSAIDs and are slightly less likely to cause gastrointestinal toxicity; however, they are not less likely to cause renal toxicity. Celecoxib 200 mg orally once/day has a comparable cardiovascular safety profile to nonselective NSAIDs. It remains unclear whether full-dose celecoxib (200 mg orally 2 times a day ) has cardiovascular risks comparable to the nonselective NSAIDs.
NSAIDs should generally be avoided in patients with previous peptic ulcer disease or dyspepsia; gastric acid suppressive therapy (eg, proton pump inhibitors) should be given to these patients and others at increased risk for gastric ulceration (eg, older adults) if an NSAID is used. Other possible adverse effects of all NSAIDs include headache, confusion and other central nervous system symptoms, increased blood pressure, edema, and decreased platelet function; however, celecoxib has no significant antiplatelet effect. NSAIDs may increase cardiovascular risk (see NSAIDs should generally be avoided in patients with previous peptic ulcer disease or dyspepsia; gastric acid suppressive therapy (eg, proton pump inhibitors) should be given to these patients and others at increased risk for gastric ulceration (eg, older adults) if an NSAID is used. Other possible adverse effects of all NSAIDs include headache, confusion and other central nervous system symptoms, increased blood pressure, edema, and decreased platelet function; however, celecoxib has no significant antiplatelet effect. NSAIDs may increase cardiovascular risk (seeTreatment of Pain/Nonopioid Analgesics). Creatinine levels can rise reversibly because of inhibited renal prostaglandins and reduced renal blood flow; rarely, interstitial nephritis can occur. Patients with urticaria, rhinitis, or asthma caused by aspirin can have the same problems with these other NSAIDs, but celecoxib may not cause these allergic problems.
NSAIDs should be used at the lowest possible dose needed to mitigate their adverse effects.
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
NSAID | Usual Dosage (Oral) | Maximum Recommended Daily Dose |
|---|---|---|
Nonselective NSAIDs | ||
DiclofenacDiclofenac | 75 mg 2 times a day or 50 mg 3 times a day 100 mg once/day sustained-release | 150 mg |
EtodolacEtodolac | 300–500 mg 2 times a day | 1200 mg |
FenoprofenFenoprofen | 300–600 mg 4 times a day | 3200 mg |
FlurbiprofenFlurbiprofen | 100 mg 2 or 3 times a day | 300 mg |
IbuprofenIbuprofen | 400–800 mg 4 times a day | 3200 mg |
IndomethacinIndomethacin | 25 mg 3 to 4 times a day 75 mg 2 times a day sustained-release | 200 mg |
KetoprofenKetoprofen | 50–75 mg 4 times a day 200 mg once/day sustained-release | 300 mg |
Meclofenamate | 50 mg 3 or 4 times a day | 400 mg |
Meloxicam*Meloxicam* | 7.5 mg once/day | 15 mg |
NabumetoneNabumetone | 1000–2000 mg/day in 1 dosage or in divided dosages (500–1000 mg 2 times a day) | 2000 mg |
NaproxenNaproxen | 250–500 mg 2 times a day | 1500 mg |
OxaprozinOxaprozin | 1200 mg once/day | 1800 mg |
PiroxicamPiroxicam | 20 mg once/day | 20 mg |
SulindacSulindac | 150–200 mg 2 times a day | 400 mg |
TolmetinTolmetin | 400 mg 3 times a day | 1800 mg |
Cyclooxygenase-2 (COX-2) selective NSAIDs | ||
CelecoxibCelecoxib | 200 mg once/day or 2 times a day | 400 mg |
* COX-2 specificity is unclear. | ||
Corticosteroids
Systemic corticosteroids decrease inflammation and other symptoms more rapidly than other medications used for rheumatoid arthritis. However, they do not prevent joint destruction, and their clinical benefit often diminishes with time. Furthermore, rebound often follows the withdrawal of corticosteroids in active disease. Because of their long-term adverse effects, corticosteroids are usually given only for short periods of time to maintain function until a DMARD has taken effect.
Corticosteroids may be used for severe joint or systemic manifestations of rheumatoid arthritis (eg, vasculitis, pleurisy, pericarditis). Relative contraindications include peptic ulcer disease, hypertension, untreated infections, diabetes mellitus, and glaucoma. The risk of latent tuberculosis should be considered before corticosteroid therapy is begun.
Intra-articular injections of depot corticosteroids may temporarily help control pain and swelling in particularly painful joints. Triamcinolone hexacetonide may suppress inflammation for the longest time. Triamcinolone acetonide and methylprednisolone acetate are also effective. No single joint should be injected with a corticosteroid more than 3 to 4 times a year, as too-frequent injections may accelerate joint destruction. Because injectable corticosteroid esters are crystalline, local inflammation transiently increases within a few hours in of depot corticosteroids may temporarily help control pain and swelling in particularly painful joints. Triamcinolone hexacetonide may suppress inflammation for the longest time. Triamcinolone acetonide and methylprednisolone acetate are also effective. No single joint should be injected with a corticosteroid more than 3 to 4 times a year, as too-frequent injections may accelerate joint destruction. Because injectable corticosteroid esters are crystalline, local inflammation transiently increases within a few hours in< 2% of patients receiving injections. Although infection is rare, with one study reporting a rate of approximately 1 of 2,000 procedures (10), infection must be considered if pain occurs > 24 hours after injection.
Medications for rheumatoid arthritis references
1. Fraenkel L, Bathon JM, England BR, et al: 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol 73(7):1108-1123, 2021. doi:10.1002/art.41752
2. Smolen JS, Landewé RBM, Bijlsma JWJ, et al: EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis 79(6):685-699, 2020. doi:10.1136/annrheumdis-2019-216655
3. Huscher D, Thiele K, Gromnica-Ihle E, et al: Dose-related patterns of glucocorticoid-induced side effects. Ann Rheum Dis 68(7):1119-1124, 2009. doi:10.1136/ard.2008.092163
4. Moreland LW, O'Dell JR, Paulus HE, et al: A randomized comparative effectiveness study of oral triple therapy versus etanercept plus methotrexate in early aggressive rheumatoid arthritis: the treatment of Early Aggressive Rheumatoid Arthritis Trial. : A randomized comparative effectiveness study of oral triple therapy versus etanercept plus methotrexate in early aggressive rheumatoid arthritis: the treatment of Early Aggressive Rheumatoid Arthritis Trial.Arthritis Rheum. 2012;64(9):2824-2835. doi:10.1002/art.34498
5. O'Dell JR, Haire CE, Erikson N, et al: Treatment of rheumatoid arthritis with methotrexate alone, sulfasalazine and hydroxychloroquine, or a combination of all three medications. : Treatment of rheumatoid arthritis with methotrexate alone, sulfasalazine and hydroxychloroquine, or a combination of all three medications.N Engl J Med 334(20):1287-1291, 1996. doi:10.1056/NEJM199605163342002
6. Sammaritano LR, Bermas BL, Chakravarty EE, et al: 2020 American College of Rheumatology guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Care Res (Hoboken) 72(4):461-488, 2020. doi:10.1002/acr.24130
7. Goodman SM, Springer BD, Chen AF, et al: 2022 American College of Rheumatology/American Association of Hip and Knee Surgeons guideline for the perioperative management of antirheumatic medication in patients with rheumatic diseases undergoing elective total hip or total knee arthroplasty. Arthritis Care Res (Hoboken) 74(9):1399-1408, 2022. doi:10.1002/acr.24893
8. Singh JA, Saag KG, Bridges SL Jr, et al: 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol 68(1):1-26, 2016. doi:10.1002/art.39480
9. Ytterberg SR, Bhatt DL, Mikuls TR, et al: Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med 386(4):316-326, 2022. doi:10.1056/NEJMoa2109927
10. Petersen SK, Hansen I, Andreasen RA: Low frequency of septic arthritis after arthrocentesis and intra-articular glucocorticoid injection. Scand J Rheumatol. 2019;48(5):393-397. doi:10.1080/03009742.2019.1584329
Prognosis for Rheumatoid Arthritis
Rheumatoid arthritis decreases life expectancy; however, this effect on mortality has been decreasing over time and appears to be small. One large cohort study found an excess mortality of only approximately 4 months, which was not apparent until 20 years post-diagnosis (1). Respiratory conditions (eg, interstitial lung disease, pneumonia) were the leading cause of death. Other major causes of excess mortality among patients with rheumatoid arthritis include cardiovascular disease and neoplasms (2). Disease activity should be controlled to lower cardiovascular disease risk in all patients with rheumatoid arthritis. (See also the European League Against Rheumatism's (EULAR) recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders.)
Although the majority of patients experience improvement with treatment, some data suggest that less than half of patients experience sustained remissions (3). At least 10% of patients are eventually severely disabled despite full treatment (4). White people and women have a poorer prognosis, as do patients with subcutaneous nodules, advanced age at disease onset, inflammation in ≥ 20 joints, early erosions, cigarette smoking, high erythrocyte sedimentation rate, and high levels of rheumatoid factor or anticyclic citrullinated peptide (anti-CCP) (5).
Prognosis references
1. Black RJ, Lester S, Tieu J, et al. Mortality estimates and excess mortality in rheumatoid arthritis. Rheumatology (Oxford). 2023;62(11):3576-3583. doi:10.1093/rheumatology/kead106
2. Kerola AM, Kazemi A, Rollefstad S, et al: All-cause and cause-specific mortality in rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis: a nationwide registry study. Rheumatology (Oxford). 2022;61(12):4656-4666. doi:10.1093/rheumatology/keac210
3. Scott IC, Ibrahim F, Panayi G, et al: The frequency of remission and low disease activity in patients with rheumatoid arthritis, and their ability to identify people with low disability and normal quality of life. Semin Arthritis Rheum. 2019;49(1):20-26. doi:10.1016/j.semarthrit.2018.12.006
4. Lacaille D, Sheps S, Spinelli JJ, Chalmers A, Esdaile JM. Identification of modifiable work-related factors that influence the risk of work disability in rheumatoid arthritis. Arthritis Rheum. 2004;51(5):843-852. doi:10.1002/art.20690
5. Albrecht K, Zink A: Poor prognostic factors guiding treatment decisions in rheumatoid arthritis patients: a review of data from randomized clinical trials and cohort studies. Arthritis Res Ther. 2017;19(1):68. Published 2017 Mar 23. doi:10.1186/s13075-017-1266-4
Key Points
Rheumatoid arthritis is a systemic inflammatory disorder.
The most characteristic manifestation is a symmetric polyarthritis involving peripheral joints such as wrists and metacarpophalangeal and metatarsophalangeal joints, often with constitutional symptoms.
Extra-articular findings can include rheumatoid nodules, vasculitis causing leg ulcers or multiple mononeuropathy, pleural or pericardial effusions, pulmonary nodules, pulmonary infiltrates or fibrosis, pericarditis, myocarditis, lymphadenopathy, Felty syndrome, Sjögren syndrome, scleromalacia, and episcleritis.
Radiographs and advanced imaging are helpful, but early diagnosis is primarily by recognizing specific clinical findings and demonstrating abnormal laboratory test results, including autoantibodies (serum rheumatoid factor and anti-cyclic citrullinated peptide antibody) and acute-cell phase reactants (erythrocyte sedimentation rate or C-reactive protein). Diagnosis requires documented joint inflammation and should not be based on laboratory testing alone.
Treat almost all patients aggressively early, primarily with medications that modify disease activity.
Medications that modify disease activity include conventional DMARDs (particularly methotrexate), biologic agents such as tumor necrosis factor (TNF)-inhibitors, and targeted synthetic DMARDs such as tofacitinib.Medications that modify disease activity include conventional DMARDs (particularly methotrexate), biologic agents such as tumor necrosis factor (TNF)-inhibitors, and targeted synthetic DMARDs such as tofacitinib.
Rheumatoid arthritis causes a small decrease in life expectancy (mostly due to respiratory conditions, coronary heart disease, or neoplasms) and causes severe disability in 10% of patients. Control of inflammation and attention to traditional risk factors may reduce the incidence of coronary events.







